How Does Blood Flow Restriction (BFR) Training Accelerate Injury Recovery? Physiotherapy in Toronto | Rehab Mechanics
How Does Blood Flow Restriction (BFR) Training Accelerate Injury Recovery?
Summary for those on GO (TL;DR):
Blood Flow Restriction (“BFR”) training accelerates injury recovery by utilizing a specialized medical pneumatic tourniquet to partially restrict venous blood flow out of a muscle while maintaining arterial inflow. This creates a highly localized hypoxic (low-oxygen) environment that "tricks" the brain into triggering massive muscle growth and cellular repair using only very light weights (typically 20% - 30% of a patient's One Repetition Maximum). This evidence-based modality is exceptionally effective for the following types of patients:
post-operative patients;
severe tendinopathies, and
joint injuries where heavy lifting is clinically contraindicated.
Key Takeaways:
Primary Clinical Benefit: BFR allows patients to achieve the profound muscle hypertrophy (growth) and strength gains normally associated with heavy weightlifting, but with a fraction of the mechanical stress placed on vulnerable, healing joints or surgical repairs.
Target Demographics: Highly indicated for post-surgical ACL reconstructions, severe osteoarthritis patients, meniscus repairs, and chronic tendinopathies where traditional high-load resistance training provokes severe pain.
Core Modalities: Rehabilitation involves the application of a clinical-grade pneumatic cuff to the upper arm or thigh, followed by a strict protocol of high-repetition, low-load exercises under constant physiological monitoring by a registered physiotherapist.
General Timelines: Measurable increases in muscle cross-sectional area and functional strength are frequently observed within 3 to 6 weeks of consistent BFR integration, significantly preventing the rapid muscle atrophy that typically follows a severe injury.

A physiotherapist at Rehab Mechanics monitoring a patient performing a low-load squat while wearing an FDA-approved pneumatic Blood Flow Restriction (BFR) cuff on the proximal thigh, illustrating a modern clinical modality for accelerated muscle hypertrophy.
Understanding the Physiology and Biomechanics of BFR Training
Historically, the golden rule of muscle physiology and rehabilitation dictated that to build significant muscle mass and restore functional strength, a patient must lift heavy mechanical loads. According to the principles of mechanotransduction, tissues adapt to the specific demands placed upon them. In practice, this meant lifting weights exceeding $70\%$ to $80\%$ of a patient's One Repetition Maximum ($1\text{RM}$) to stimulate structural changes in the muscle fibers.
However, when a patient suffers a severe acute injury (such as a torn ACL, a ruptured Achilles, or a rotator cuff repair) or is dealing with highly reactive joint degeneration (such as severe knee osteoarthritis), placing heavy mechanical loads on the joint is dangerous, structurally compromising, or simply physically impossible due to pain.
The Threat of Arthrogenic Muscle Inhibition (AMI)
This inability to lift heavy weights creates a vicious and rapid clinical cycle. When a joint is injured or undergoes surgery, the body initiates a neurological protective mechanism known as Arthrogenic Muscle Inhibition (AMI). The central nervous system literally "turns off" the muscles surrounding the injured joint to prevent further movement and protect the damaged tissue.
For example, following knee surgery, the quadriceps muscle can begin to visibly atrophy (waste away) and lose significant strength within a matter of days due to AMI. Because the joint hurts, the patient cannot lift heavy weights to reverse the atrophy; because the muscles remain weak, the joint becomes even less stable and more painful.
Blood Flow Restriction (BFR) training offers a profound solution: it chemically bypasses the mechanical requirement for heavy lifting, allowing us to halt muscle atrophy and rebuild the joint's "engine" without straining the damaged "chassis."
The Science of the Ischemic Environment and Metabolic Stress
During a clinical BFR session, a specialized medical-grade pneumatic cuff is placed on the proximal portion of the limb (the uppermost part of the arm near the shoulder, or the upper thigh near the groin).
Calculating Limb Occlusion Pressure (LOP)
Crucially, the goal is not to completely cut off circulation, which would be extremely dangerous. Instead, the BFR device is inflated to a highly precise, individualized pressure known as the Limb Occlusion Pressure (LOP). A physiotherapist utilizes a Doppler ultrasound or the BFR device's internal Bluetooth sensors to determine the exact pressure required to cut off $100\%$ of the blood flow for that specific patient on that specific day.
Once the maximum LOP is found, the cuff pressure is dialed back to a therapeutic range—typically $50\% - 80\%$ LOP for the legs, and $40\% - 50\%$ LOP for the arms. This precise calibration allows oxygenated arterial blood to flow into the working muscle, but strictly restricts the deoxygenated venous blood from flowing out.
Hypoxia and Cellular Swelling
As the patient performs a simple, low-load exercise (e.g., lifting $20\%$ of their max capacity), the working muscle rapidly burns through its local oxygen supply. Because new oxygen is arriving slowly and the waste products cannot escape, the localized tissue environment becomes severely hypoxic (low-oxygen) and highly acidic.
This pooling of blood and the rapid accumulation of metabolic byproducts (such as lactic acid and hydrogen ions) creates profound metabolic stress. Additionally, the pooling blood causes extreme cellular swelling, which physically stretches the walls of the muscle cells. The body's central nervous system perceives this intense metabolic stress and cellular swelling as a massive physiological emergency—as if the patient is lifting a monolithic weight—and it reacts by initiating a massive repair cascade.
Henneman’s Size Principle and Systemic Hormonal Release
To understand why BFR builds muscle so effectively with light weights, we must look at how the brain communicates with muscles. Henneman’s Size Principle dictates that the nervous system recruits muscle fibers in a specific sequence, starting with the smallest, most fatigue-resistant fibers first, and only calling upon the largest, most powerful fibers when absolutely necessary.
Under normal circumstances, your body relies on Type I (slow-twitch, endurance) muscle fibers for light tasks like walking or lifting light objects. Because these fibers rely heavily on oxygen, they can work for a long time without fatiguing. To force the body to recruit the massive Type II (fast-twitch) muscle fibers—the ones responsible for explosive strength and significant muscle growth—you typically have to lift a very heavy weight that overwhelms the Type I fibers.
The Hypoxic Hack
BFR completely short-circuits this neurological rule. Because the BFR cuff has created a low-oxygen environment, the oxygen-dependent Type I fibers exhaust and fail almost immediately. Panic-stricken, the central nervous system is forced to prematurely recruit the massive Type II fast-twitch fibers just to continue moving the very light weight.
Simultaneously, the intense buildup of lactic acid and the firing of these Type II fibers triggers the anterior pituitary gland in the brain to release a massive systemic surge of Human Growth Hormone (HGH) and Insulin-like Growth Factor-1 (IGF-1). These powerful anabolic hormones are flushed through the entire bloodstream, accelerating collagen synthesis, bone healing, and massive muscle hypertrophy. Through BFR, we achieve the systemic biological healing response of Olympic weightlifting while mechanically protecting the injured local tissue.
Clinical Assessment: Medical vs. Recreational BFR
It is vital to distinguish clinical BFR therapy from recreational "gym-bro" occlusion training. Wrapping a knee wrap or an elastic band tightly around a limb at the gym is highly dangerous, as it offers no way to measure arterial inflow, risking severe nerve damage or complete arterial occlusion.
At our 68 Abell Street facility in Toronto, we utilize only FDA and Health Canada-approved medical pneumatic tourniquets that continuously monitor and adjust pressure. Furthermore, an exhaustive in-person physical assessment and medical history review are legally and clinically required before initiating BFR therapy.
Because BFR temporarily alters localized blood pressure and cardiovascular demand, a physiotherapist must rule out absolute contraindications, which include:
Deep Vein Thrombosis (DVT): A history of blood clots, endothelial dysfunction, or severe vascular compromise.
Severe Hypertension: Unmanaged or highly volatile high blood pressure.
Pregnancy: BFR is strictly contraindicated during pregnancy due to altered hemodynamics.
Active Cancer or Tumor: Within the affected limb or lymphatic system.
Severe Peripheral Neuropathy: Loss of sensation that would prevent the patient from providing accurate feedback on cuff comfort and nerve compression.
Only after a precise diagnosis is established, absolute contraindications are ruled out, and informed patient consent is obtained detailing the risks and physiological sensations of the treatment, will BFR interventions commence.
Comprehensive Treatment Modalities Utilizing BFR
Rehabilitation using BFR at Rehab Mechanics is never a standalone treatment; it is a highly specialized tool integrated into a broader, multimodal recovery framework.
The Standard Clinical Protocol (30-15-15-15)
The clinical application of BFR relies on high-repetition, short-rest protocols to intentionally maximize the accumulation of metabolites. Once the cuff is inflated to the precise therapeutic pressure, the patient begins a highly specific, grueling set structure using only $20\% - 30\%$ of their $1\text{RM}$:
Set 1: 30 repetitions (This initial high-rep set acts as the "primer" to rapidly deplete local oxygen and initiate the lactic acid burn).
Rest: 30 seconds (Crucially, the cuff remains inflated during the rest period to trap the metabolites and prevent oxygen from flushing the muscle).
Set 2: 15 repetitions.
Rest: 30 seconds.
Set 3: 15 repetitions.
Rest: 30 seconds.
Set 4: 15 repetitions (Totaling 75 repetitions).
The cuff is immediately deflated after the final repetition, allowing a massive rush of highly oxygenated, nutrient-dense blood to flood the tissue (hyperemia).
Condition-Specific Applications
This protocol is utilized with basic, joint-sparing exercises tailored to the specific injury:
Post-Operative ACL: Simple straight-leg raises or isometric quad sets to reverse Arthrogenic Muscle Inhibition without straining the new graft.
Knee Osteoarthritis: BFR applied during stationary cycling (10-15 minutes of low-intensity biking) to build quad strength while offloading the bone-on-bone joint.
Achilles Tendinopathy: Seated calf raises with BFR to safely load the calf complex and tendon without requiring heavy, painful standing weights.
Integration with Manual Therapy
BFR optimally pairs with targeted soft tissue therapy and joint mobilizations. While BFR aggressively rebuilds the muscular "engine," manual therapy is utilized to ensure the "chassis" (the joint capsule and fascial tissue) moves freely. Restoring normal joint arthrokinematics through manual mobilization ensures that the newly acquired muscle strength is applied efficiently, safely, and smoothly through a full, pain-free range of motion.
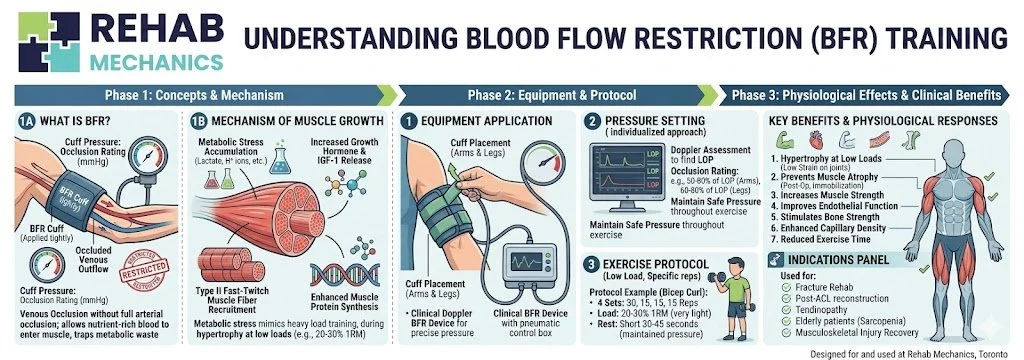
Our homemade curated diagram for BFR
Phase Breakdown for BFR Rehabilitation
Rehabilitation PhaseBFR Application & LoadingClinical Objective
Phase 1: Post-Acute Atrophy Prevention
Isometric holds and gravity-eliminated movements with BFR. Cuff pressure is moderate.
Prevent severe post-surgical or post-injury muscle wasting (AMI) without loading the damaged joint.
Phase 2: Hypertrophy & Cellular Repair
Isotonic movements (e.g., leg extensions, bicep curls) at $20\%-30\%$ $1\text{RM}$. Standard 75-rep protocol.
Induce profound metabolic stress, stimulate early Type II fiber recruitment, and trigger systemic growth hormone release.
Phase 3: Mechanical Loading Transition
Deflating the cuff; transitioning to heavier, traditional resistance training ($60\%+$ $1\text{RM}$).
Begin conditioning the tendons, ligaments, and bones to tolerate heavy, real-world mechanical stress.
Phase 4: Functional Return
Plyometrics, heavy compound lifts, and multi-joint occupational simulations without BFR.
Restore full, unrestricted athletic or occupational capacity and dynamic stability.
Author Biography
Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist.
Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:
The content provided in this article is for general educational and informational purposes only and does not constitute formal medical advice. Individual physiological responses to physiotherapy and vascular therapies vary significantly. Rehab Mechanics does not guarantee specific treatment outcomes. An in-person assessment is legally and clinically required to definitively evaluate cardiovascular suitability, rule out vascular contraindications, develop a treatment plan, and obtain informed consent before commencing BFR therapy.