Can Physiotherapy Cure De Quervain's Tenosynovitis Without Cortisone?
Yes. Physiotherapy effectively cures De Quervain’s tenosynovitis without cortisone. By utilizing targeted thumb splinting, deep soft tissue release, and progressive eccentric loading, physiotherapy reduces tendon sheath inflammation and restores pain-free grip strength for new parents and tech workers.
The Urban Epidemic of "Mommy Thumb" and Tech Wrist
Liberty Village and Queen West are vibrant neighborhoods characterized by two distinct demographics: young, growing families and highly driven tech professionals. While these groups seem completely different, they frequently walk into Rehab Mechanics suffering from the exact same debilitating injury: De Quervain's Tenosynovitis.
Whether you are repeatedly lifting a growing newborn out of a crib 30 times a day, or spending 10 hours furiously typing and swiping on a smartphone, your thumbs and wrists are undergoing massive, unnatural mechanical stress.
When a sharp, catching, or burning pain develops at the base of the thumb and radiates up the forearm, basic tasks like turning a doorknob, holding a coffee mug, or unbuckling a car seat become agonizing. The traditional medical approach often involves a quick corticosteroid injection. However, chemical injections do not fix the biomechanical overload. To permanently resolve this severe wrist pain, you must physically rehabilitate the tendons and the restrictive sheaths that surround them.
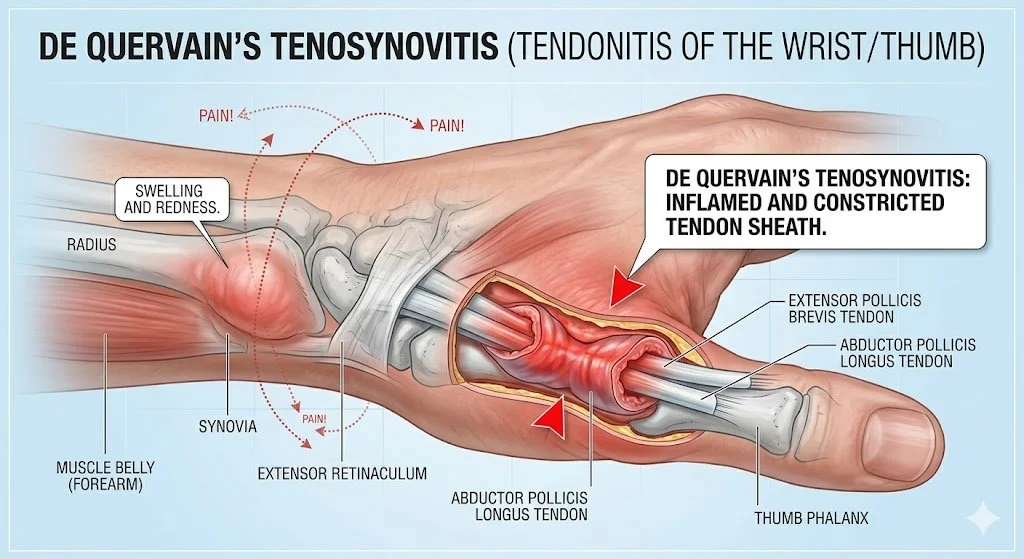
Structural Analysis: The Anatomy of the First Dorsal Compartment
To understand why this specific injury is so stubborn and painful, we must perform a detailed biomechanical analysis of the wrist's architecture.
The Extensor Retinaculum
Your wrist is wrapped in a thick, fibrous band of connective tissue called the extensor retinaculum. Its job is to act like a biological pulley system, keeping your tendons strapped tightly to the bones of your wrist so they do not bow outward when you move your hand.
The Tunnels (Compartments): This band is divided into six distinct tunnels or "compartments."
The Vulnerable First Compartment: De Quervain's syndrome occurs exclusively in the very first compartment, located directly over the styloid process of the radius (the bony bump at the base of your thumb).
The Tendons Involved
Two specific tendons must share this incredibly tight, rigid tunnel:
Abductor Pollicis Longus (APL): The muscle that pulls your thumb away from your hand.
Extensor Pollicis Brevis (EPB): The muscle that straightens the tip of your thumb.
The Biomechanical Friction
Every time you grip an object and angle your wrist downward (a motion called ulnar deviation—exactly the motion used to lift a baby under the armpits), these two tendons slide rapidly back and forth through the first compartment.
Tenosynovitis Explained
When the mechanical load exceeds the tissue's capacity, a destructive cycle begins.
Synovial Swelling: The protective, lubricating sheath (synovium) surrounding the tendons becomes intensely inflamed and swollen from the friction.
The Strangulation Effect: Because the bony tunnel and the retinaculum cannot expand, the swollen tendons become trapped. They physically catch and grind against the walls of the tunnel, causing exquisite, sharp pain and sometimes a visible, hard swelling at the base of the thumb.
Identifying the Clinical Red Flags
De Quervain's is frequently misdiagnosed as carpal tunnel syndrome or thumb arthritis. We look for specific mechanical signs:
Finkelstein's Test: If you tuck your thumb inside your fist and aggressively tilt your wrist downward toward your pinky, a breathtaking, sharp pain along the thumb side of the wrist is a positive indicator.
The "Catch" or "Snap": A physical sensation of the tendon popping or snapping as it struggles to drag itself through the swollen compartment.
Localized Swelling: A tender, highly sensitive, swollen bump directly on the radial bone.
Primary Source Proof: Non-Operative Wrist Rehabilitation
Clinical orthopedic research explicitly supports the use of progressive, conservative physiotherapy—including targeted splinting and eccentric loading—as a highly effective, first-line intervention for stenosing tenosynovitis.
Download Clinical Efficacy PDF: The Effectiveness of Conservative Management and Eccentric Exercise in De Quervain’s Tenosynovitis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for upper extremity rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating De Quervain's requires absolute clinical precision. You cannot aggressively stretch an already strangled tendon. We utilize a highly specific, three-phased biomechanical approach.
Phase 1: Acute Offloading and Inflammation Control (Weeks 1-3)
We must physically stop the friction to allow the synovial swelling to subside.
Thumb Spica Splinting: We provide a specialized, rigid splint that immobilizes the thumb and wrist. Wearing this temporarily prevents the APL and EPB tendons from sliding through the inflamed compartment, halting the mechanical irritation.
Advanced Modalities: Utilizing extracorporeal shockwave therapy (ESWT) or targeted interferential currents to rapidly decrease the acute chemical inflammation without relying on oral medications.
Phase 2: Soft Tissue Decompression
The muscles attached to the inflamed tendons are usually in massive spasm.
Instrument-Assisted Soft Tissue Mobilization (IASTM): Our physiotherapists use specialized tools to break down the tight, fibrotic tissue in the forearm muscle bellies, instantly reducing the pulling tension on the tendons passing through the wrist.
Joint Mobilization: Gently mobilizing the carpal bones (specifically the scaphoid and trapezium) to ensure optimal joint mechanics and remove any secondary bony compression.
Phase 3: Eccentric Loading and Neuromuscular Control
Once the pain decreases, we must structurally rebuild the tendon to handle your daily life.
Eccentric Strengthening: Tendons respond incredibly well to the "lowering" phase of an exercise. We prescribe specific, heavy, slow eccentric thumb extensions and radial deviations to force the body to lay down new, healthy, parallel collagen fibers, thickening and bulletproofing the tendon.
Ergonomic Coaching: For parents, we teach the "scoop" lifting technique to avoid dangerous ulnar deviation. For tech workers, we implement ergonomic mouse alternatives and split keyboards to keep the wrist entirely neutral during a 10-hour workday.
Stop the Wrist Pain Today
You do not have to struggle to hold your child or type your emails. De Quervain's tenosynovitis is a structural problem with a highly effective mechanical solution.
Book a comprehensive upper extremity assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite orthopedic care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.