Should I See a Physiotherapist Right After a Car Accident?
Yes. You should see a physiotherapist immediately after a car accident. Early intervention prevents acute whiplash and soft tissue damage from becoming chronic pain. A registered physiotherapist will also guide you through Ontario’s complex MVA claims process to ensure your rehabilitation is fully funded.
The Hidden Danger of Low-Speed Collisions
The adrenaline rush immediately following a motor vehicle accident (MVA) often masks the severity of structural injuries. You might walk away from a fender bender on the Gardiner Expressway feeling perfectly fine, only to wake up 48 hours later unable to turn your neck.
Delayed-onset muscle soreness and joint stiffness are the hallmarks of auto collisions. Waiting for the pain to disappear on its own is a critical mistake. Scar tissue forms rapidly. If cervical or lumbar sprains heal in shortened, restricted positions, you are setting the stage for months, or even years, of chronic musculoskeletal dysfunction.
Structural Analysis of Whiplash Associated Disorders (WAD)
Whiplash is not a single injury; it is a mechanism of injury that creates a cascade of structural failures throughout the cervical spine and surrounding tissues.
The Biomechanics of the Impact
During a rear-end collision, your torso is thrust forward while your head remains momentarily static.
Hyperextension Phase: Your neck snaps violently backward. This stretches the anterior longitudinal ligament and crushes the facet joints at the back of the cervical spine.
Hyperflexion Phase: As the vehicle stops, your head is whipped violently forward. This tears the posterior neck muscles, overstretches the spinal cord, and damages the intervertebral discs.
Associated Symptoms Beyond Neck Pain
Because the cervical spine houses critical neurological structures, whiplash often presents with systemic symptoms:
Cervicogenic Headaches: Pain radiating from the base of the skull into the forehead and behind the eyes.
Radiculopathy: Numbness, tingling, or weakness radiating down the shoulders and into the hands.
Vestibular Dysfunction: Dizziness, vertigo, and ringing in the ears (tinnitus).
Navigating Ontario’s MVA Claims Process
In Ontario, your auto insurance provider is required by law to cover the cost of your rehabilitation under the Statutory Accident Benefits Schedule (SABS), regardless of who was at fault. However, navigating the Health Claims for Auto Insurance (HCAI) system is complex.
How Rehab Mechanics Streamlines Your Claim
Our clinical framework encompasses a broad operational spectrum under Ontario's regulatory frameworks.
OCF-18 Treatment Plans: We formulate, submit, and manage standard treatment plans directly through HCAI.
Direct Billing: We coordinate directly with your auto insurer, so you are not left paying out-of-pocket for essential medical care.
Interdisciplinary Care: Located inside the Prime Medical Centre on Abell Street, we work seamlessly alongside medical doctors to ensure your recovery pathway is fully documented and medically supported.
Clinical Intervention: Our Rehabilitation Protocol
Rest is no longer considered the appropriate treatment for whiplash. Prolonged use of cervical collars leads to rapid muscle atrophy.
Phase 1: Acute Inflammation Management: Introducing pain-free micro-movements to prevent scar tissue adhesion.
Phase 2: Restoring Joint Kinematics: Manual mobilizations to restore normal gliding motion to the cervical facet joints.
Phase 3: Work Hardening: Implementing targeted resistance training to rebuild the structural integrity of the upper back and neck for your specific job demands.
Primary Source Proof
Early mobilization and active physical therapy are clinically proven to drastically reduce the incidence of chronic pain following motor vehicle collisions compared to passive rest protocols.
Read the PubMed Evidence: The Efficacy of Early Active Mobilization in Whiplash-Associated Disorders
Do Not Delay Your Assessment
If you have been involved in a motor vehicle accident in Toronto, time is of the essence. Early diagnosis and immediate therapeutic intervention are your best defense against chronic pain.
Book your MVA assessment today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, and our team is ready to guide you through both the physical and administrative hurdles of your recovery.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Do I Absolutely Need Surgery to Fix a Torn Meniscus?
No. The vast majority of degenerative meniscus tears heal entirely without surgery. An aggressive, non-operative physiotherapy protocol of joint unloading, quadriceps strengthening, and neuromuscular retraining stabilizes the knee, permanently eliminates catching pain, and prevents early-onset osteoarthritis.
The Misunderstanding of Knee Cartilage Injuries
An MRI reading of a "torn meniscus" strikes fear into the hearts of active Torontonians. Whether you twisted your knee playing in a recreational soccer league at Lamport Stadium, or simply felt a sharp pop while crouching down to pick up a box in your Queen West apartment, the immediate assumption is that a torn tissue must be surgically cut out or sewn back together.
For decades, orthopedic surgeons routinely performed arthroscopic surgeries to "clean up" torn menisci. However, modern medical imaging and rigorous clinical trials have completely flipped this narrative.
Unless your knee is physically, immovably locked in place, rushing into surgery is often highly detrimental. Removing cartilage rapidly accelerates joint degeneration. At Rehab Mechanics, we prioritize identifying the true biomechanical cause of your knee pain, utilizing advanced conservative rehabilitation to stabilize the joint and save your natural cartilage.
Structural Analysis of the Knee's Shock Absorbers
To understand why conservative physiotherapy is the international standard of care, we must perform a detailed biomechanical analysis of the knee joint and its internal shock absorbers.
The Anatomy of the C-Shaped Cushions
The knee is a massive hinge joint where your thigh bone (femur) rests on top of your shin bone (tibia). Sandwiched between these two bones are two pieces of tough, rubbery fibrocartilage known as the medial (inside) and lateral (outside) menisci.
Mechanical Function: They act as crucial shock absorbers, distributing your body weight evenly across the joint surface and preventing the bones from grinding directly against one another.
The Blood Supply Dilemma (Red Zone vs. White Zone)
The location of the tear dictates the healing potential:
The Red-Red Zone: The outer third of the meniscus has a rich blood supply. Tears here can physically heal and scar back together with proper load management.
The White-White Zone: The inner two-thirds lack a direct blood supply. Tears here will never "knit" back together. However, they do not need to. Physiotherapy trains the surrounding muscles to absorb the shock, rendering the tear entirely asymptomatic.
Identifying the Clinical Red Flags
Meniscus tears present with a highly specific set of mechanical symptoms that differ greatly from standard runner's knee or a basic ligament sprain:
The "Catching" Sensation: A sharp, localized pain when you bend or straighten the knee, feeling as though something is momentarily stuck inside the joint hinge.
Joint Line Tenderness: Pressing your finger precisely into the soft space between the bones on the side of your knee produces exquisite pain.
Delayed Effusion: Unlike an ACL tear which swells instantly, a meniscus tear often causes the knee to slowly puff up with fluid 24 to 48 hours after the initial tweak.
The Physiotherapy Protocol: Bulletproofing the Knee
Our clinical approach focuses strictly on mechanical decompression, reducing joint effusion, and building massive structural support around the damaged cartilage.
1. Joint Decompression and Effusion Management
We cannot build strength if the joint is massively swollen.
Manual Therapy: We use targeted soft tissue release on the calf, hamstring, and IT band to reduce the compressive forces pulling the knee joint tightly together.
Lymphatic Drainage: Utilizing manual techniques to push the stagnant joint fluid (effusion) out of the knee capsule, instantly reducing the feeling of pressure and restoring range of motion.
2. Neuromuscular Quadriceps Reactivation
Swelling inside the knee triggers a reflex that actively shuts down your quadriceps muscle (Arthrogenic Muscle Inhibition).
Isometric Activation: We use pain-free isometric holds and Neuromuscular Electrical Stimulation (NMES) to force the quadriceps to fire, overriding the brain's shutdown signal.
3. Closed Kinetic Chain Strength and Proprioception
We must teach the leg how to absorb gravity without relying on the damaged cartilage.
Gluteal Stabilization: Strengthening the side glutes (gluteus medius) prevents the knee from caving inward (valgus collapse), which is the primary movement that crushes the meniscus.
Proprioceptive Retraining: Utilizing balance boards to retrain the micro-stabilizers in the knee, ensuring the joint reacts instantly to sudden changes in direction.
Primary Source Proof
Massive, landmark orthopedic trials (including the ESCAPE trial) have definitively proven that for degenerative meniscus tears, structured, supervised physical therapy yields pain relief and functional outcomes that are identical to arthroscopic partial meniscectomy surgery, without subjecting the patient to surgical risks.
Read the PubMed Evidence: Physical Therapy versus Arthroscopic Partial Meniscectomy for Meniscal Tears
Save Your Cartilage Today
You do not have to accept an invasive surgery to fix a clicking, painful knee. By aggressively strengthening the muscular scaffolding around the joint, your body can adapt, compensate, and completely resolve the pain of a torn meniscus.
Book your comprehensive knee assessment today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community

Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Fix Pinched Nerves and Radiating Arm Pain?
Yes. Physiotherapy can completely resolve pinched nerves (cervical radiculopathy). A specialized protocol of cervical joint mobilization, deep neck flexor strengthening, and postural correction physically decompresses the cervical spine, eliminating radiating arm pain and preventing permanent disc damage.
The Epidemic of Forward Head Posture in Toronto
Walk into any coffee shop in Queen West, jump on the King streetcar, or look around a downtown creative agency, and you will see the same physical posture: the deep, sustained spinal slump. We are a culture permanently hunched over smartphones, tablets, and multiple monitors.
This modern posture is colloquially known as "Tech Neck." While a stiff neck might seem like a minor annoyance, the long-term biomechanical consequences are severe. When the neck is chronically pushed forward out of its natural alignment, it creates massive structural shearing forces on the delicate cervical vertebrae.
Eventually, this passive stress leads to a catastrophic tissue failure. The pain stops being a dull ache in the neck and suddenly morphs into a terrifying, sharp, burning sensation radiating down your shoulder blade, triceps, and all the way into your fingers. This is cervical radiculopathy—a pinched nerve in the neck. At Rehab Mechanics, we specialize in diagnosing and structurally correcting complex spinal and discogenic pathology without relying on heavy painkillers or invasive injections.
Structural Analysis of the Cervical Spine
To successfully treat radiating arm pain, we cannot just massage the shoulder. We must perform a rigorous biomechanical analysis of the cervical spine to locate exactly where the nerve is being crushed.
The Physics of the Heavy Head
The human head weighs approximately 10 to 12 pounds when perfectly balanced on top of the spine.
The Leverage Effect: For every single inch your head drifts forward past your shoulders to stare at a screen, the mechanical load on your neck muscles and joints essentially doubles.
Chronic Overload: A head jutting three inches forward exerts roughly 40 pounds of pressure on the lower cervical spine. Your neck was not engineered to hold a bowling ball at an angle for eight hours a day.
The Anatomy of a Cervical Disc Bulge
The seven vertebrae of your neck (C1 through C7) are separated by intervertebral discs, which act as crucial shock absorbers.
The Annulus and Nucleus: These discs have a tough, fibrous outer ring (annulus fibrosus) and a soft, gel-like center (nucleus pulposus).
The Tearing Process: The chronic 40-pound pressure of "Tech Neck" unevenly crushes the front of the discs, slowly pushing the gel-like center backward toward the spinal cord. Over time, the outer ring tears, and the gel bulges outward.
Cervical Radiculopathy (The Pinched Nerve)
The space where the nerve roots exit the spine to travel down your arm is incredibly narrow.
Mechanical Strangulation: When a cervical disc bulges backward, it physically invades this narrow space, crushing the nerve root against the bone.
The Symptom Pathway: Because these nerves wire your entire upper extremity, compression at the neck causes severe, shooting pain, numbness, tingling, and profound muscular weakness deep in your arm, forearm, or hand.
Identifying the Clinical Red Flags
Nerve compression in the neck behaves very differently than a standard pulled muscle. If you experience the following, you are dealing with structural nerve impingement:
The "Toothache" in the Arm: A deep, unrelenting, throbbing pain in the shoulder blade or triceps that you cannot rub or stretch away.
Sensory Loss: Your thumb and index finger, or your pinky and ring finger, feel permanently "asleep" or overly sensitive to cold.
Motor Drop: You suddenly cannot perform a push-up, or your arm feels inexplicably heavy when trying to reach overhead to wash your hair.
Relief Posture (Bakody's Sign): You intuitively find that resting your hand on top of your head is the only way to relieve the sharp pain in your arm. (This physically shortens the nerve, taking the tension off the pinched root).
The Physiotherapy Intervention: Decompressing the Spine
At Rehab Mechanics, we reject passive treatments like hot packs for neurological injuries. We utilize a highly aggressive, mechanically driven protocol to centralize the pain (draw it out of the arm and back up to the neck) and retract the bulging disc.
1. Directional Preference Therapy (The McKenzie Method)
Our immediate clinical priority is stopping the nerve compression.
Cervical Retraction: We utilize specific, repeated movements—often cervical retractions (creating a "double chin") and controlled extensions—to physically alter the pressure gradient inside the disc. This mechanical pumping action draws the bulging gel back toward the center, taking it off the nerve root.
Postural Taping: Applying rigid kinesiology tape to the mid-back to act as a physical reminder, preventing you from slumping forward and re-herniating the disc between sessions.
2. Advanced Manual Therapy and Traction
The muscles surrounding a pinched nerve will instantly go into a massive, protective spasm, locking the neck into a rigid block.
Cervical Joint Mobilization: Our Registered Physiotherapists use precise, hands-on Grade II and III glides to free up the stiffened facet joints of the neck, restoring rotational capacity.
Manual Cervical Traction: Gently pulling the head upward to physically separate the cervical vertebrae, instantly opening up the nerve spaces (foramen) and providing immediate, profound relief from the radiating arm pain.
3. Deep Cervical Flexor and Scapular Stabilization
Once the disc is retracted and the nerve is free, we must build the muscular scaffolding necessary to hold your head upright permanently.
Neuromuscular Re-education: The deep muscles at the front of your throat are entirely shut down by tech neck. We prescribe specific, tiny nodding exercises to re-awaken these crucial stabilizers.
Thoracic Extension: Strengthening the mid-back (rhomboids and lower trapezius) to pull the shoulder blades down and back, creating a solid, stable foundation for the neck to rest upon.
Primary Source Proof
Extensive orthopedic research and clinical guidelines confirm that multimodal physiotherapy—combining specific mechanical traction, cervical mobilization, and deep flexor strengthening—is the most highly effective conservative intervention for resolving cervical radiculopathy, frequently outperforming surgical decompression in long-term functional outcomes.
Read the PubMed Evidence: The Efficacy of Conservative Physiotherapy in the Management of Cervical Radiculopathy
Stop Ignoring Your Neck Pain
A stiff neck is a warning sign; radiating arm pain is a structural emergency. Do not wait for a bulging disc to cause permanent nerve damage or muscular atrophy in your arm. Expert, targeted physical rehabilitation can decompress your spine, reverse the damage of tech neck, and restore full feeling and strength to your upper body.
Book your comprehensive spinal assessment today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.

Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does Pain Behind the Kneecap Mean My Cartilage is Gone?
No. Sharp, grinding pain beneath the kneecap is usually Patellofemoral Pain Syndrome, caused by poor mechanical tracking, not necessarily cartilage loss. Physiotherapy permanently resolves this by strengthening weak glutes, correcting foot pronation, and realigning the kneecap to eliminate the bone-on-bone friction.
The Agony of the Subway Stairs
Toronto is a highly vertical city. Whether you are walking down into the depths of a TTC subway station, descending the steep steps of your Queen West apartment, or doing lunges at a local gym, your knees are subjected to immense downward pressure.
For many active urbanites, this daily routine is violently interrupted by a sharp, grinding, or dull aching pain located exactly behind or around the edges of the kneecap. The pain is particularly cruel because it is highly specific: it spikes when walking down stairs, but feels fine walking up. It also creates the classic "movie theater sign," where sitting with your knees bent for a long period (like at a desk or on an airplane) causes a deep, throbbing ache that makes you desperately want to straighten your leg.
When patients experience this "crunching" sensation, they instantly panic, assuming their cartilage has completely worn away and they are doomed to early arthritis (Chondromalacia Patellae). At Rehab Mechanics, we frequently diagnose this as Patellofemoral Pain Syndrome (PFPS), commonly known as Runner's Knee.
The good news is that PFPS is rarely a structural degeneration of the knee itself. It is almost always a biomechanical failure of the hip and foot. By correcting the human mechanics above and below the knee, expert physical therapy can perfectly realign the kneecap and permanently silence the grinding pain.
Structural Analysis: The Mechanics of the Kneecap
To cure Runner's Knee, we must stop looking at the knee in isolation and perform a deep analysis of how the kneecap operates within the entire kinetic chain.
The "Train on the Tracks" Anatomy
Your kneecap (patella) does not float freely. It is a biological pulley embedded inside your massive quadriceps tendon.
The Trochlear Groove: On the front of your thigh bone (femur), there is a V-shaped bony groove.
The Tracking Mechanism: When you bend and straighten your leg, the kneecap is supposed to glide perfectly up and down through the dead-center of this groove, like a train on a track.
The Breakdown: Why the Train Derails
Patellofemoral Pain Syndrome occurs when the kneecap is pulled off-center. Instead of gliding smoothly down the middle of the groove, it violently grinds against the outer bony ridge of the femur.
The Pelvic Drop (The True Culprit)
In 80% of PFPS cases, the knee is actually the innocent victim of a weak hip.
Gluteus Medius Weakness: When you stand on one leg (which happens with every step you take while walking or running), the muscle on the side of your hip (gluteus medius) must fire to keep your pelvis level.
Femoral Internal Rotation: If that hip muscle is weak from sitting at a desk all day, your pelvis drops. This causes your entire thigh bone to collapse and rotate inward (valgus collapse).
The Grinding Friction: While the thigh bone rotates inward, the kneecap is held in place by tight outer leg structures (like the IT band). The result is a massive, highly destructive sheer force that grinds the underside of the kneecap against the femur, inflaming the highly sensitive articular cartilage.
The Foot Foundation (Overpronation)
The problem can also start from the ground up.
If you have flat feet or weak arches (excessive pronation), your foot collapses inward when it strikes the pavement.
This inward collapse violently twists the shin bone (tibia) inward, twisting the knee joint and pulling the kneecap aggressively off its tracking line.
Primary Source Proof: Kinematic Rehabilitation
Orthopedic sports medicine literature emphatically supports the "hip-down" approach, proving that strengthening the posterolateral hip musculature provides significantly faster and more permanent relief for patellofemoral pain than traditional knee-focused exercises.
Review the Clinical Evidence on PubMed: Gluteal Muscle Strengthening for Patellofemoral Pain Syndrome (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for knee rehabilitation.
The Rehab Mechanics Kneecap Tracking Protocol
We do not just ice your knee and give you basic leg lifts. To permanently cure PFPS, we must rewire the biomechanics of your entire lower body.
Phase 1: Pain Modulation and Tissue Release (Weeks 1-3)
Before we can build strength, we must release the tight structures that are physically pulling the kneecap off-center.
IT Band and Lateral Retinaculum Release: Our physiotherapists use advanced, deep myofascial release on the outside of the thigh (TFL and vastus lateralis). By loosening these extremely tight structures, we instantly provide mechanical slack, allowing the kneecap to drift back toward the center of the groove.
Patellar Taping (McConnell Taping): We apply rigid kinesiology tape directly over the kneecap, physically taping it into the center of the groove. This mechanically unloads the inflamed tissue and allows you to walk down stairs pain-free while we rehabilitate the muscles.
Phase 2: Hip Isolation and Foundation Fortification (Weeks 4-6)
We must build the muscular scaffolding that prevents the thigh bone from collapsing inward.
Isolated Gluteal Activation: Utilizing targeted, side-lying hip abductions, banded clamshells, and isometric holds to wake up the dormant lateral stabilizers of the pelvis.
VMO Retraining: We use specific biofeedback to teach your brain to fire the vastus medialis oblique (the teardrop-shaped muscle on the inside of the knee) earlier in the movement cycle, actively pulling the kneecap inward against the lateral friction.
Phase 3: Dynamic Integration and Gait Retraining (Weeks 6-10)
Strength on a treatment table means nothing if it doesn't translate to the sidewalk.
Anti-Valgus Training: We progress to dynamic step-downs, lateral lunges, and single-leg squats while utilizing tactile feedback (like a resistance band pulling the knee inward) to force your brain to consciously fire the glutes and push the knee straight.
Foot Mechanics Check: If structural overpronation is driving the knee pain, Sanjay is qualified to assess and dispense custom medical orthotics to permanently support the arch and align the shin bone.
Silence the Grinding Joint
You do not have to live with the fear of stairs or the chronic, aching pain of runner's knee. By identifying and correcting the foundational biomechanics of your hips and feet, physical therapy offers a permanent, non-surgical solution to patellofemoral pain.
Book a comprehensive biomechanical knee assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.

Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.


Will Foam Rolling Fix My IT Band Syndrome and Outer Knee Pain?
No. Foam rolling cannot physically stretch the IT band. Physiotherapy cures IT band syndrome by addressing the root biomechanical cause: weak gluteal muscles and pelvic drop. Strengthening your lateral hip stabilizers stops the mechanical compression causing your severe outer knee pain.
The Runner's Worst Nightmare in Toronto
For the thousands of runners and cyclists navigating the Martin Goodman Trail or the hills of High Park, outer knee pain is an incredibly prevalent and devastating issue. You start your run feeling fantastic, but by kilometer four, a sharp, stabbing, and burning pain develops on the exact outside edge of your knee. It becomes so severe that you are forced to stop and limp home.
This condition is widely known as Iliotibial (IT) Band Syndrome. If you visit a standard walk-in clinic or browse generic fitness forums, the advice is almost unanimously the same: "Your IT band is tight. You need to stretch it and foam roll it."
Patients will spend agonizing hours grinding a hard foam roller up and down their outer thigh, bruising their tissue and screaming in pain, only to find that their knee hurts exactly the same amount on their next run.
At Rehab Mechanics in Queen West, we specialize in advanced sports biomechanics. We know that the IT band is not a muscle, and therefore, it cannot be "tight" or "stretched." IT Band Syndrome is a profound failure of hip stabilization. To permanently cure the knee pain, we must put away the foam roller and rebuild the mechanical foundation of your pelvis.
Structural Analysis: The Mechanics of the Iliotibial Band

To understand why stretching fails, we must perform a detailed anatomical analysis of what the IT band actually is and how it functions under the heavy load of running.
The Anatomy of the IT Band
The Iliotibial Band is not a muscle. It is a massive, incredibly thick strip of fascial connective tissue.
The Tensile Strength: Research shows that the IT band possesses the tensile strength of soft steel. It takes thousands of pounds of force to stretch it even a millimeter. This is why foam rolling is biologically useless for "lengthening" the band; you are simply bruising the skin and muscles underneath it.
The Anchors: The IT band originates at your hip, attaching to two specific muscles: the Tensor Fasciae Latae (TFL) in the front, and the Gluteus Maximus in the back. It then runs all the way down your outer thigh and anchors into the tibia (shin bone) just below the knee.
The Pathology of Outer Knee Pain
For decades, sports medicine believed IT band syndrome was a "friction" issue—that the band was snapping back and forth over the bony bump on the outside of the knee (the lateral epicondyle). Modern medical imaging has disproven this.
The Compression Model
IT Band Syndrome is not a friction problem; it is a highly localized compression problem.
The Fat Pad: Situated directly underneath the IT band at the outer knee is a highly innervated, highly vascularized layer of fat and connective tissue.
The Squeeze: When the biomechanics of the leg fail, the IT band acts like a tight tourniquet. It violently bows inward and crushes this highly sensitive fat pad against the bone with every single foot strike. This severe crushing is what causes the sharp, burning, debilitating pain.
The Biomechanical Trigger: Pelvic Drop
If the IT band is crushing the knee, why is it so tight? The answer lies at the opposite end of the band: your hip.
Gluteus Medius Weakness
When you run, you spend the entire time balancing on one leg. The gluteus medius (the muscle on the side of your hip) is responsible for keeping your pelvis level.
The Trendelenburg Gait: If you have a weak gluteus medius due to sitting at a desk all day, your pelvis will drop on the opposite side every time your foot hits the pavement.
The Whiplash Effect: When the pelvis drops, the femur (thigh bone) violently shifts and rotates inward. Because the IT band is attached to the hip and the knee, this inward collapse aggressively yanks the band taut, forcing it to compress the delicate fat pad at the knee.
To fix the knee, you must stop the pelvis from dropping.
Primary Source Proof: Kinematic Rehabilitation
Advanced orthopedic and sports medicine literature definitively proves that IT band syndrome is driven by hip abductor weakness, and that targeted pelvic stabilization is vastly superior to localized knee treatments or fascial stretching.
Review the Clinical Evidence on PubMed: Hip Abductor Weakness in Distance Runners with Iliotibial Band Syndrome (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for sports rehabilitation.
The Rehab Mechanics Corrective Protocol
We treat IT Band Syndrome by entirely revamping your running mechanics and building an indestructible pelvic foundation.
Phase 1: Calming the Compression (Weeks 1-3)
We must immediately stop the fat pad from being crushed.
Activity Modification: We implement a temporary halt to running on sloped or cambered surfaces (which aggressively drops the pelvis) and reduce weekly mileage to sub-symptom levels.
Soft Tissue De-Tethering: We do not roll the IT band. Instead, our physiotherapists use advanced manual therapy to strip the TFL and Gluteus Maximus muscles at the top of the hip. By releasing the muscular anchors, we introduce structural slack into the band itself.
Phase 2: Neuromuscular Hip Isolation (Weeks 3-6)
We must wake up the sleeping lateral stabilizers.
Glute Medius Activation: Utilizing highly isolated, side-lying movements (like clam shells with resistance bands and strict hip abductions). We use tactile feedback to ensure you are firing the glute and not compensating with the lower back.
Isometric Loading: Using heavy, static holds against the wall to train the gluteus medius to contract continuously, simulating the sustained effort required during a long run.
Phase 3: Dynamic Pelvic Control and Gait Retraining (Weeks 6-10)
Strength on a treatment table means nothing if it doesn't translate to the pavement.
Closed Kinetic Chain Integration: We progress to dynamic step-downs, single-leg deadlifts, and lateral lunges. We meticulously monitor your knee tracking to ensure the glute fires instantly, preventing the femur from rotating inward.
Cadence Manipulation: We may analyze your running gait on a treadmill. Increasing your step rate (cadence) by just 5% to 10% drastically reduces the impact force and limits the amount of time the pelvis has to drop, providing massive relief to the outer knee.
Run Without Limits
You do not have to abandon your marathon goals or suffer through agonizing foam rolling sessions. By correcting the structural biomechanics of your pelvis and hips, you can permanently eliminate the compressive forces causing your knee pain.
Book a comprehensive sports biomechanics assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite running rehabilitation in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is My Inner Knee Pain a Meniscus Tear or Just Bursitis?
Maybe. While meniscus tears cause joint clicking and pain directly on the joint line, sharp inner knee pain below the joint is often pes anserine bursitis. Physiotherapy resolves both by correcting pelvic mechanics, releasing hyperactive hamstrings, and strengthening glutes to eliminate structural friction.
The Diagnostic Confusion of Medial Knee Pain
For the runners, cyclists, and weekend warriors navigating the paths of Trinity Bellwoods and the Martin Goodman Trail, knee pain is a persistent threat. When a sharp, stinging pain develops on the inside (medial) aspect of the knee, panic often ensues.
Athletes immediately jump to the worst-case scenario: "I've torn my medial meniscus" or "I've blown my MCL." They expect to be scheduled for an MRI and placed on a surgical waitlist. However, at Rehab Mechanics in Queen West, we frequently uncover a highly treatable, yet massively misunderstood, biomechanical culprit: Pes Anserine Bursitis.
While a meniscus tear happens deep inside the joint capsule, pes anserine bursitis happens outside the joint, roughly two to three inches below the actual knee hinge. It is a severe, friction-based inflammatory condition. When you understand that this condition is not a structural tear of cartilage, but rather a functional failure of your hip and thigh muscles, the path to a full, non-surgical recovery becomes clear. Through advanced human mechanics physical therapy, we can stop the friction and permanently eliminate the inner knee pain.
Structural Analysis: The Mechanics of the "Goose Foot"
To accurately diagnose and treat this condition, we must perform a detailed structural analysis of the medial knee architecture and the specific tendons that anchor there.
The Anatomy of the Pes Anserinus
"Pes Anserinus" is Latin for "goose foot." It refers to the webbed, three-pronged shape of three specific muscle tendons as they merge and attach to the inside of your shin bone (tibia), just below the knee joint.
The Three Muscles: These tendons belong to the Sartorius (front of the thigh), the Gracilis (inner thigh/groin), and the Semitendinosus (inner hamstring).
The Anchor Point: Together, they act as massive, dynamic stabilizers, preventing your lower leg from twisting outward during running and pivoting.
The Bursa Sac: Sitting directly underneath this three-pronged tendon attachment, protecting it from grinding against the hard shin bone, is the pes anserine bursa—a fluid-filled, friction-reducing sac.
The Pathology of Friction (Bursitis)
Bursitis is not a random occurrence; it is a mechanical penalty for poor movement patterns.
The Valgus Collapse Trigger
If your pelvic mechanics are faulty, your knee pays the price.
Gluteus Medius Weakness: When you run, you spend the entire time balancing on one leg. If the muscle on the side of your hip (gluteus medius) is weak from sitting at a desk all day, your pelvis drops.
The Inward Cave: This pelvic drop forces your thigh bone to violently rotate inward, causing your knee to collapse toward your midline (a movement called knee valgus).
The Whiplash Effect: Every time your knee caves inward, the three tendons of the pes anserinus are violently yanked taut against the bone to stop the collapse.
The Inflammatory Crush: This relentless, repetitive yanking physically crushes the bursa sac underneath the tendons. The bursa becomes engorged, swollen, and excruciatingly painful, making it impossible to walk down stairs or run without a sharp, stabbing sensation.
Identifying the Clinical Red Flags: Bursitis vs. Meniscus
How do we differentiate pes anserine bursitis from a torn meniscus or ligament sprain?
The Location: Meniscus pain is felt directly on the joint line (the space between the femur and tibia). Pes anserine pain is felt exactly 2 to 3 inches below the joint line, on the flat part of the inner shin bone.
The Touch Test: Pressing your finger directly onto that spot below the joint line produces a breathtaking, exquisite point-tenderness.
The Stair Trigger: The pain is uniquely severe when descending stairs or stepping down off a Toronto streetcar, as this requires massive eccentric hamstring control, which crushes the inflamed bursa.
Absence of Locking: Unlike a meniscus tear, the knee does not physically "lock," "catch," or click. The hinge works fine; the pain is purely superficial.

Primary Source Proof: Biomechanical Knee Rehabilitation
Orthopedic and sports medicine literature dictates that correcting lumbo-pelvic kinematics and strengthening the hip abductors is the definitive, long-term solution for resolving medial knee overuse injuries like pes anserine bursitis, vastly outperforming localized rest or cortisone injections.
Review the Clinical Evidence on PubMed: The Role of Hip Muscle Function in the Treatment of Patellofemoral and Medial Knee Pain (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for sports rehabilitation.
The Rehab Mechanics Corrective Protocol
We do not just ice the knee. To cure this condition, we must physically alter the angle of your leg during movement.
Phase 1: Tendon Desensitization and Inflammation Control (Weeks 1-3)
We must immediately stop the mechanical crushing of the bursa.
Activity Modification: A temporary halt on running and stair-climbing workouts to allow the swollen bursa sac to chemically cool down.
Advanced Myofascial Release: Our physiotherapists apply targeted, deep manual therapy to the bellies of the hamstring, gracilis, and sartorius muscles high up in the thigh. Releasing the tension at the top of the muscles instantly provides mechanical slack to the tendons at the knee.
Kinesiology Taping: Utilizing strategic taping patterns to gently lift the skin and fascia over the medial knee, decompressing the inflamed bursa and providing immediate pain relief during walking.
Phase 2: Pelvic Fortification and Neuromuscular Control (Weeks 4-6)
We must build the muscular scaffolding that prevents the knee from caving inward.
Isolated Glute Medius Activation: Utilizing side-lying hip abductions, banded clamshells, and isometric wall holds to wake up the lateral stabilizers of the pelvis.
Eccentric Hamstring Loading: Tendons need strength to handle force without spasming. We use slow, controlled hamstring curls and sliders to build robust resilience in the semitendinosus tendon so it no longer crushes the bursa.
Phase 3: Dynamic Integration and Gait Retraining (Weeks 6-8+)
We must ensure your new hip strength translates to the pavement.
Anti-Valgus Training: We progress to dynamic step-downs, lateral lunges, and single-leg squats while utilizing tactile feedback (like a resistance band pulling the knee inward) to force your brain to consciously fire the glutes and push the knee straight.
Cadence Manipulation for Runners: If running is your goal, we may analyze your gait and increase your step cadence by 5-10%. Taking slightly shorter, faster steps drastically reduces the heavy, bounding impact that triggers the valgus collapse.
Stop the Friction, Save Your Knee
You do not have to live with stinging inner knee pain or fear that you have a torn meniscus. By addressing the deep biomechanics of your hip and thigh, physical therapy offers a permanent, non-surgical solution to pes anserine bursitis.
Book a comprehensive biomechanical knee assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Are Your Chronic Migraines Actually Being Caused by Your Neck?
Yes. Many chronic headaches misdiagnosed as migraines are actually cervicogenic headaches. Physiotherapy cures this by mobilizing the stiff upper cervical joints and releasing suboccipital spasms, cutting off the faulty nerve signals that project severe pain from the neck into the forehead and eyes.
The Daily Battle with Head Pain
In the intense, screen-dominated work environments of Toronto's Financial District and Queen West, chronic headaches are an epidemic. Countless professionals wake up daily with a dull, throbbing pressure wrapping around their temples, an agonizing tightness at the base of the skull, or sharp, piercing pain radiating directly behind one eye.
The typical medical route involves consulting a family doctor, receiving a diagnosis of "migraines" or "tension headaches," and being prescribed heavy medications like triptans or muscle relaxants. While these drugs may temporarily numb the pain, they do absolutely nothing to address the structural root cause. The headaches inevitably return the next day.
At Rehab Mechanics, we frequently encounter patients who have suffered for years under the false assumption that their brain chemistry is to blame. In reality, a massive percentage of these "migraines" are mechanical. They are Cervicogenic Headaches—meaning the pain originates in the structures of the neck. By overhauling your cervical biomechanics and correcting "Tech Neck," specialized physiotherapy can permanently turn off the headache alarm without a single pill.
Structural Analysis: The Mechanics of Referred Head Pain
To understand how a problem in your neck creates blinding pain in your forehead, we must perform a detailed biomechanical and neurological analysis of the upper cervical spine.
The Cervical Foundation
The human head weighs approximately 10 to 12 pounds. It balances on the top three vertebrae of your neck: the Atlas (C1), the Axis (C2), and C3.
The Suboccipital Muscles: A dense cluster of four tiny muscles connects the base of your skull to these top vertebrae. Their primary job is to hold your head level and coordinate eye movements.
The Biomechanical Collapse (Tech Neck)
When you sit hunched over a laptop or stare down at your phone for eight hours a day, your head translates forward.
The Leverage Crisis: For every inch your head moves forward, the functional weight on your neck muscles doubles.
The Spasm: To stop your 30-pound head from falling onto your chest, the suboccipital muscles must lock into a severe, chronic spasm. The joints of the upper neck (the facet joints) become violently compressed and jammed.
The Neurological Bridge (The TCN)
Why does a jammed neck joint cause pain behind your eye? The answer lies in a neurological phenomenon called "referred pain," driven by a specific relay station in your brainstem.
The Trigeminal-Cervical Nucleus (TCN): The nerves that supply sensation to the upper neck joints (C1-C3) merge into the TCN.
The Shared Pathway: Crucially, the Trigeminal Nerve—which supplies sensation to your forehead, temples, jaw, and face—also plugs into this exact same relay station.
The Sensory Confusion: When the joints in your upper neck are mechanically crushed and inflamed, they flood the TCN with danger signals. The brain is overwhelmed by this data and misinterprets the origin of the pain, projecting the agony forward into the head and face.
Identifying the Clinical Red Flags: Cervicogenic vs. Migraine
Proper differential diagnosis is essential. We look for specific mechanical clues that prove the neck is the true culprit.
Unilateral Pain: Cervicogenic headaches almost always affect only one side of the head and neck, whereas true tension headaches usually wrap around both sides like a tight band.
Movement Triggers: The headache spikes or can be actively reproduced by moving the neck (e.g., looking up at the ceiling or turning to check a blind spot). True migraines are typically triggered by chemical factors (hormones, food, light) rather than mechanical movement.
The "Base of the Skull" Anchor: The pain almost always starts as a stiff, deep ache at the very base of the skull before wrapping over the top of the head toward the eye.
Primary Source Proof: Cervicogenic Decompression
Clinical neurology and physical therapy research heavily dictates that targeted manual mobilization of the cervical spine combined with deep neck flexor strengthening is the most effective intervention for eradicating cervicogenic headaches, vastly outperforming pharmacological management.
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for neurological rehabilitation.
The Rehab Mechanics Eradication Protocol
We do not just massage the neck. We systematically decompress the neurological bottleneck and rebuild your postural endurance.
Phase 1: Neurological Decompression (Weeks 1-3)
Our immediate goal is to un-jam the upper neck joints to stop the faulty nerve signals flooding the brainstem.
Sustained Natural Apophyseal Glides (SNAGs): Our physiotherapists use precise, gentle Grade II and III manual mobilizations to physically free the stiff C1, C2, and C3 vertebrae, restoring their micro-gliding motion.
Suboccipital Release: We apply targeted, deep ischemic compression directly into the base of the skull to melt away the rigid muscle spasms that are compressing the nerves.
Phase 2: Restoring the Foundation (Weeks 3-6)
Your neck cannot sit straight if your mid-back is hunched over.
Thoracic Spine Unlocking: Utilizing high-grade joint manipulations to forcefully restore thoracic extension (the ability to arch the mid-back backward). This stops the neck from having to hyper-extend to see the computer screen.
Pectoral Myofascial Release: Lengthening the tight chest muscles that are physically dragging the shoulders forward.
Phase 3: Deep Cervical Fortification (Weeks 6+)
We must build the biological endurance necessary to hold your head perfectly balanced for an entire workday.
Deep Cervical Flexor (DCF) Activation: We use specific biofeedback drills (like micro-chin tucks) to wake up the tiny muscles in the front of your throat. When these muscles fire, they automatically pull the head back over the shoulders, permanently turning off the emergency spasms in the suboccipital muscles.
Scapular Retraction: Implementing heavy rows and prone Y-raises to strengthen the mid-back, physically anchoring the shoulders down and away from the ears.
Turn Off the Headache Alarm
You do not have to accept daily headaches or rely on a permanent supply of painkillers. By identifying the mechanical failures in your cervical spine and rebuilding your postural endurance, you can permanently eradicate the pain.
Book a comprehensive neurological and biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does Numbness in Your Pinky Finger Mean You Have Cubital Tunnel Syndrome?
Yes. Numbness isolated to the pinky and ring fingers strongly indicates Cubital Tunnel Syndrome (ulnar nerve entrapment). Physiotherapy permanently resolves this by utilizing targeted nerve gliding, releasing the flexor carpi ulnaris, and correcting workstation ergonomics to decompress the nerve without surgery.
The "Funny Bone" That Isn't So Funny
For the massive population of remote workers, software engineers, and gamers living in Toronto’s Queen West and Liberty Village neighborhoods, upper extremity nerve pain is an epidemic.
Many patients walk into Rehab Mechanics complaining of a strange, deeply unsettling sensation: their pinky finger and the outer half of their ring finger feel permanently "asleep," accompanied by a burning, electrical ache on the inside of their elbow. Because they type all day, they immediately assume they have developed Carpal Tunnel Syndrome.
However, Carpal Tunnel Syndrome affects the thumb and index fingers. When the numbness is strictly isolated to the pinky side of the hand, the problem is entirely different. You are dealing with Cubital Tunnel Syndrome—a severe mechanical entrapment of the ulnar nerve at the elbow joint.
Often triggered by sitting with your elbows bent tightly at a desk or leaning heavily on hard armrests for hours, this condition can rapidly progress from a mild annoyance to profound hand weakness and muscle wasting. At Rehab Mechanics, we specialize in advanced neurodynamics. We can physically decompress the ulnar nerve, restore its sliding mobility, and save you from invasive elbow surgery.
Structural Analysis: The Mechanics of Ulnar Nerve Entrapment

To effectively cure Cubital Tunnel Syndrome, we must perform a detailed biomechanical analysis of the ulnar nerve's pathway and the exact anatomical bottleneck where it gets crushed.
The Anatomy of the Cubital Tunnel
The ulnar nerve originates in the cervical spine (neck), travels down the arm, and must cross the elbow joint to reach the hand.
The Anatomical Bottleneck: As it crosses the elbow, the nerve runs through a very narrow, bony groove on the inside of the joint, situated directly behind the medial epicondyle (the bony bump on the inner elbow).
Osborne’s Ligament: This groove forms the "cubital tunnel." The roof of the tunnel is a thick band of tissue called Osborne’s ligament, which traps the nerve tightly against the bone.
The "Funny Bone": Because the nerve runs so close to the surface here, hitting this specific spot causes a massive electrical shock down the arm—the classic "funny bone" reaction.

The Biomechanics of Nerve Strangulation
Nerves are designed to stretch and slide, but they absolutely cannot tolerate sustained compression or extreme traction.
The Traction Squeeze (Elbow Flexion)
The primary driver of Cubital Tunnel Syndrome is prolonged elbow flexion (bending the elbow past 90 degrees).
The Desk Worker Trap: Typing on a keyboard with your elbows tucked tightly, or sleeping with your arms curled tightly up to your chest (fetal position), violently stretches the ulnar nerve tightly around the medial epicondyle.
The Volume Drop: When you bend your elbow fully, the physical volume (space) inside the cubital tunnel drops by over 50%. The nerve is aggressively stretched and simultaneously crushed by the narrowing tunnel.

The Friction Squeeze (External Compression)
The Armrest Trap: Leaning your inner elbow heavily on a hard plastic office chair armrest or a desk edge applies direct, ischemic (blood-starving) compression to the nerve.
The Result: The nerve becomes inflamed, swollen, and choked. Because the tunnel is rigid, the swollen nerve becomes trapped, leading to severe numbness in the hand and a sharp loss of grip strength.
Identifying the Clinical Red Flags
Cubital Tunnel Syndrome requires immediate intervention before permanent nerve damage occurs. We look for highly specific clinical signs:
The Pinky Split: Numbness and tingling that specifically affects the pinky finger and exactly half of the ring finger.
Tinel's Sign: Tapping lightly on the inside of the elbow sends an immediate, highly irritable electrical shock shooting down into the hand.
Wartenberg's Sign: In advanced cases, the muscles in the hand become so weak that the pinky finger naturally drifts outward and cannot be pulled tightly against the other fingers.
Froment's Sign: A visible inability to pinch a piece of paper tightly between the thumb and index finger without the thumb aggressively bending at the knuckle to compensate for weak hand muscles.
Primary Source Proof: Conservative Nerve Decompression

Clinical neurology and upper extremity orthopedic research universally supports conservative physiotherapy—specifically neurodynamic gliding and nocturnal splinting—as the highly effective, first-line standard of care for resolving mild to moderate Cubital Tunnel Syndrome.
Review the Clinical Evidence on PubMed: The Effectiveness of Conservative Treatment and Neurodynamic Mobilization in Cubital Tunnel Syndrome (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for nerve entrapment rehabilitation.
The Rehab Mechanics Decompression Protocol
Treating an entrapped nerve requires absolute mechanical precision. You cannot aggressively stretch an inflamed nerve, as pulling on it will only trigger a massive pain flare-up. We must utilize targeted "remedial mechanics" to create space and restore nerve glide.
Phase 1: Acute Decompression and Splinting (Weeks 1-3)
Our absolute first priority is stopping the mechanical crushing of the nerve.
Nocturnal Extension Splinting: You spend a third of your life asleep, often with your elbows tightly curled. We utilize specialized night splints that keep the elbow locked at a safe, neutral angle (roughly 45 degrees), preventing the nocturnal strangulation that causes you to wake up with dead hands.
Ergonomic Overhaul: We provide strict, actionable coaching to eliminate the "armrest trap" at your desk and optimize your keyboard position to prevent extreme elbow flexion during the 10-hour workday.
Phase 2: Neural Mobilization (Flossing)
Nerves must be able to slide smoothly through their anatomical tunnels.
Ulnar Nerve Gliding (Neurodynamics): When compressed for months, the ulnar nerve gets "stuck" to the surrounding tissue with microscopic scar tissue. We prescribe highly specific, gentle "flossing" movements that systematically tug the nerve back and forth through the cubital tunnel. This breaks the fibrotic adhesions and restores the nerve's slippery mobility without overstretching it.
Phase 3: Soft Tissue Unlocking and Double Crush Prevention
We must release the surrounding muscular "brakes" that are pulling on the elbow joint.
Flexor Carpi Ulnaris (FCU) Release: The ulnar nerve dives directly into the FCU muscle in the forearm after leaving the elbow. If this muscle is locked in a tight spasm from heavy typing, it creates a secondary crush point. We use deep instrument-assisted soft tissue mobilization (IASTM) to melt this tension.
Cervical Spine Screening: Nerves originate in the neck. We meticulously screen your cervical spine to ensure a bulging disc or "Tech Neck" posture is not creating a primary pinch at the nerve root (Double Crush Syndrome).
Restore Feeling to Your Hands
You do not have to live with numb fingers, dropping coffee mugs, or the looming threat of invasive ulnar nerve transposition surgery. By identifying the mechanical bottlenecks and actively restoring the nerve's sliding capacity, physiotherapy can completely resolve Cubital Tunnel Syndrome.
Book a comprehensive neurological and biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is My Numb Arm Caused by Thoracic Outlet Syndrome or a Pinched Nerve?
Yes. Thoracic Outlet Syndrome causes severe arm numbness by physically crushing the brachial plexus nerves between the collarbone and first rib. Physiotherapy permanently resolves this by mobilizing the first rib, releasing the scalene muscles, and restoring proper scapular mechanics to decompress the nerves.
The Mystery of the "Dead Arm"
For the thousands of professionals working in Toronto’s tech and financial sectors, spending ten to twelve hours a day hunched over a laptop is standard practice. Over time, many of these workers develop a deeply frightening symptom profile: a heavy, aching pain in the base of the neck accompanied by numbness, tingling, or a "pins and needles" sensation shooting all the way down their arm and into their pinky and ring fingers.
When patients visit a standard walk-in clinic, this is almost always misdiagnosed as Carpal Tunnel Syndrome or a herniated cervical disc. Patients are given wrist braces or neck traction devices, yet the numbness persists or worsens when they try to lift their arms overhead to wash their hair or sleep.
Why do these treatments fail? Because the nerve is not being pinched in the wrist or the spine. It is being violently crushed in the crowded anatomical intersection between your neck and your shoulder—a condition known as Thoracic Outlet Syndrome (TOS).

At Rehab Mechanics in Queen West, we specialize in complex neurological and biomechanical mapping. We do not just guess where your nerve is pinched; we systematically trace the mechanical bottlenecks to physically un-trap the nerve, saving you from unnecessary anxiety and invasive surgical consultations.
Structural Analysis: The Anatomy of the Thoracic Outlet
To cure TOS, we must perform a detailed biomechanical analysis of the "thoracic outlet"—the narrow, highly congested physical passageway that vital nerves and blood vessels must navigate to reach your arm.
The Brachial Plexus
The nerves that power your arm and hand exit the spinal cord in your neck and weave together into a massive, thick cable called the brachial plexus. To get to your arm, this cable must thread the needle through three distinct, dangerous bottlenecks.
1. The Scalene Triangle

Your scalene muscles run from the side of your neck down to your very first rib. The brachial plexus must pass directly between the anterior and middle scalene muscles.
The Postural Trap: If you suffer from "Tech Neck" (forward head posture), these scalene muscles must work in constant overdrive to hold your heavy head up.
The Strangulation: They become massively hypertrophied (thickened) and locked in spasm, acting like a tight vice grip that crushes the nerve bundle against the top of the first rib.
2. The Costoclavicular Space
This is the tiny, bony gap between your collarbone (clavicle) and your first rib.
The Postural Trap: Carrying heavy laptop bags on the TTC, or simply living with a rounded, slouched posture, causes your shoulder blades to roll forward and your collarbone to drop downward.
The Strangulation: The heavy collarbone drops like a ceiling directly onto the first rib, physically pinning and crushing the brachial plexus and the subclavian artery. This causes the arm to feel "heavy," cold, or completely dead.
3. The Pectoralis Minor Space
After surviving the collarbone, the nerves must run directly underneath the pectoralis minor muscle on the front of your chest.
The Strangulation: A tight, shortened chest muscle acts like a tourniquet. Every time you reach your arm overhead, the pec minor violently stretches tight, cutting off the nerve signals and blood flow to the arm.
Identifying the Clinical Red Flags
Thoracic Outlet Syndrome presents with highly specific symptoms that differentiate it from a simple pinched neck nerve or carpal tunnel.
The Overhead "Dead Arm": Holding your arms overhead (like blow-drying your hair or hanging curtains) causes the arm to rapidly fatigue, ache profoundly, or go completely numb.
The Ulnar Distribution: The tingling is usually most severe in the pinky and ring fingers, tracing up the inside of the forearm.
Aching Collarbone: A dull, deep, unrelenting ache located right at the base of the neck, deep behind the collarbone.
Vascular Symptoms: In rare but severe cases, the arm may actually change color (turning pale or bluish) or feel noticeably colder than the other arm due to compromised blood flow.
Primary Source Proof: Non-Operative Decompression
Clinical neurology and orthopedic literature confirm that targeted, conservative physiotherapy focusing on muscular release, first rib mobilization, and postural restoration is the highly effective, first-line standard of care for neurogenic Thoracic Outlet Syndrome.
Review the Clinical Evidence on PubMed: Conservative Management and Physiotherapy for Neurogenic Thoracic Outlet Syndrome (National Institutes of Health)
The Rehab Mechanics TOS Decompression Protocol
Treating TOS requires absolute precision. We cannot use generic neck stretches, as aggressively pulling on an already-crushed nerve will only increase the burning pain. We must physically decompress the bottlenecks.
Phase 1: Advanced Decompression and Manual Therapy (Weeks 1-4)
Before we can correct posture, we must manually open the thoracic outlet.
First Rib Mobilization: Our Registered Physiotherapists use precise, downward manual pressure to mobilize an elevated, stuck first rib. Dropping this rib instantly creates massive physical space for the nerves to breathe.
Scalene and Pec Minor Release: Utilizing intensive soft tissue mobilization and ischemic compression to melt away the dense spasms in the neck and chest muscles that are strangulating the brachial plexus.
Diaphragmatic Breathing Integration: The scalene muscles are secondary breathing muscles. We teach you how to breathe deeply using your diaphragm to stop the scalenes from overworking and spasming with every breath you take.
Phase 2: Neurodynamic Flossing (Weeks 3-6)
Nerves need to slide smoothly to stay healthy.
Nerve Gliding: When compressed for months, the brachial plexus gets stuck in microscopic scar tissue. We prescribe specific, gentle "flossing" movements that tug the nerve back and forth through the thoracic outlet, breaking the adhesions and restoring its slippery mobility.
Phase 3: Scapular and Cervical Fortification (Weeks 6+)
This is the permanent cure. We must rebuild the muscular scaffolding that holds your collarbone and shoulders in a neutral, open position.
Lower Trapezius and Serratus Activation: Implementing heavy, targeted rows and prone Y-raises to strengthen the mid-back. These muscles physically pull the shoulder blades down and back, lifting the collarbone completely off the underlying nerves.
Deep Cervical Flexor Endurance: Re-training the tiny muscles in the front of your neck to hold your head perfectly balanced over your spine, ending the reliance on the overworked scalenes.
Stop the Numbness and Save Your Nerves
You do not have to live with a chronically numb, aching arm or consider risky surgical rib resections. By correcting the structural collapse of your upper body and widening the anatomical bottlenecks, physiotherapy can permanently free your nerves.
Book a comprehensive neurological and biomechanical assessment with our specialized team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Why Do My Deep Muscle Knots Keep Coming Back After a Massage?
Because massage only provides temporary symptom relief. Chronic muscle knots, or myofascial trigger points, are active neurological spasms driven by poor posture and joint instability. Physiotherapy cures this by addressing the underlying structural mechanics, permanently shutting down the biomechanical overload causing the spasm.

The Endless Cycle of Temporary Relief
For the thousands of professionals working in Toronto’s Financial District, Liberty Village, and Queen West, extreme muscle tension is a daily reality. The constant stress of deadlines combined with 10-hour days hunched over a laptop invariably leads to burning, rock-hard lumps in the upper back, neck, and shoulder blades.
When these "muscle knots" become so painful that they trigger tension headaches or make it hard to turn your neck, the standard response is to book a deep tissue massage. While an hour on the massage table feels incredible and provides immediate relief, the effect is notoriously short-lived. By Tuesday afternoon, the exact same burning knot has returned in the exact same spot.
Why? Because traditional massage treats the victim (the spasming muscle), but ignores the culprit (the biomechanical failure of the skeleton).
When patients search for "body mechanics physiotherapy" or "remedial mechanics" at Rehab Mechanics, they are looking to break this endless, expensive cycle. We specialize in diagnosing and treating Myofascial Pain Syndrome. We understand that a chronic muscle knot is not just tight tissue; it is a neurological cry for help from an unstable joint. By fixing the structural foundation of your posture, we can turn off the spasm permanently.
Structural Analysis: The Biology of a Trigger Point
To cure chronic muscle knots, we must perform a deep cellular and biomechanical analysis of what a "knot" actually is and why it forms.
The Microscopic Lock (The Sarcomere)
A muscle knot is medically known as a Myofascial Trigger Point. It is not a clump of tangled fibers; it is a chemical and neurological lock-up at the microscopic level.
The Sarcomere: Muscle fibers are made up of millions of tiny contracting units called sarcomeres. When you move, these units slide together and then release.
The Energy Crisis: When a muscle is forced to overwork (like holding your heavy head forward for 8 hours a day), the sarcomeres run out of oxygen and energy (ATP).
The Chemical Lock: Without energy to release the contraction, calcium leaks into the cell, and the sarcomere becomes permanently locked in a shortened, spasming state. A cluster of millions of locked sarcomeres creates the hard, painful nodule you feel under your skin.
The Biomechanical Trigger: Postural Overload
Why do these energy crises happen in the same spots over and over? The answer lies in structural compensation.
The "Tech Neck" Failure
The most common site for chronic trigger points is the upper trapezius and levator scapulae (the muscles where the neck meets the shoulder).
The Heavy Head: Your head weighs about 12 pounds. When your head translates forward to look at a screen, the mechanical leverage changes. Your 12-pound head functionally weighs 40 pounds.
The Desperate Brake: Your upper back muscles are forced to act as an emergency parking brake. They must contract continuously at maximum force to stop your head from falling onto your chest.
The Result: The muscle rapidly exhausts its blood supply, goes into a chemical lock, and forms a massive trigger point. If you massage the knot away but return to the same desk posture, the muscle has no choice but to immediately knot up again to protect your spine.
Primary Source Proof: Structural Myofascial Rehabilitation
Clinical neurological and physical therapy research heavily dictates that treating myofascial pain syndrome requires a multi-modal approach combining deep mechanical release with targeted postural stabilization and joint mobilization to achieve long-term resolution.
Review the Clinical Evidence on PubMed: Effectiveness of Manual Therapy and Corrective Exercise in Myofascial Pain Syndrome (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for myofascial rehabilitation.
The Rehab Mechanics Eradication Protocol
At our Prime Medical Centre clinic, we do not just rub the painful spot. We systematically dismantle the trigger point chemically, and then we rebuild your postural mechanics so the muscle never has to overwork again.
Phase 1: Chemical and Mechanical Deactivation (Weeks 1-3)
We must first force the locked sarcomeres to release and restore blood flow to the starving tissue.
Ischemic Compression: Our physiotherapists apply intense, highly sustained, pinpoint manual pressure directly into the center of the trigger point. This temporarily cuts off all blood flow to the knot (ischemia). When the pressure is released, a massive surge of fresh, oxygen-rich blood rushes in, flushing out the inflammatory pain chemicals and unlocking the sarcomeres.
Instrument-Assisted Soft Tissue Mobilization (IASTM): Utilizing specialized tools to sheer across the fascia, breaking down the dense, fibrotic scar tissue that has built up around the chronic knot.
Phase 2: Joint Unlocking and Skeletal Realignment (Weeks 2-4)
Muscles attach to bones. If the bones are stuck in a bad position, the muscle will stay tight.
Thoracic Spine Mobilization: A hunched, frozen mid-back forces the neck and shoulders to overwork. We utilize high-grade manual joint manipulations to forcefully restore thoracic extension (the ability to arch the mid-back backward).
Cervical Decompression: Gentle manual traction to un-jam the compressed facet joints in the neck, taking the neurological tension off the spasming muscles.
Phase 3: Deep Neuromuscular Fortification (Weeks 4-8)
This is the permanent cure. We must build the biological endurance required to hold your posture perfect for an entire workday.
Deep Cervical Flexor Activation: We use specific biofeedback drills to wake up the tiny muscles in the front of your throat. When these muscles are strong, they automatically pull the head back over the shoulders, instantly turning off the emergency "parking brake" in your upper traps.
Lower Trapezius Endurance: We prescribe targeted Y-raises and prone holds to build massive endurance in the lower shoulder blades, physically anchoring the shoulders down and away from the ears.
Break the Cycle of Tension
You do not have to accept burning shoulders and tension headaches as the inevitable cost of your career. By identifying the root structural failures of your posture and rebuilding your body mechanics, you can permanently eradicate chronic muscle knots.
Book a comprehensive biomechanical and postural assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does Pain Behind the Kneecap Mean My Cartilage is Gone?
No. Sharp, grinding pain beneath the kneecap is usually Patellofemoral Pain Syndrome, caused by poor mechanical tracking, not necessarily cartilage loss. Physiotherapy permanently resolves this by strengthening weak glutes, correcting foot pronation, and realigning the kneecap to eliminate the bone-on-bone friction.
The Agony of the Subway Stairs

Toronto is a highly vertical city. Whether you are walking down into the depths of a TTC subway station, descending the steep steps of your Queen West apartment, or doing lunges at a local gym, your knees are subjected to immense downward pressure.
For many active urbanites, this daily routine is violently interrupted by a sharp, grinding, or dull aching pain located exactly behind or around the edges of the kneecap. The pain is particularly cruel because it is highly specific: it spikes when walking down stairs, but feels fine walking up. It also creates the classic "movie theater sign," where sitting with your knees bent for a long period (like at a desk or on an airplane) causes a deep, throbbing ache that makes you desperately want to straighten your leg.
When patients experience this "crunching" sensation, they instantly panic, assuming their cartilage has completely worn away and they are doomed to early arthritis. At Rehab Mechanics, we frequently diagnose this as Patellofemoral Pain Syndrome (PFPS), commonly known as Runner's Knee.
The good news is that PFPS is rarely a structural degeneration of the knee itself. It is almost always a biomechanical failure of the hip and foot. By correcting the human mechanics above and below the knee, expert physical therapy can perfectly realign the kneecap and permanently silence the grinding pain.
Structural Analysis: The Mechanics of the Kneecap
To cure Runner's Knee, we must stop looking at the knee in isolation and perform a deep analysis of how the kneecap operates within the entire kinetic chain.
The "Train on the Tracks" Anatomy
Your kneecap (patella) does not float freely. It is a biological pulley embedded inside your massive quadriceps tendon.
The Trochlear Groove: On the front of your thigh bone (femur), there is a V-shaped bony groove.
The Tracking Mechanism: When you bend and straighten your leg, the kneecap is supposed to glide perfectly up and down through the dead-center of this groove, like a train on a track.
The Breakdown: Why the Train Derails
Patellofemoral Pain Syndrome occurs when the kneecap is pulled off-center. Instead of gliding smoothly down the middle of the groove, it violently grinds against the outer bony ridge of the femur.
The Pelvic Drop (The True Culprit)
In 80% of PFPS cases, the knee is actually the innocent victim of a weak hip.
Gluteus Medius Weakness: When you stand on one leg (which happens with every step you take while walking or running), the muscle on the side of your hip (gluteus medius) must fire to keep your pelvis level.
Femoral Internal Rotation: If that hip muscle is weak from sitting at a desk all day, your pelvis drops. This causes your entire thigh bone to collapse and rotate inward (valgus collapse).
The Grinding Friction: While the thigh bone rotates inward, the kneecap is held in place by tight outer leg structures (like the IT band). The result is a massive, highly destructive sheer force that grinds the underside of the kneecap against the femur, inflaming the highly sensitive articular cartilage.
The Foot Foundation (Overpronation)
The problem can also start from the ground up.
If you have flat feet or weak arches (excessive pronation), your foot collapses inward when it strikes the pavement.
This inward collapse violently twists the shin bone (tibia) inward, twisting the knee joint and pulling the kneecap aggressively off its tracking line.
Primary Source Proof: Kinematic Rehabilitation
Orthopedic sports medicine literature emphatically supports the "hip-down" approach, proving that strengthening the posterolateral hip musculature provides significantly faster and more permanent relief for patellofemoral pain than traditional knee-focused exercises.
Review the Clinical Evidence on PubMed: Gluteal Muscle Strengthening for Patellofemoral Pain Syndrome (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for knee rehabilitation.
The Rehab Mechanics Kneecap Tracking Protocol
We do not just ice your knee and give you basic leg lifts. To permanently cure PFPS, we must rewire the biomechanics of your entire lower body.
Phase 1: Pain Modulation and Tissue Release (Weeks 1-3)
Before we can build strength, we must release the tight structures that are physically pulling the kneecap off-center.
IT Band and Lateral Retinaculum Release: Our physiotherapists use advanced, deep myofascial release on the outside of the thigh (TFL and vastus lateralis). By loosening these extremely tight structures, we instantly provide mechanical slack, allowing the kneecap to drift back toward the center of the groove.
Patellar Taping (McConnell Taping): We apply rigid kinesiology tape directly over the kneecap, physically taping it into the center of the groove. This mechanically unloads the inflamed tissue and allows you to walk down stairs pain-free while we rehabilitate the muscles.
Phase 2: Hip Isolation and Foundation Fortification (Weeks 4-6)
We must build the muscular scaffolding that prevents the thigh bone from collapsing inward.
Isolated Gluteal Activation: Utilizing targeted, side-lying hip abductions, banded clamshells, and isometric holds to wake up the dormant lateral stabilizers of the pelvis.
VMO Retraining: We use specific biofeedback to teach your brain to fire the vastus medialis oblique (the teardrop-shaped muscle on the inside of the knee) earlier in the movement cycle, actively pulling the kneecap inward against the lateral friction.
Phase 3: Dynamic Integration and Gait Retraining (Weeks 6-10)
Strength on a treatment table means nothing if it doesn't translate to the sidewalk.
Anti-Valgus Training: We progress to dynamic step-downs, lateral lunges, and single-leg squats while utilizing tactile feedback (like a resistance band pulling the knee inward) to force your brain to consciously fire the glutes and push the knee straight.
Foot Mechanics Check: If structural overpronation is driving the knee pain, Sanjay is qualified to assess and dispense custom medical orthotics to permanently support the arch and align the shin bone.
Silence the Grinding Joint
You do not have to live with the fear of stairs or the chronic, aching pain of runner's knee. By identifying and correcting the foundational biomechanics of your hips and feet, physical therapy offers a permanent, non-surgical solution to patellofemoral pain.
Book a comprehensive biomechanical knee assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports recovery in Queen West.
Contact us to schedule your appointment:
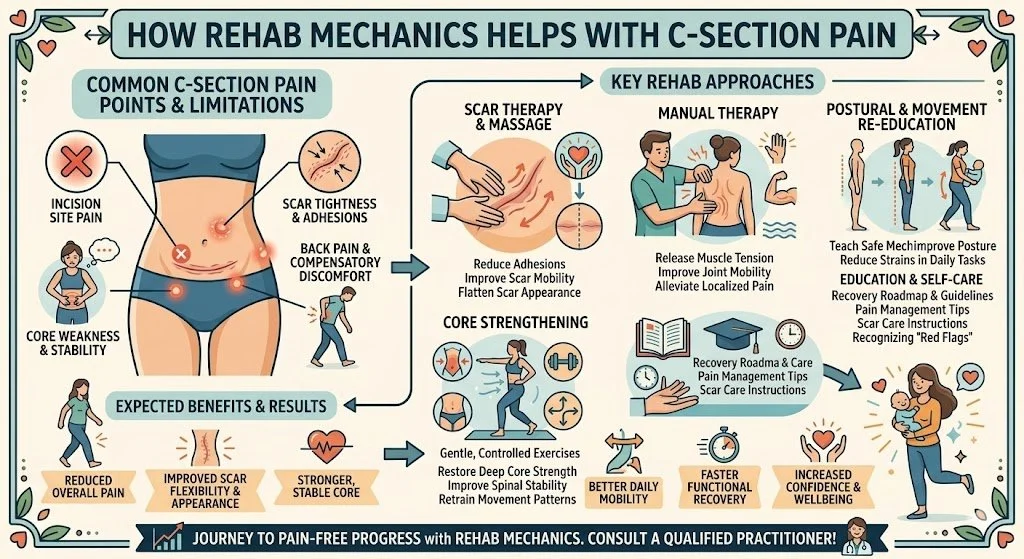
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Can I Heal a Torn ACL and Return to Sports Without Surgery?
Yes. While a completely torn ACL does not biologically reconnect, specialized physiotherapy can make you a "coper." By aggressively strengthening the hamstrings, quadriceps, and neuromuscular reflexes, physical therapy provides immense dynamic stability, allowing many athletes to return to high-level sports without reconstructive knee surgery.
The Devastating "Pop"
For the highly competitive recreational athletes in Toronto—whether you are playing soccer under the lights at Lamport Stadium, running a basketball fast-break in Trinity Bellwoods, or skiing north of the city—a knee injury is the ultimate fear.
The sequence of events is usually identical: you plant your foot, twist your body to change direction, and suddenly feel and hear a violent, sickening "pop" deep inside your knee. The joint instantly swells to the size of a grapefruit, and your leg gives out from under you.
When the MRI confirms a full rupture of the Anterior Cruciate Ligament (ACL), patients are almost universally told that surgical reconstruction is their only option if they ever want to run or play sports again. However, modern orthopedic science has radically challenged this assumption.
When patients search for "prime medical centre physical therapy" or "sports rehabilitation Toronto," they are looking for options. At Rehab Mechanics, we specialize in high-level athletic joint preservation. A torn ACL does not automatically guarantee a trip to the operating room. By meticulously overhauling the human mechanics of your leg, we can train your muscles to do the job of the missing ligament, successfully transforming you into a non-operative "coper."
Structural Analysis: The Mechanics of the ACL
To understand how you can function without an ACL, we must perform a deep biomechanical analysis of knee stability and the crucial difference between passive and active joint control.
The Anatomy of the Knee's Seatbelt
The knee is a massive hinge joint where the femur (thigh bone) sits on top of the tibia (shin bone).
The Passive Restraint: The ACL is a thick, rope-like ligament that runs diagonally through the absolute center of your knee joint.
The Mechanical Job: Its primary anatomical job is to prevent anterior tibial translation—meaning it physically stops your shin bone from sliding dangerously forward out from under your thigh bone when you stop suddenly or land from a jump. It also prevents the knee from rotating too far inward.
The "Coper" Phenomenon (Active vs. Passive Stability)
When the ACL tears, you lose your primary passive restraint. However, the human body is brilliantly engineered with a secondary, active restraint system: your muscles.

Physiotherapy - Rehab Mechanics - ACL tear
The Hamstring Defense System
Your hamstrings (the massive muscles on the back of your thigh) attach to the back of your shin bone.
When the hamstrings contract forcefully, they physically pull the shin bone backward.
This muscular pull does the exact same mechanical job as the ACL.
The Neuromuscular Lag
Neuromuscular: attention to detail - mind-muscle connection
The reason your knee gives out (buckles) after an ACL tear is not just because the ligament is gone; it is because your brain is too slow to fire the hamstrings when you twist.
If we can train your nervous system to fire the hamstrings automatically and explosively the millisecond your foot hits the ground, your knee will be perfectly stable. Patients who successfully achieve this high-level neurological reflex are clinically classified as "copers."
Primary Source Proof: Non-Operative ACL Success
One of the most famous, landmark orthopedic trials in modern sports medicine (the KANON trial) definitively proved that structured, intensive rehabilitation alone yields functional outcomes and meniscus preservation rates equal to early surgical ACL reconstruction.
Review the Clinical Evidence on PubMed: A Randomized Trial of Treatment for Acute Anterior Cruciate Ligament Tears (New England Journal of Medicine)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for sports rehabilitation.
The Rehab Mechanics ACL "Coper" Protocol
Rehabilitating an ACL-deficient knee requires an incredibly aggressive, elite-level conditioning program. We do not just put you on a stationary bike; we rebuild the entire neuromuscular software of your lower body.
Phase 1: Effusion Eradication and Quad Reactivation (Weeks 1-4)
Before we can build strength, we must drain the massive swelling (effusion) that is shutting down your leg.
Arthrogenic Muscle Inhibition (AMI): The massive swelling from the tear triggers a spinal reflex that completely paralyzes your quadriceps muscle. We use Neuromuscular Electrical Stimulation (NMES) and heavy isometric holds to forcefully override this shutdown and wake the quad back up.
Restoring Extension: The knee must be able to lock perfectly straight. If it remains even slightly bent, walking will destroy the cartilage. We use aggressive manual overpressure to restore terminal knee extension.
Phase 2: Heavy Closed-Chain Strength (Weeks 4-10)
Once the swelling clears, we must build a muscular exoskeleton around the knee.
Hamstring Hypertrophy: We implement heavy, eccentric hamstring loading (like Romanian Deadlifts and Nordic Hamstring Curls). The hamstrings must become exceptionally thick and strong to act as your new ACL.
Gluteal Fortification: If the side glute (gluteus medius) is weak, the knee will cave inward during movement, placing terrifying stress on the joint. We heavily load the lateral pelvic stabilizers to keep the leg perfectly straight during single-leg balance.
Phase 3: Perturbation and Neuromuscular Re-Wiring (Weeks 10-16)
Strength is useless if the brain cannot use it instantly.
Reactive Stability: Our physiotherapists apply sudden, unexpected pushes and pulls to your body while you balance on an unstable surface (like a BOSU ball). This "perturbation training" forces your spinal cord to react in milliseconds, firing the hamstrings automatically to secure the joint.
Deceleration Training: We teach your body how to safely absorb the force of gravity. We practice precise landing mechanics from drop jumps, ensuring the hips and glutes take the shock, completely sparing the knee.
Phase 4: Return to Sport (RTS) Testing
We run you through an exhaustive battery of single-leg hop tests, agility drills, and psychological readiness questionnaires. You are only cleared to return to the soccer pitch when your injured leg is performing at 90%+ the capacity of your uninjured leg.
Take the Rehab Path First
Even if you ultimately decide to undergo ACL surgery, completing a rigorous physical therapy program beforehand (Pre-Hab) is clinically proven to drastically improve your surgical outcome. Give your body the chance to prove its resilience.
Book a comprehensive sports knee assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite athletic recovery in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
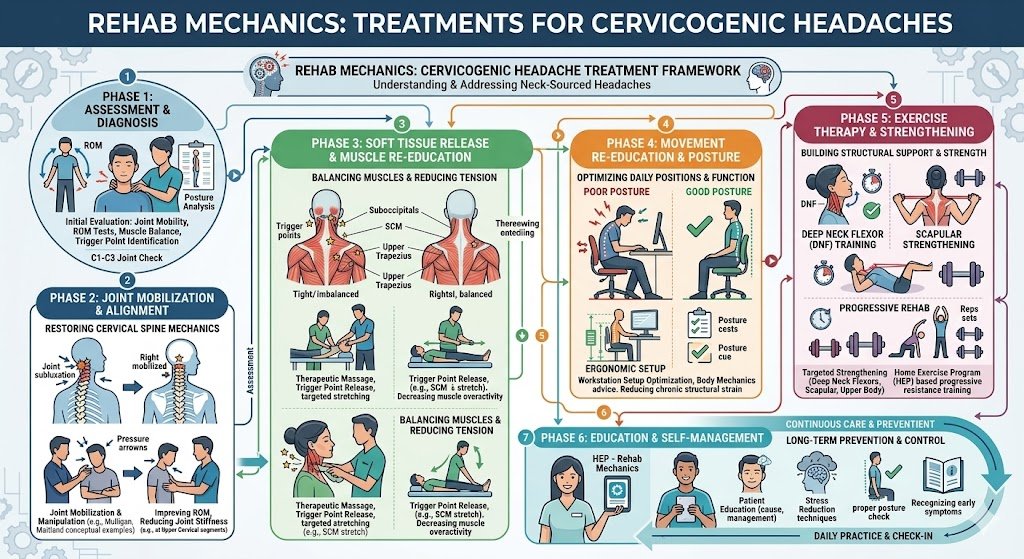
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does a Stiff Neck and Clumsy Hands Mean Cervical Spinal Stenosis?
Yes. A stiff neck combined with dropping objects or hand clumsiness strongly indicates cervical spinal stenosis and potential myelopathy. Specialized physiotherapy physically decompresses the cervical spine, opening the nerve canals to restore neurological function and prevent irreversible spinal cord damage.
The Danger of Ignoring "Just a Stiff Neck"
For the aging tech workers and dedicated professionals in downtown Toronto, a stiff neck is often brushed off as the inevitable cost of a desk-bound career. You rub some muscle cream on your upper back, adjust your monitor, and push through the day.
However, when a chronically stiff neck is suddenly accompanied by bizarre neurological symptoms—such as struggling to button your dress shirt in the morning, constantly dropping your car keys, or feeling a strange, heavy unsteadiness in your legs when walking down Queen Street West—the problem has escalated far beyond a simple muscle strain.
These are the clinical hallmarks of Cervical Spinal Stenosis leading to Cervical Spondylotic Myelopathy. This is not just a pinched nerve in the arm; it is a structural strangulation of the actual spinal cord inside your neck. At Rehab Mechanics, we prioritize elite neurological screening and structural diagnostics. While advanced cases of myelopathy represent a surgical emergency, early and moderate cases of cervical stenosis can be aggressively managed through biomechanical physiotherapy, stabilizing the spine and preventing the condition from deteriorating.
Structural Analysis: The Mechanics of Spinal Cord Compression
To understand the gravity of this condition, we must perform a detailed anatomical analysis of the cervical spine and how space physically runs out over time.
The Anatomy of the Cervical Canal
The seven vertebrae of your neck (C1 through C7) form a protective bony tube called the spinal canal.
The Master Cable: Running directly down the center of this tube is your spinal cord—the master electrical cable that connects your brain to the rest of your body.
The Nerve Roots: Branching off the spinal cord, individual nerve roots exit through small side holes (neural foramina) to power your arms and hands.
The Pathology of Stenosis (Narrowing)
"Stenosis" is the medical term for abnormal narrowing. It is a slow, degenerative cascade driven by age, genetics, and decades of poor posture.
Disc Degeneration and Bulging: As the cervical discs dry out and flatten with age, they bulge backward into the central spinal canal.
Osteophyte Formation: Because the discs are flat, the vertebrae rub together. The body attempts to stabilize the wobbly spine by growing massive, jagged bone spurs (osteophytes) inside the spinal canal and the neural foramina.
Ligamentum Flavum Buckling: The thick ligament that runs down the back of the spinal canal thickens and buckles inward.
Cervical Myelopathy: The Strangulation Effect
When all three of these degenerative changes happen simultaneously, the space inside the spinal canal practically vanishes.
The Crushing Force: The bone spurs, bulging discs, and thick ligaments physically crush the spinal cord itself.
The Neurological Fallout: Because the spinal cord controls the entire body below the neck, the symptoms are widespread. This is Cervical Spondylotic Myelopathy. It cuts off the high-speed neurological signals required for fine motor skills (hands) and heavy balance (legs).
Identifying the Clinical Red Flags of Myelopathy
How do we differentiate a standard pinched nerve from dangerous spinal cord compression? We look for specific, multi-system neurological failures.
Loss of Fine Motor Skills: A sudden inability to perform delicate tasks: handwriting deteriorates, tying shoelaces becomes impossible, or you struggle to use a knife and fork.
The "Heavy Legs" or Balance Issues: You feel uncoordinated, clumsy, or uniquely unsteady when walking, often feeling the need to hold onto walls or a cane.
Bilateral Symptoms: Numbness, tingling, or "electrical shocks" occurring in both hands or arms simultaneously, rather than just one side.
Lhermitte’s Sign: A terrifying sensation of an electric shock shooting rapidly down your spine and into your arms or legs when you aggressively bend your chin down to your chest.
Primary Source Proof: Non-Operative Decompression
Orthopedic and neurosurgical guidelines dictate that while severe myelopathy requires surgery, mild to moderate cervical spinal stenosis can be highly effectively managed with structured physical therapy focusing on deep neck stabilization and postural correction to prevent neurological progression.
Review the Clinical Evidence on PubMed: Non-Operative Management of Cervical Spondylotic Myelopathy and Spinal Stenosis (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for complex spinal rehabilitation.
The Rehab Mechanics Decompression Protocol
Treating cervical stenosis requires absolute caution and immense clinical precision. Aggressively cracking or twisting a stenotic neck is incredibly dangerous. We utilize gentle, targeted "remedial mechanics" to create physical space for the spinal cord.
Phase 1: Mechanical Decompression and Traction (Weeks 1-4)
Our immediate priority is un-pinching the spinal cord and nerve roots without provoking the nervous system.

Manual Cervical Traction: Our specialized physiotherapists apply gentle, sustained upward pulling (distraction) to the skull. This physically separates the cervical vertebrae by millimeters, instantly widening the spinal canal and allowing the suffocating spinal cord to breathe.
Flexion-Biased Mobilization: Looking up at the ceiling (extension) physically closes the spinal canal and crushes the cord. We use highly specific manual techniques to promote slight cervical flexion, which maximizes the diameter of the nerve canals.
Suboccipital Release: Melting away the massive, protective muscle spasms at the base of the skull that are trapping the neck in a rigid, painful block.
Phase 2: Postural Overhaul and Thoracic Unlocking (Weeks 4-8)
We must fix the foundation. The neck cannot find a neutral, open position if the upper back is frozen in a slouch.
Thoracic Spine Mobilization: Utilizing Grade III and IV mobilizations to restore the ability of your mid-back to arch backward. This stops your neck from having to hyper-extend to see the computer screen.
Scapular Retraction: Strengthening the rhomboids and middle trapezius to pull the heavy shoulders back and down, providing a solid platform for the cervical spine to rest upon.
Phase 3: Deep Cervical Fortification (Weeks 8-12+)
Because the structural bones are failing (degeneration), the muscles must take over the job of holding the spine perfectly still.
Deep Cervical Flexor (DCF) Endurance: The tiny muscles in the front of your throat act as the core of your neck. We utilize precise biofeedback drills (like micro-nodding against resistance) to rebuild these vital stabilizers.
Isometric Stabilization: We apply multi-directional, unexpected resistance to your head while you attempt to hold it perfectly still. This trains your nervous system to automatically fire the neck muscles to prevent the wobbly vertebrae from shifting and crushing the spinal cord during sudden movements.
Protect Your Spinal Cord
Do not ignore clumsy hands or unexplainable balance issues. Cervical spinal stenosis is a serious, progressive condition. By radically overhauling your spinal mechanics and building a deep muscular brace, expert physical therapy can halt the progression, relieve the nerve pressure, and help you avoid high-risk spinal surgery.
Book a comprehensive neurological and spinal assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite, diagnostic orthopedic care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
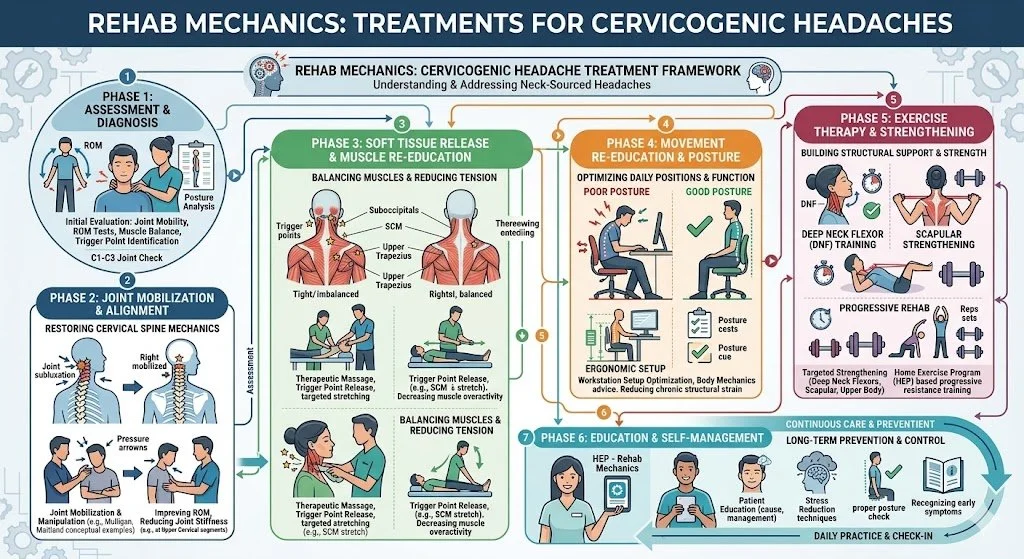
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Is My Inner Knee Pain a Meniscus Tear or Pes Anserine Bursitis?
Maybe. While meniscus tears involve joint clicking, sharp inner knee pain directly below the joint line is often pes anserine bursitis. Physiotherapy resolves this by correcting pelvic mechanics, releasing hyperactive hamstrings, and strengthening the glutes to eliminate the structural friction causing the inflammation.
The Diagnostic Confusion of Medial Knee Pain
For the runners, cyclists, and weekend warriors navigating the paths of Trinity Bellwoods and the Martin Goodman Trail, knee pain is a persistent threat. When a sharp, stinging pain develops on the inside (medial) aspect of the knee, panic often ensues.
Athletes immediately jump to the worst-case scenario: "I've torn my medial meniscus" or "I've blown my MCL." They expect to be scheduled for an MRI and placed on a surgical waitlist. However, at Rehab Mechanics in Queen West, we frequently uncover a highly treatable, yet massively misunderstood, biomechanical culprit: Pes Anserine Bursitis.
While a meniscus tear happens deep inside the joint capsule, pes anserine bursitis happens outside the joint, roughly two inches below the actual knee hinge. It is a severe, friction-based inflammatory condition. When you understand that this condition is not a structural tear of cartilage, but rather a functional failure of your hip and thigh muscles, the path to a full, non-surgical recovery becomes clear. Through advanced human mechanics physical therapy, we can stop the friction and permanently eliminate the inner knee pain.
Structural Analysis: The Mechanics of the "Goose Foot"
To accurately diagnose and treat this condition, we must perform a detailed structural analysis of the medial knee architecture and the specific tendons that anchor there.
The Anatomy of the Pes Anserinus
"Pes Anserinus" is Latin for "goose foot." It refers to the webbed, three-pronged shape of three specific muscle tendons as they merge and attach to the inside of your shin bone (tibia), just below the knee joint.
The Three Muscles: These tendons belong to the Sartorius (front of the thigh), the Gracilis (inner thigh/groin), and the Semitendinosus (inner hamstring).
The Anchor Point: Together, they act as massive, dynamic stabilizers, preventing your lower leg from twisting outward during running and pivoting.
The Bursa Sac: Sitting directly underneath this three-pronged tendon attachment, protecting it from grinding against the hard shin bone, is the pes anserine bursa—a fluid-filled, friction-reducing sac.
The Pathology of Friction (Bursitis)
Bursitis is not a random occurrence; it is a mechanical penalty for poor movement patterns.
The Valgus Collapse Trigger
If your pelvic mechanics are faulty, your knee pays the price.
Gluteus Medius Weakness: When you run, you spend the entire time balancing on one leg. If the muscle on the side of your hip (gluteus medius) is weak from sitting at a desk all day, your pelvis drops.
The Inward Cave: This pelvic drop forces your thigh bone to violently rotate inward, causing your knee to collapse toward your midline (a movement called knee valgus).
The Whiplash Effect: Every time your knee caves inward, the three tendons of the pes anserinus are violently yanked taut against the bone to stop the collapse.
The Inflammatory Crush: This relentless, repetitive yanking physically crushes the bursa sac underneath the tendons. The bursa becomes engorged, swollen, and excruciatingly painful, making it impossible to walk down stairs or run without a sharp, stabbing sensation.
Identifying the Clinical Red Flags
How do we differentiate pes anserine bursitis from a torn meniscus or ligament sprain?
The Location: Meniscus pain is felt directly on the joint line. Pes anserine pain is felt exactly 2 to 3 inches below the joint line, on the flat part of the inner shin bone.
The Touch Test: Pressing your finger directly onto that spot produces a breathtaking, exquisite point-tenderness.
The Stair Trigger: The pain is uniquely severe when descending stairs or stepping down off a Toronto streetcar, as this requires massive eccentric hamstring control, which crushes the inflamed bursa.
Absence of Locking: Unlike a meniscus tear, the knee does not physically "lock," "catch," or click. The hinge works fine; the pain is purely superficial.
Primary Source Proof: Biomechanical Knee Rehabilitation
Orthopedic and sports medicine literature dictates that correcting lumbo-pelvic kinematics and strengthening the hip abductors is the definitive, long-term solution for resolving medial knee overuse injuries like pes anserine bursitis, vastly outperforming localized rest or cortisone injections.
Review the Clinical Evidence on PubMed: The Role of Hip Muscle Function in the Treatment of Patellofemoral and Medial Knee Pain (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for sports rehabilitation.
The Rehab Mechanics Corrective Protocol
We do not just ice the knee. To cure this condition, we must physically alter the angle of your leg during movement.
Phase 1: Tendon Desensitization and Inflammation Control (Weeks 1-3)
We must immediately stop the mechanical crushing of the bursa.
Activity Modification: A temporary halt on running and stair-climbing workouts to allow the swollen bursa sac to chemically cool down.
Advanced Myofascial Release: Our physiotherapists apply targeted, deep manual therapy to the bellies of the hamstring, gracilis, and sartorius muscles high up in the thigh. Releasing the tension at the top of the muscles instantly provides mechanical slack to the tendons at the knee.
Kinesiology Taping: Utilizing strategic taping patterns to gently lift the skin and fascia over the medial knee, decompressing the inflamed bursa and providing immediate pain relief during walking.
Phase 2: Pelvic Fortification and Neuromuscular Control (Weeks 4-6)
We must build the muscular scaffolding that prevents the knee from caving inward.
Isolated Glute Medius Activation: Utilizing side-lying hip abductions, banded clamshells, and isometric wall holds to wake up the lateral stabilizers of the pelvis.
Eccentric Hamstring Loading: Tendons need strength to handle force without spasming. We use slow, controlled hamstring curls and sliders to build robust resilience in the semitendinosus tendon so it no longer crushes the bursa.
Phase 3: Dynamic Integration and Gait Retraining (Weeks 6-8+)
We must ensure your new hip strength translates to the pavement.
Anti-Valgus Training: We progress to dynamic step-downs, lateral lunges, and single-leg squats while utilizing tactile feedback (like a resistance band pulling the knee inward) to force your brain to consciously fire the glutes and push the knee straight.
Cadence Manipulation for Runners: If running is your goal, we may analyze your gait and increase your step cadence by 5-10%. Taking slightly shorter, faster steps drastically reduces the heavy, bounding impact that triggers the valgus collapse.
Stop the Friction, Save Your Knee
You do not have to live with stinging inner knee pain or fear that you have a torn meniscus. By addressing the deep biomechanics of your hip and thigh, physical therapy offers a permanent, non-surgical solution to pes anserine bursitis.
Book a comprehensive biomechanical knee assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Vestibular Physiotherapy Cure Post-Concussion Syndrome and Vertigo?
Yes. Vestibular physiotherapy cures post-concussion syndrome by recalibrating the brain’s sensorimotor integration. Targeted ocular and vestibular exercises eliminate chronic vertigo, visual disturbances, and cognitive fog, restoring normal neurological function after a traumatic brain injury or motor vehicle accident.
The Hidden Neurological Epidemic in Toronto
In the fast-paced, high-density environment of downtown Toronto, traumatic brain injuries are incredibly common. Whether you sustained a violent whiplash injury during a rear-end collision on the Gardiner Expressway, suffered a hard check during a recreational hockey game at a local arena, or simply slipped on an icy sidewalk in Queen West, the resulting concussion can completely derail your life.
For decades, the standard medical advice for a concussion was "cocoon therapy": sit in a dark, quiet room, avoid all screens, and wait for the brain to heal. We now know that prolonged passive rest is actually detrimental.
When patients arrive at Rehab Mechanics weeks or months after their injury, they are often desperate. They describe a lingering, suffocating "brain fog," severe light sensitivity, and a terrifying sensation of vertigo or dizziness every time they turn their head to cross a busy intersection. This is Post-Concussion Syndrome (PCS).

At our clinic inside the Prime Medical Centre, we reject the "wait and see" approach. A concussion is not just a bruise on the brain; it is a profound biomechanical and neurological disconnection. Through highly specialized vestibular physical therapy, we actively rebuild the neural pathways, stopping the dizziness and restoring your cognitive clarity.
Structural Analysis: The Mechanics of a Concussion
To understand how physical therapy can heal the brain, we must perform a detailed structural analysis of what happens during a concussive impact and how the vestibular system operates.
The Neurometabolic Cascade

A concussion is a Mild Traumatic Brain Injury (MTBI). It is caused by a massive acceleration and deceleration force that violently shakes the brain inside the skull.
Axonal Shearing: The delicate nerve fibers (axons) in your brain are stretched and twisted. This sheer force physically damages the cell membranes.
The Energy Crisis: The brain goes into a state of panic, releasing massive amounts of excitatory neurotransmitters (like glutamate). The brain demands a massive amount of glucose (energy) to repair the cells, but the trauma temporarily restricts cerebral blood flow.
The Result: The brain is starved of energy. This metabolic mismatch is what causes the immediate exhaustion, confusion, and deep headaches.
The Vestibular Apparatus Failure
While the brain is recovering chemically, the physical hardware that keeps you balanced is often knocked entirely offline. Your vestibular system is located deep inside your inner ear.
The Semicircular Canals and Otoliths
The Hardware: You have three fluid-filled loops (semicircular canals) in each ear that act as biological gyroscopes, detecting rotational movement. You also have two sac-like structures (otoliths) that detect gravity and linear acceleration.
The Software (Vestibulo-Ocular Reflex): These inner ear sensors constantly talk to your eyes through the Vestibulo-Ocular Reflex (VOR). The VOR is the software program that allows you to keep your eyes perfectly focused on a stationary object while you move your head.
The Pathology of Sensory Mismatch
In Post-Concussion Syndrome, the impact damages the VOR software.
The Glitch: When you turn your head to look for a streetcar, your inner ear tells your brain you are moving at one speed, but your eyes tell your brain you are moving at a different speed.
The Crash: The brain cannot process this conflicting data. It triggers an immediate error response: severe dizziness, sudden nausea, and a feeling of floating or unsteadiness.
Primary Source Proof: Vestibular Rehabilitation
Contemporary neurological and sports medicine literature explicitly mandates that active, targeted vestibular rehabilitation is significantly superior to physical rest for the resolution of prolonged post-concussion symptoms and dizziness.
Review the Clinical Evidence on PubMed: The Effectiveness of Vestibular Rehabilitation in the Treatment of Post-Concussion Syndrome (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for neurological rehabilitation.
The Rehab Mechanics Vestibular Protocol
Treating PCS requires immense clinical precision. We do not just guess; we use specific neurological testing to identify exactly which reflex is broken, and we prescribe targeted "remedial mechanics" to fix it.
Phase 1: Cervicogenic Decompression (Weeks 1-3)
It is biomechanically impossible to sustain a concussion without also sustaining a whiplash injury to the neck.
Upper Cervical Unlocking: The top three joints of the neck (C1-C3) contain thousands of balance sensors. If the neck is locked from whiplash, it sends warped balance signals to the brain, mimicking vertigo. We use precise manual therapy to un-jam these joints.
Suboccipital Release: We apply deep ischemic compression to the tiny, spasming muscles at the base of the skull to instantly relieve the severe tension headaches associated with the trauma.
Phase 2: Neurological Recalibration and Habituation (Weeks 2-6)
We must force the brain to fix the software glitch. We do this through controlled exposure.
Gaze Stabilization (VOR Retraining): We prescribe highly specific ocular drills. You will focus your eyes on a target (like a letter 'X' on the wall) while rotating your head side to side at a specific speed (using a metronome). This forces the brain to repair the connection between the inner ear and the eyes.
Habituation Drills: We intentionally, but safely, expose you to the exact movements that make you dizzy (e.g., bending over to pick up an object and standing up quickly). By repeating these movements in a controlled environment, the brain slowly desensitizes to the motion, turning off the nausea alarm.
Phase 3: Exertional Tolerance and Return to Play (Weeks 6+)
The final step is proving to the brain that it can handle an elevated heart rate without crashing.
Sub-Symptom Threshold Training: We use a stationary bike to carefully elevate your heart rate. We find the exact heart rate that triggers your headache or dizziness (the threshold).
Progressive Overload: We prescribe a daily cardiovascular program where you exercise just below that threshold. Over weeks, this heals the cerebral blood flow problem, safely pushing your threshold higher and higher until you can run, lift, and play sports completely symptom-free.
Clear the Brain Fog
You do not have to live in a dark room or accept chronic dizziness as your new normal. By actively rebuilding your neurological pathways and resolving the structural trauma in your neck, physical therapy can fully restore your balance and mental clarity.
Book a comprehensive post-concussion and vestibular assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced neurological and orthopedic care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Pelvic Floor Physiotherapy Prevent Surgery for Pelvic Organ Prolapse?
Yes. Pelvic floor physiotherapy is the primary, non-surgical treatment for pelvic organ prolapse. By structurally rebuilding the pelvic sling, releasing fascial tension, and mastering intra-abdominal pressure, physical therapy significantly reduces prolapse symptoms and frequently prevents the need for reconstructive surgery.
The Silent Epidemic in Women's Health
In Toronto, the physical demands placed on women are immense. Whether navigating the intense recovery period following childbirth, managing the hormonal shifts of menopause, or maintaining a heavy weightlifting routine at a local Queen West gym, the female pelvic floor is subjected to massive, chronic stress.
A deeply distressing and profoundly under-discussed consequence of this stress is Pelvic Organ Prolapse (POP). Women often discover POP subtly—a feeling of "heaviness" or dragging in the lower pelvis after a long day of standing, a sensation of incomplete bladder emptying, or the terrifying discovery of a physical bulge at the vaginal opening.
The traditional medical reflex is often to wait until the prolapse becomes severe enough to warrant complex reconstructive surgery or the permanent placement of a pessary ring. At Rehab Mechanics, our specialized Perinatal and Pelvic Health program categorically rejects this passive "wait and see" approach. The pelvic floor is a dynamic musculoskeletal system. Through highly specialized, trauma-informed physical therapy, we can radically improve the biomechanical support of your pelvic organs, reversing symptoms and restoring your structural confidence.
Structural Analysis: The Mechanics of the Pelvic Floor
To understand how physiotherapy reverses prolapse symptoms, we must perform a detailed biomechanical analysis of the pelvic architecture and the forces that govern it.
The Anatomy of the Pelvic Sling
The pelvic floor is an intricate, multi-layered hammock of 14 different muscles, thick fascial sheets, and strong ligaments.
The Structural Floor: This hammock forms the absolute base of your abdominal cavity. It physically spans the gap between your pubic bone in the front and your tailbone in the back.
The Organ Support: Resting directly on top of this muscular sling are your vital pelvic organs: the bladder (anterior), the uterus (central), and the rectum (posterior).
The Pathology of Prolapse
Pelvic Organ Prolapse occurs when this supporting hammock fails, allowing one or more of these organs to drop downward into the vaginal canal.
Cystocele: The bladder drops into the front wall.
Uterine Prolapse: The uterus drops straight down the center.
Rectocele: The rectum bulges into the back wall.
The Two Mechanisms of Failure
The hammock can fail for two very different biomechanical reasons.
1. Fascial Tearing (The Trauma Model)
During a prolonged or mechanically difficult vaginal childbirth, the massive downward pressure can physically stretch or tear the thick connective tissue (the endopelvic fascia) and the levator ani muscles. The hammock loses its structural integrity and sags.
2. The Pressure System Failure (The Chronic Model)
Your core is a sealed, pressurized cylinder. The diaphragm is the roof, the abdominals are the walls, and the pelvic floor is the base.
Intra-Abdominal Pressure (IAP): Every time you cough, sneeze, jump, or lift a heavy barbell, the pressure inside this cylinder spikes massively.
The Downward Crush: If your breathing mechanics are faulty—for example, if you hold your breath and bear down heavily when lifting a car seat—you force 100% of that pressure directly down onto the pelvic organs. Over years, this repetitive, crushing downward force stretches the hammock until the organs drop.
Primary Source Proof: Conservative Pelvic Rehabilitation
Global urogynecology and pelvic health research definitively establishes that highly supervised, specific pelvic floor muscle training is the gold standard for reducing symptom severity and improving the anatomical stage of mild to moderate pelvic organ prolapse.
Review the Clinical Evidence on PubMed: Pelvic Floor Muscle Training for Secondary Prevention of Pelvic Organ Prolapse (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for pelvic health.
The Rehab Mechanics Prolapse Protocol
You cannot fix a prolapse by simply downloading a generic app and doing hundreds of "Kegels." Doing Kegels incorrectly can actually worsen the downward pressure. We use a precise, inside-out "human mechanics" approach.
Phase 1: Advanced Diagnostics and Internal Assessment
We must accurately map the muscular failure.
The Internal Exam: With your strict, ongoing consent, our specialized physiotherapist performs an internal vaginal examination. This allows us to physically palpate the muscles to determine their resting tone, strength, endurance, and to identify the exact organs involved in the prolapse.
Hypertonic vs. Hypotonic: Surprisingly, many women with prolapse actually have overactive (hypertonic) pelvic floors. The muscles are constantly clenched in a state of spasm, making them exhausted and useless when a real pressure spike hits.
Phase 2: Restoring the Cylinder (Pressure Management)
Before we strengthen the floor, we must fix the roof.
Diaphragmatic Integration: We completely retrain your breathing mechanics. We teach you how to breathe laterally into your ribcage so the diaphragm and pelvic floor move in perfect synchrony, like a piston, rather than crashing into each other.
The "Knack": Teaching your nervous system to automatically pre-contract the pelvic floor milliseconds before you cough or lift, proactively shielding the organs from the sudden pressure spike.
Phase 3: Neuromuscular Up-Training and Hypertrophy
If the muscles are weak (hypotonic), we must structurally rebuild their thickness and endurance.
Eccentric and Concentric Loading: We guide you through highly specific, graded contractions of the pelvic sling in various gravity-dependent positions (lying down, seated, and eventually standing).
Endurance Holds: The pelvic floor must be able to hold the organs up for a 14-hour day. We build biological endurance using prolonged, sub-maximal isometric holds.
Phase 4: Functional Loading and Real-World Mechanics
We transition your rehab to match your lifestyle demands.
Symptom-Free Lifting: Integrating your new pelvic floor strength into squats, deadlifts, and functional mom-mechanics (like lifting a toddler from a crib).
Pessary Integration: If conservative therapy requires physical support, our physiotherapists can consult and collaborate on the integration of a vaginal pessary—a soft, removable silicone device that acts like an internal sports bra, physically holding the organs up while we rehabilitate the muscles around it.
Take Back Your Structural Confidence
A diagnosis of Pelvic Organ Prolapse does not mean you have to stop exercising, live with chronic heaviness, or immediately schedule surgery. By mastering your intra-abdominal pressure and deeply rehabilitating your pelvic sling, you can manage the condition and reclaim your active life.
Book a highly confidential, specialized pelvic health assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite, private care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is My Hip Bursitis Actually a Torn Glute Tendon?
Yes. Chronic outer hip pain, frequently misdiagnosed as trochanteric bursitis, is usually gluteal tendinopathy. Physiotherapy definitively resolves this by halting compressive stretching, utilizing heavy isometric loading, and restoring pelvic stability to rebuild the degenerated tendon without relying on cortisone injections.
The Diagnostic Confusion of Outer Hip Pain
In the active, aging, and post-partum populations of Queen West and downtown Toronto, lateral (outer) hip pain is a pervasive issue. It usually presents as a deep, aching, or sometimes sharp pain directly over the bony bump on the outside of the hip.
The symptoms are highly specific and incredibly disruptive. Patients find it excruciating to sleep on their side at night. Walking up flights of stairs becomes agonizing, and standing on one leg to put on pants triggers a sharp weakness in the hip.
When patients visit standard medical clinics, they are almost universally handed the exact same diagnosis: "Trochanteric Bursitis." They are prescribed rest, generic hip stretches, and often pushed toward corticosteroid injections to reduce the "inflammation of the bursa sac."
However, at Rehab Mechanics, we know that true, isolated bursitis is exceptionally rare. In the vast majority of cases, the bursa is only inflamed because the massive tendons lying directly on top of it are actively decaying. This condition is Greater Trochanteric Pain Syndrome (GTPS), specifically driven by Gluteal Tendinopathy.
Stretching a degenerated tendon will only cause further structural damage. To permanently cure this hip pain, you must abandon the "bursitis" stretches and aggressively rebuild the tendon’s capacity to handle your body weight.
Structural Analysis: The Mechanics of the Lateral Hip
To successfully rehabilitate gluteal tendinopathy, we must perform a biomechanical analysis of the hip architecture and understand exactly why the tendons are breaking down.
The Anatomy of the Gluteal Cuff
Your hip is stabilized by a network of muscles that function identically to the rotator cuff in your shoulder.
Gluteus Medius and Minimus: These two muscles originate on your pelvis and travel down to anchor directly into the Greater Trochanter (the large, bony bump on the outside of your thigh bone).
The Primary Function: Their absolute primary job is to hold your pelvis perfectly level when you stand, walk, or run on one leg.
The Bursa Sacs: Sitting directly underneath these tendons, right against the bone, are fluid-filled bursa sacs designed to prevent friction.
The Pathology of Compressive Tendinosis
Gluteal Tendinopathy is an overuse injury, but not necessarily from running marathons. It is caused by chronic, daily biomechanical overload and compression.
The "Wrap-Around" Compression

Tendons are designed to be pulled straight. They begin to degenerate when they are tightly wrapped around a bone and crushed.
The Postural Triggers: Sitting with your legs crossed, standing while heavily shifting your weight onto one hip ("hanging on your hip"), or sleeping on your side without a pillow between your knees forces the top leg to drop across the midline of your body (adduction).
The Mechanical Crushing: This posture physically drags the gluteal tendons tightly across the massive bony bump of the greater trochanter. This violent mechanical compression squeezes the blood out of the tendon, triggering cellular death and chaotic scar tissue formation (tendinosis).
The "Bursitis" Illusion: The degenerated, swollen tendon then crushes the underlying bursa sac. While the bursa is inflamed, it is merely the innocent victim of the failing tendon above it.
Identifying the Clinical Red Flags
Treating tendinopathy like simple bursitis guarantees treatment failure. We look for specific mechanical clues to confirm the tendon is the primary pain generator.
The Single-Leg Stance Test: Standing on the affected leg for 30 seconds triggers severe, localized pain over the outside bone, accompanied by a noticeable dropping of the pelvis.
Night Pain: Exquisite pain when sleeping on the affected side (due to direct pressure) OR the unaffected side (because the top leg drops, wrapping the tendon around the bone).
Pain with Stretching: Pulling the knee across the chest (a common "glute stretch") causes the pain to sharply increase, as you are actively compressing the injured tendon against the bone.
Primary Source Proof: Tendon Rehabilitation vs. Cortisone
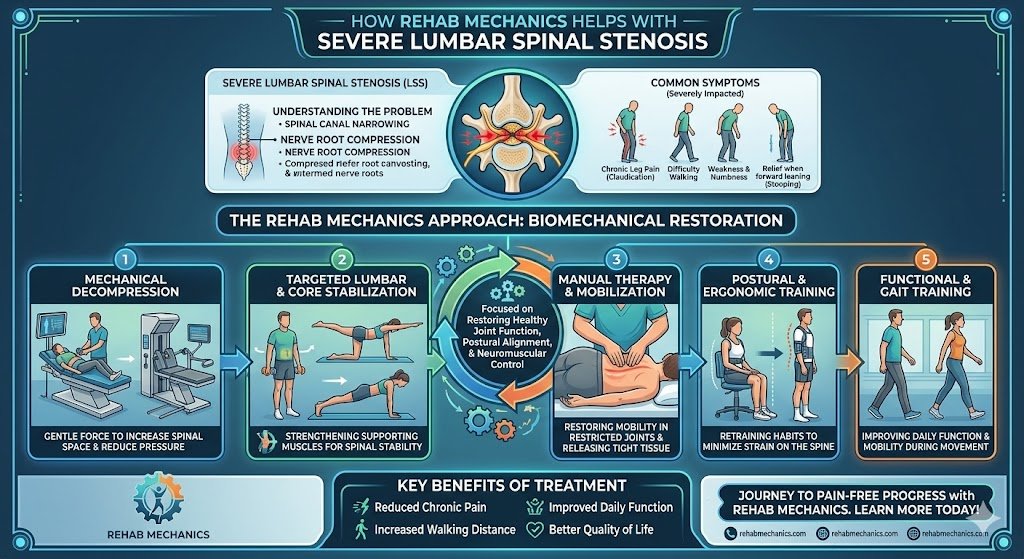
Orthopedic research has revolutionized the treatment of lateral hip pain, definitively proving that targeted, heavy-load physiotherapy protocols vastly outperform corticosteroid injections for long-term resolution and structural healing.
Review the Clinical Evidence on PubMed: Education Plus Exercise Versus Corticosteroid Injection Use in Gluteal Tendinopathy (National Institutes of Health)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for tendon rehabilitation.
The Rehab Mechanics Tendon Protocol
We do not just chase the inflammation. We use advanced "remedial mechanics" to rebuild the tendon's tensile strength and correct the movement faults that caused the compression.
Phase 1: Decompression and Pain Modulation (Weeks 1-4)
The absolute first step is stopping the mechanical crushing of the tendon.
The Anti-Stretch Mandate: We immediately halt all cross-body glute stretching and IT band rolling, as this actively damages the tendon insertion.
Postural Education: We correct your sleep posture (mandating a thick pillow between the knees and ankles) and teach you how to stand with equal weight distribution to eliminate compressive adduction.
Isometric Loading (The Painkiller): We utilize heavy, static holds. You will push your hip outward against an immovable resistance band. This safely fires the glute muscle without moving the joint, which provides a massive, immediate reduction in nerve sensitivity and pain.
Phase 2: Heavy Slow Resistance (HSR) Training (Weeks 4-8)
Once the acute pain subsides, we must force the tendon to lay down new, parallel collagen fibers.
Slow, Heavy Tension: Tendons only remodel under heavy load. We utilize exercises like slow, heavy side-lying hip abductions and weighted clamshells (4 seconds up, 4 seconds down).
Avoiding the Danger Zone: All exercises are strictly controlled to ensure the leg never drops below the midline of the body, allowing us to strengthen the tissue while completely avoiding the painful compressive "wrap-around" zone.
Phase 3: Dynamic Pelvic Control (Weeks 8-12+)
We must teach the newly strengthened tendon how to function during the chaotic mechanics of walking and stair climbing.
Closed Kinetic Chain Integration: Progressing to weight-bearing exercises like offset split squats, step-ups, and single-leg deadlifts.
Trendelenburg Eradication: We meticulously monitor your pelvic mechanics during these movements to ensure your glute fires instantly, keeping your pelvis level and preventing the femur from collapsing inward.
Stop Treating the Wrong Injury
Do not let a misdiagnosis of bursitis trap you in an endless cycle of cortisone shots and painful stretching. By identifying the true tendinopathy and committing to progressive mechanical loading, you can rebuild your hip and sleep through the night pain-free.
Book a comprehensive biomechanical hip assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic rehabilitation in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Should I Stop Running if I Have Severe Shin Splints?
No. Total rest weakens tissues. Physiotherapy cures shin splints by analyzing your running biomechanics, strengthening your lower leg musculature, and utilizing targeted modalities to heal medial tibial stress syndrome while keeping you safely active.
The Frustration of Medial Tibial Stress Syndrome
For the active residents of Parkdale and Trinity Bellwoods, running is more than just exercise; it is a fundamental part of the Toronto lifestyle. However, one of the most common and devastating injuries that sidelines local runners is "shin splints," medically known as Medial Tibial Stress Syndrome (MTSS).
The typical cycle is incredibly frustrating. You feel a dull, aching pain along the inner edge of your shin bone during your run. You ignore it. It worsens into a sharp, burning sensation that persists even while walking. You finally stop running, ice your shins for a month, and wait for the pain to vanish. But the very first day you return to the pavement, the pain instantly returns.
At Rehab Mechanics, we see this exact cycle weekly. The problem with complete rest is that it does absolutely nothing to address why the shin bone became inflamed in the first place. Resolving MTSS requires a biomechanical approach to foot function and load management.
Structural Analysis: What Causes Shin Splints?
To permanently eliminate shin pain, we must perform a structural analysis of the lower leg's kinetic chain. Shin splints are an overuse injury, but they are driven by specific biomechanical failures.
The Anatomy of MTSS

The pain you feel is the result of excessive pulling forces on the periosteum (the thin layer of tissue covering the bone) of the tibia (shinbone).
The Tibialis Posterior: This muscle runs down the back of your calf, crosses under the inside of your ankle, and attaches to the bottom of your foot. Its primary job is to hold up your foot arch.
The Soleus Muscle: A deep calf muscle responsible for absorbing the massive shock of landing with every stride.
Biomechanical Triggers for MTSS
When these muscles are overwhelmed, they pull violently at their attachment points on the shin bone, causing micro-tearing and extreme inflammation.
Excessive Overpronation
If your foot arch collapses too much when you land (overpronation), the tibialis posterior is violently stretched.
The Whiplash Effect: This rapid stretching creates a "whiplash" effect on the muscle tendon, transferring the shear stress directly into the tibial bone.
Weak Hip Stabilizers

If your gluteus medius (side hip muscle) is weak, your knee will collapse inward (knee valgus) when your foot strikes the ground.
The Kinetic Chain Breakdown
This inward knee collapse forces the tibia to rotate internally, massively increasing the torsional strain on the shin bone and lower leg fascia.
Primary Source Proof: Running Kinematics

Our approach to treating running pathologies rejects passive rest in favor of active, evidence-based rehabilitation protocols.
Download Clinical Efficacy PDF: The Role of Biomechanical Loading and Foot Orthoses in the Management of Medial Tibial Stress Syndrome (Open Access Medical Review)
The Rehab Mechanics Treatment Protocol

Treating MTSS effectively requires a progressive, phased approach. We do not just treat the shin; we rebuild the entire leg.
Phase 1: Acute Load Management
We do not prescribe total rest, but we do prescribe relative rest.
Activity Modification: We will temporarily replace pavement running with pain-free cross-training (like cycling or deep-water running) to maintain your cardiovascular fitness.
Manual Soft Tissue Release: Using targeted massage and instrument-assisted techniques to release the hypertonic (overly tight) soleus and tibialis posterior muscles.
Shockwave Therapy: For chronic cases, we utilize shockwave therapy to stimulate blood flow and cellular repair directly at the tibial attachment site.
Phase 2: Structural Strengthening
This is where the cure happens. We must increase the load capacity of your lower leg.
Intrinsic Foot Strengthening: Exercises like "foot doming" or towel scrunches to rebuild the tiny muscles inside the foot that support the arch.
Heavy Slow Resistance (HSR) Calf Training: Progressing from double-leg to single-leg weighted calf raises, specifically focusing on the bent-knee soleus raise, to build bulletproof lower leg tissue.
Gluteal Activation: Clamshells, lateral band walks, and single-leg deadlifts to stabilize the pelvis and prevent the knee from caving inward.
Phase 3: Gait Retraining
Before you return to Trinity Bellwoods, we must fix the way you run.
Cadence Modification: Increasing your step rate by just 5% to 10% drastically reduces the impact forces on the shin bone with each step.
Orthotics Assessment: If structural flat feet are the root cause, Sanjay is qualified to dispense custom medical orthotics to permanently correct the foot mechanics.
Graded Return-to-Run (RTR): Providing a strict, interval-based running schedule to progressively re-introduce mechanical load to the tibia without triggering a relapse.
Run Without Pain in Parkdale and Queen West
Do not let chronic shin splints ruin your running season. Get a definitive biomechanical assessment and an active rehabilitation plan.
Book an appointment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible from Parkdale, Queen West, and Liberty Village.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist and the founder of Rehab Mechanics in Toronto. With over 15 years of clinical practice, Sanjay specializes in complex musculoskeletal rehabilitation, utilizing evidence-based therapeutics to guide his patients toward long-term recovery and optimal athletic performance.
Do I Always Need Physiotherapy for a Rolled Ankle?
Yes. Ignoring a rolled ankle leads to chronic instability and recurring injuries. Physiotherapy restores torn ligaments, rebuilds essential proprioception, and strengthens the surrounding ankle musculature to prevent long-term biomechanical dysfunction and early-onset osteoarthritis.
The Trap of the "Simple" Sprain
"It is just a rolled ankle. I'll walk it off." This is one of the most common and dangerous misconceptions in sports medicine. Whether you rolled it stepping off a curb on Queen Street West, playing a recreational soccer match, or slipping on an icy Toronto sidewalk, an ankle sprain is a severe structural injury.
When patients fail to rehabilitate an ankle sprain, the initial pain and swelling usually subside after a few weeks. However, the underlying mechanical damage remains. Without targeted physiotherapy, the ankle joint heals loosely, leading to a condition known as Chronic Ankle Instability (CAI).
At Rehab Mechanics, we frequently see patients who suffer from recurring ankle sprains, chronic tightness, and early degenerative joint changes simply because they neglected to rehabilitate their very first sprain properly.
Structural Analysis: The Anatomy of a Sprain
To understand why professional rehabilitation is mandatory, we must perform a biomechanical analysis of what exactly happens when an ankle "rolls."

The Lateral Ligament Complex

The vast majority (over 80%) of ankle sprains are "inversion" sprains, meaning the foot rolls inward. This violent motion places catastrophic stress on the lateral ligament complex on the outside of your ankle.
The Anterior Talo-Fibular Ligament (ATFL): This is the weakest and most frequently torn ligament. It stops the foot from sliding forward.
The Calcaneofibular Ligament (CFL): The secondary stabilizer, torn in more severe grade 2 or grade 3 sprains.
The Neurological Damage: Loss of Proprioception

When you tear a ligament, you do not just tear collagen fibers; you tear specialized nerve endings called mechanoreceptors.
What is Proprioception?
Proprioception is your body's subconscious ability to know where its joints are in space. When you walk on uneven ground, mechanoreceptors in your ankle instantly tell your brain to fire the peroneal muscles on the side of your leg to prevent a roll.
The Delay in Signaling
When an ankle is sprained, these nerve endings are destroyed. Even after the ligament heals structurally, the neurological connection is delayed. Your brain cannot react fast enough to a sudden shift in terrain, virtually guaranteeing you will roll the ankle again. Physiotherapy is the only way to rebuild this neurological pathway.
Primary Source Proof: Proprioceptive Rehabilitation

The clinical literature explicitly states that progressive neuromuscular training is non-negotiable for preventing recurrent ankle injuries.
Download Clinical Efficacy PDF: The Effectiveness of Proprioceptive Training in the Prevention of Chronic Ankle Instability (PubMed/NIH)
The Rehab Mechanics Treatment Protocol
Restoring a sprained ankle to 100% capacity requires a phased, progressive loading strategy. Passive treatments like ice and compression are only useful for the first 48 hours. After that, active rehab begins.
Phase 1: Acute Management and Mobility
The goal is to control the swelling while preventing the joint capsule from freezing solid.
Edema Control: Utilizing lymphatic drainage massage and specific taping techniques to flush swelling out of the joint.
Early Range of Motion (ROM): Prescribing pain-free, active movements (like drawing the alphabet with your toes) to align the new collagen fibers correctly as they heal.
Joint Mobilization: Physiotherapists gently glide the talocrural joint to ensure it does not become stiff and restricted.
Phase 2: Muscular Fortification
Once the acute pain subsides, we must replace the lost stability of the torn ligament with muscular strength.

Peroneal Strengthening: Using resistance bands to heavily strengthen the peroneal muscles on the outside of the calf. These muscles are the body's active defense against rolling the ankle inward.
Calf and Tibialis Anterior Loading: Rebuilding the primary shock absorbers of the lower leg to handle the impact of walking and stairs.
Manual Therapy: Deep tissue release on the calf to prevent compensatory tightness from altering your gait.
Phase 3: Neuromuscular Re-education
This is the phase that prevents the next sprain. We rebuild the brain-to-ankle connection.
Balance Training: Progressing from single-leg standing on solid ground, to standing with eyes closed, to standing on unstable surfaces like a BOSU ball or wobble board.
Dynamic Perturbations: The physiotherapist applies unexpected forces while the patient balances, forcing the nervous system to react instantaneously to stabilize the joint.
Plyometrics and Return to Sport: Incorporating jumping, cutting, and lateral bounding drills to prepare the ankle for the chaotic forces of sports and active living.
Secure Your Foundation in Queen West

An unstable ankle changes the way you walk, which eventually damages your knees, hips, and lower back. Treat the injury correctly the first time.
Book a comprehensive ankle assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced biomechanical care in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist and the founder of Rehab Mechanics in Toronto. With over 15 years of clinical practice, Sanjay specializes in complex musculoskeletal rehabilitation, utilizing evidence-based therapeutics to guide his patients toward long-term recovery and optimal athletic performance.
Does Poor Posture Cause Sharp Pain in the Middle of the Back?
Yes. Prolonged desk posture locks the thoracic spine and rib joints, causing sharp, stabbing mid-back pain. Physiotherapy utilizes targeted joint manipulation and postural strengthening to unlock the thoracic vertebrae, restoring full spinal extension and allowing for deep, pain-free breathing.
The Silent Agony of the Desk Worker
When people discuss back pain, they almost exclusively talk about the lower back (lumbar spine) or the neck (cervical spine). However, for the massive population of office workers, software developers, and creatives in downtown Toronto, there is a third, highly agonizing zone: the thoracic spine.
If you experience a sharp, knife-like stabbing sensation directly between your shoulder blades—especially after sitting at your desk for four hours—you are experiencing thoracic joint dysfunction.
This pain is uniquely frightening because it often wraps around the ribcage to the front of the chest, sometimes mimicking the symptoms of a heart condition or making it physically painful to take a deep breath. Countless patients end up in the emergency room out of fear, only to be told their heart is fine and they simply have "muscle strain."
At Rehab Mechanics, we know that generic muscle relaxants will not fix this. This sharp, stabbing pain is a profound mechanical joint lock caused by the modern urban lifestyle. Correcting it requires precise biomechanical physiotherapy to restore the lost mobility of your mid-back and ribcage.
Structural Analysis: The Mechanics of the Thoracic Spine
To understand why sitting ruins your mid-back, we must perform a detailed anatomical analysis of the thoracic spine and its unique relationship with your ribcage.
The Cage of Stability
Your thoracic spine consists of 12 vertebrae (T1 through T12). Unlike your highly mobile neck and lower back, the thoracic spine is designed for rigidity and protection.
The Rib Articulations: Every single thoracic vertebra attaches to a pair of ribs. These ribs wrap around to the front of your chest to protect your heart and lungs, forming the ribcage.
Costovertebral Joints: The tiny joints where the ribs meet the spine at the back are called costovertebral joints. These joints must pivot slightly every single time you inhale to allow your lungs to expand.
The Postural Lock-Down
The human body adapts specifically to the positions it holds most often.
The Kyphotic Curve
If you spend eight hours a day slouching over a laptop in Liberty Village, your thoracic spine is forced into deep, sustained flexion (a rounded "C" shape, known as kyphosis).
The Muscular Exhaustion: The muscles between your shoulder blades (rhomboids and middle trapezius) are stretched taut over this rounded spine. They become exhausted, chemically inflamed, and form massive, burning trigger points.
The Joint Jam (Rib Dysfunction)
The sharp, stabbing pain occurs when the actual joints lock up.
Because the spine is permanently rounded forward, it loses the physical ability to extend (arch backward).
When the thoracic spine locks, the tiny rib joints attached to it also jam.
The next time you try to twist to grab something behind you, or take a deep, forceful breath, that jammed rib joint violently pinches the surrounding capsule and nerves, sending a breathtaking jolt of pain through your chest and back.
Primary Source Proof: Thoracic Mobilization
Orthopedic research confirms that high-grade manual mobilization of the thoracic spine and ribs yields immediate and profound relief for mid-back pain, vastly outperforming generic stretching routines.
Download Clinical Efficacy PDF: The Efficacy of Thoracic Spine Manipulation and Mobilization in the Treatment of Mechanical Mid-Back Pain (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for spinal rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating thoracic pain is highly satisfying clinically because targeted joint mobilization often provides immediate, profound relief. However, we must follow that up with structural strengthening to ensure the pain does not return the next day.
Phase 1: Joint Unlocking and Decompression
We must physically restore the mobility of the spine and ribs.
High-Velocity Low-Amplitude (HVLA) Thrusts: When clinically appropriate, physiotherapists use highly specific, safe manipulations to instantly un-jam the locked facet and costovertebral joints, resulting in an immediate restoration of deep breathing capacity.
Manual Glides: Utilizing Grade III and IV sustained pressure on the vertebrae to gently stretch the stiffened joint capsules and encourage normal spinal extension.
Pectoral Release: Lengthening the tight chest muscles that are physically holding the spine in a rounded, kyphotic position.
Phase 2: Active Mobility Restoration
Once the joints are unlocked, we must train the nervous system to use the new range of motion.
Thoracic Extension Drills: Using foam rollers or specialized massage balls to isolate and actively bend individual spinal segments backward, reversing the desk posture.
Rotational Mobility: Exercises like "open books" or quadruped T-spine rotations to ensure the ribcage can pivot smoothly without catching.
Phase 3: Scapular and Spinal Fortification
To permanently banish the pain, we must build the muscular strength to hold the spine upright against gravity.
Lower Trapezius Activation: Teaching you how to fire the muscles at the bottom of the shoulder blades to pull them down and back.
Isometric Endurance: Implementing heavy farmer's carries and prone positional holds to build the biological endurance needed to sit with perfect posture for an entire 8-hour workday without fatigue.
Reclaim Your Spine
You do not have to endure the burning, stabbing pain of a locked mid-back. Do not settle for another temporary massage. By addressing the specific joint mechanics of your thoracic spine and ribcage, physiotherapy can provide permanent relief and effortless posture.
Book a comprehensive spinal assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.