Can Pelvic Floor Physiotherapy Prevent Surgery for Pelvic Organ Prolapse?
Yes. Pelvic floor physiotherapy is the primary, non-surgical treatment for pelvic organ prolapse. By structurally rebuilding the pelvic sling, releasing fascial tension, and mastering intra-abdominal pressure, physical therapy significantly reduces prolapse symptoms and frequently prevents the need for reconstructive surgery.
The Silent Epidemic in Women's Health
In Toronto, the physical demands placed on women are immense. Whether navigating the intense recovery period following childbirth, managing the hormonal shifts of menopause, or maintaining a heavy weightlifting routine at a local Queen West gym, the female pelvic floor is subjected to massive, chronic stress.
A deeply distressing and profoundly under-discussed consequence of this stress is Pelvic Organ Prolapse (POP). Women often discover POP subtly—a feeling of "heaviness" or dragging in the lower pelvis after a long day of standing, a sensation of incomplete bladder emptying, or the terrifying discovery of a physical bulge at the vaginal opening.
The traditional medical reflex is often to wait until the prolapse becomes severe enough to warrant complex reconstructive surgery or the permanent placement of a pessary ring. At Rehab Mechanics, our specialized Perinatal and Pelvic Health program categorically rejects this passive "wait and see" approach. The pelvic floor is a dynamic musculoskeletal system. Through highly specialized, trauma-informed physical therapy, we can radically improve the biomechanical support of your pelvic organs, reversing symptoms and restoring your structural confidence.
Structural Analysis: The Mechanics of the Pelvic Floor
To understand how physiotherapy reverses prolapse symptoms, we must perform a detailed biomechanical analysis of the pelvic architecture and the forces that govern it.
The Anatomy of the Pelvic Sling
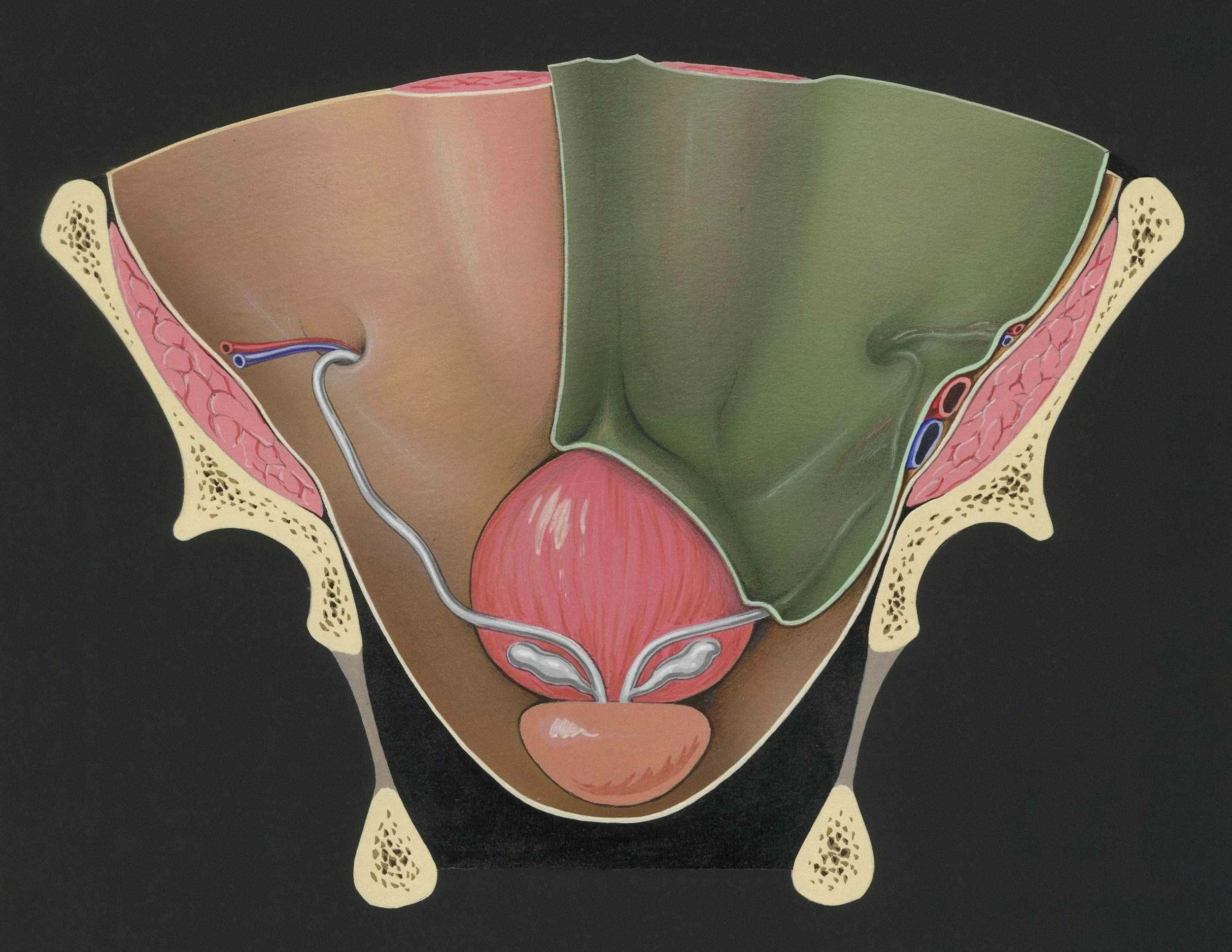
The pelvic floor is an intricate, multi-layered hammock of 14 different muscles, thick fascial sheets, and strong ligaments.
The Structural Floor: This hammock forms the absolute base of your abdominal cavity. It physically spans the gap between your pubic bone in the front and your tailbone in the back.
The Organ Support: Resting directly on top of this muscular sling are your vital pelvic organs: the bladder (anterior), the uterus (central), and the rectum (posterior).
The Pathology of Prolapse
Pelvic Organ Prolapse occurs when this supporting hammock fails, allowing one or more of these organs to drop downward into the vaginal canal.
Cystocele: The bladder drops into the front wall.
Uterine Prolapse: The uterus drops straight down the center.
Rectocele: The rectum bulges into the back wall.
The Two Mechanisms of Failure
The hammock can fail for two very different biomechanical reasons.
1. Fascial Tearing (The Trauma Model)
During a prolonged or mechanically difficult vaginal childbirth, the massive downward pressure can physically stretch or tear the thick connective tissue (the endopelvic fascia) and the levator ani muscles. The hammock loses its structural integrity and sags.
2. The Pressure System Failure (The Chronic Model)
Your core is a sealed, pressurized cylinder. The diaphragm is the roof, the abdominals are the walls, and the pelvic floor is the base.
Intra-Abdominal Pressure (IAP): Every time you cough, sneeze, jump, or lift a heavy barbell, the pressure inside this cylinder spikes massively.
The Downward Crush: If your breathing mechanics are faulty—for example, if you hold your breath and bear down heavily when lifting a car seat—you force 100% of that pressure directly down onto the pelvic organs. Over years, this repetitive, crushing downward force stretches the hammock until the organs drop.
Primary Source Proof: Conservative Pelvic Rehabilitation
Global urogynecology and pelvic health research definitively establishes that highly supervised, specific pelvic floor muscle training is the gold standard for reducing symptom severity and improving the anatomical stage of mild to moderate pelvic organ prolapse.
Review the Clinical Evidence on PubMed: Pelvic Floor Muscle Training for Secondary Prevention of Pelvic Organ Prolapse (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for pelvic health.
The Rehab Mechanics Prolapse Protocol
You cannot fix a prolapse by simply downloading a generic app and doing hundreds of "Kegels." Doing Kegels incorrectly can actually worsen the downward pressure. We use a precise, inside-out "human mechanics" approach.
Phase 1: Advanced Diagnostics and Internal Assessment
We must accurately map the muscular failure.
The Internal Exam: With your strict, ongoing consent, our specialized physiotherapist performs an internal vaginal examination. This allows us to physically palpate the muscles to determine their resting tone, strength, endurance, and to identify the exact organs involved in the prolapse.
Hypertonic vs. Hypotonic: Surprisingly, many women with prolapse actually have overactive (hypertonic) pelvic floors. The muscles are constantly clenched in a state of spasm, making them exhausted and useless when a real pressure spike hits.
Phase 2: Restoring the Cylinder (Pressure Management)
Before we strengthen the floor, we must fix the roof.
Diaphragmatic Integration: We completely retrain your breathing mechanics. We teach you how to breathe laterally into your ribcage so the diaphragm and pelvic floor move in perfect synchrony, like a piston, rather than crashing into each other.
The "Knack": Teaching your nervous system to automatically pre-contract the pelvic floor milliseconds before you cough or lift, proactively shielding the organs from the sudden pressure spike.
Phase 3: Neuromuscular Up-Training and Hypertrophy
If the muscles are weak (hypotonic), we must structurally rebuild their thickness and endurance.
Eccentric and Concentric Loading: We guide you through highly specific, graded contractions of the pelvic sling in various gravity-dependent positions (lying down, seated, and eventually standing).
Endurance Holds: The pelvic floor must be able to hold the organs up for a 14-hour day. We build biological endurance using prolonged, sub-maximal isometric holds.
Phase 4: Functional Loading and Real-World Mechanics
We transition your rehab to match your lifestyle demands.
Symptom-Free Lifting: Integrating your new pelvic floor strength into squats, deadlifts, and functional mom-mechanics (like lifting a toddler from a crib).
Pessary Integration: If conservative therapy requires physical support, our physiotherapists can consult and collaborate on the integration of a vaginal pessary—a soft, removable silicone device that acts like an internal sports bra, physically holding the organs up while we rehabilitate the muscles around it.
Take Back Your Structural Confidence
A diagnosis of Pelvic Organ Prolapse does not mean you have to stop exercising, live with chronic heaviness, or immediately schedule surgery. By mastering your intra-abdominal pressure and deeply rehabilitating your pelvic sling, you can manage the condition and reclaim your active life.
Book a highly confidential, specialized pelvic health assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite, private care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.