How to Treat Cervicogenic Headaches? Physiotherapy for Neck Pain | Rehab Mechanics
How to Treat Cervicogenic Headaches?
Summary for our “Multi Taskers” (TL;DR):
Physiotherapy treats cervicogenic headaches by addressing the mechanical dysfunctions in the upper cervical spine (the neck) that are referring pain into the head. By utilizing targeted joint mobilizations to restore mobility in the C1-C3 vertebrae, releasing hypertonic suboccipital muscles, and prescribing corrective exercises to strengthen the deep neck flexors, physiotherapists can dismantle the root cause of the pain rather than temporarily masking the symptoms.
Key Takeaways:
Primary Symptoms: A dull, unilateral (one-sided) ache that begins at the base of the skull and radiates forward over the top of the head, frequently settling behind one eye, in the temple, or along the jawline. Pain is typically aggravated by sustained neck postures (like staring at a monitor) or specific head movements.
The Pathology: Cervicogenic headaches are not vascular (like migraines) or neurochemical; they are strictly mechanical. Irritation of the facet joints, ligaments, or nerves in the top three vertebrae of the neck physically refers pain signals into the facial region via a neurological relay station called the trigemino-cervical nucleus.
Core Modalities: Evidence-based management requires upper cervical manual therapy, suboccipital myofascial release, and a strict postural re-education protocol to reverse "forward head posture."
General Timelines: With strict adherence to clinical advice, manual therapy, and workplace ergonomic modifications, significant reductions in headache frequency and intensity are commonly observed within 3 to 6 weeks of targeted physiotherapy intervention.
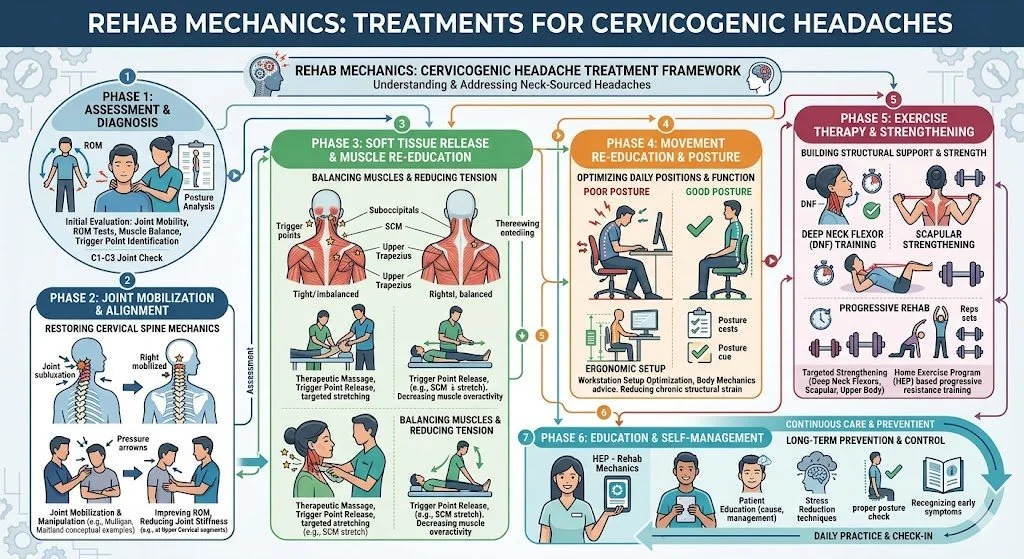
Medical diagram demonstrating the upper cervical spine (C1-C3 vertebrae) and the suboccipital muscles, illustrating the neurological pathway where neck irritation refers pain through the greater occipital nerve over the skull, identifying the source of cervicogenic headaches
Understanding the Anatomy of a Cervicogenic Headache
A headache is not always a problem inside the head. In fact, for a massive segment of the population—particularly modern office workers, software developers, and individuals engaged in prolonged screen time—chronic headaches are actually a symptom of severe mechanical dysfunction originating in the neck.
Medically, a cervicogenic headache translates literally to "a headache originating from the cervical spine." To understand why a stiff joint in your neck causes a piercing, relentless pain behind your right eye, we must examine the highly complex biomechanical structure of the upper neck and the intricate neurological wiring of the upper spinal cord.
The Atlas and the Axis: The Biomechanics of the Upper Neck
The root cause of a cervicogenic headache almost exclusively lies in the top three vertebrae of the neck, known as C1, C2, and C3. The top two bones are anatomically unique compared to the rest of the spine.
C1 (The Atlas): Named after the mythological Titan who held up the world, the Atlas holds up your skull. It does not have a traditional solid "body"; it is essentially a bony ring that cradles the base of the head, allowing for the "nodding" (flexion/extension) motion.
C2 (The Axis): The Axis features a bony peg (the dens) that sticks straight up through the ring of the Atlas.
The joint between these two bones—the atlanto-axial joint—is responsible for approximately 50% of the total rotational capacity of your entire neck. Because it is highly mobile, it is inherently less stable and highly susceptible to mechanical locking, joint stiffness, and ligamentous strain. When this specific joint stops gliding smoothly, a cascade of localized inflammation and muscle guarding begins.
The Trigemino-Cervical Nucleus: The Neurological Short-Circuit
The physical stiffness in the C1-C3 joints is translated into a headache through a fascinating neurological anomaly. The sensory nerves that exit these upper vertebrae converge in a specific, dense cluster of the spinal cord known as the Trigemino-Cervical Nucleus.
Crucially, the Trigeminal Nerve—the major, three-branched cranial nerve responsible for feeling sensation in your eye (V1 branch), upper cheek (V2 branch), and jaw (V3 branch)—also plugs into this exact same neurological hub.
When the facet joints of the upper neck become jammed, inflamed, or mechanically irritated, they send continuous distress signals into this shared hub. Because the brain struggles to differentiate exactly where the signal originated within this crowded neurological intersection, it frequently misinterprets the neck pain as coming from the face, the temple, or the front of the head. This phenomenon is known as referred pain. It is the exact same neurological mechanism that causes a patient experiencing a heart attack to feel pain in their left arm.
The Mechanical Triggers: "Tech Neck" and The Suboccipitals
The most common culprit triggering this neurological cascade is "Upper Cross Syndrome," better known as forward-head posture or "tech neck." When you hunch over a laptop or smartphone, your skull shifts forward.
The human head weighs approximately 10 to 12 pounds. However, basic physics dictates that for every inch your head shifts forward out of a neutral alignment, the functional weight placed on the cervical spine doubles. A head shifted forward by 30 degrees effectively weighs 40 pounds.
To keep your eyes level with the horizon while your head is jutting forward, your body must sharply hinge the skull backward at the very top of the neck (the C1-C2 level). This unnatural hinging crushes the delicate facet joints and places extreme, chronic tension on the suboccipital muscles—a group of four tiny, highly sensitive muscles located precisely at the base of the skull.
When these muscles go into chronic spasm from overwork, they frequently entrap and compress the Greater Occipital Nerve as it pierces through the muscle belly. This compression triggers a sharp, shooting, or burning pain that arcs over the top of the skull like a ram's horn.
Clinical Assessment: Migraine vs. Cervicogenic Headache
Differentiating a cervicogenic headache from a vascular migraine or a tension-type headache is the most critical step in rehabilitation, as the clinical treatments are vastly different. Treating a mechanical neck joint issue with migraine medication will only yield frustration. At our Queen West clinic, a thorough orthopedic and neurological assessment is a strict clinical requirement.
A physiotherapist will look for specific diagnostic markers that indicate a cervical origin:
Unilateral Presentation: The headache is almost always strictly on one side of the head and does not "side-shift" during an attack.
Mechanical Provocation: The headache can be actively triggered, worsened, or relieved by the physiotherapist manually applying pressure to the upper neck joints or by asking the patient to hold specific, awkward neck postures.
Absence of True Migraine Auras: While nausea can occasionally occur if the pain is severe, true cervicogenic headaches generally lack the visual auras (flashing lights), intense photophobia (light sensitivity), or neurological deficits common to severe vascular migraines.
The Cervical Flexion-Rotation Test (CFRT)
To definitively isolate the upper neck, physiotherapists utilize the gold-standard diagnostic assessment known as the Cervical Flexion-Rotation Test.
During this test, the patient lies flat on their back. The physiotherapist gently flexes the patient's neck entirely forward; this action structurally "locks out" the lower cervical vertebrae (C3-C7), ensuring they cannot move. With the neck fully flexed, the physiotherapist then rotates the head left and right.
Because the lower neck is locked out, the rotation is almost entirely isolated to the C1-C2 (atlanto-axial) joint. A normal, healthy joint should rotate approximately 45 degrees in either direction. If the rotation is severely restricted (less than 32 degrees) or if the movement instantly reproduces the patient's familiar headache, a cervicogenic pathology is clinically confirmed.
(Clinical Note: During this assessment, the physiotherapist will also perform vital neurological screening to rule out 'red flags'—such as Vertebrobasilar Insufficiency (VBI) or cervical artery dysfunction—ensuring that manual therapy is 100% safe to proceed.)
Comprehensive Treatment Modalities at Rehab Mechanics
Because cervicogenic headaches are fundamentally a mechanical joint and muscle issue, they respond exceptionally well to mechanical interventions. Pharmaceutical painkillers may temporarily mask the referred pain, but they cannot fix a jammed spinal joint or a weak muscle.
Manual Joint Mobilization
The primary, most immediate intervention is restoring the normal glide and mobility of the C1, C2, and C3 vertebral segments. Physiotherapists utilize highly specific, low-grade manual joint mobilizations.
Techniques such as Sustained Natural Apophyseal Glides (SNAGs), based on the Mulligan concept, involve the therapist applying a gentle, sustained pressure to the specific stiff vertebra while the patient actively rotates their head. By physically unjamming these stiff facet joints and restoring their natural tracking, we instantly reduce the barrage of distress signals being sent into the trigemino-cervical nucleus, effectively "turning off" the headache at its source.
Suboccipital Soft Tissue Release
To address the muscular component, soft tissue therapy is aggressively applied to the upper kinetic chain, including the sternocleidomastoid (SCM), upper trapezius, levator scapulae, and suboccipital muscles.
Physiotherapists often perform a "suboccipital release." The therapist cradles the base of the patient's skull and applies deep, sustained ischemic pressure to the tight muscle bellies just under the occipital ridge. This prolonged pressure starves the contracted muscle of oxygen locally for a brief moment, forcing the tissue to reflexively release. This down-regulates the local nervous system, frees the trapped Greater Occipital Nerve, and rapidly diminishes the throbbing tension at the base of the head.
Corrective Exercises: The Deep Neck Flexors
The final, and most crucial, step for long-term resolution is rebuilding the structural integrity of the neck to prevent the headache from returning next week. If the suboccipital muscles at the back of the neck are overly tight, the opposing muscles at the front of the neck—the Deep Neck Flexors (DNFs), specifically the longus colli and longus capitis—are almost universally weak, overstretched, and neurologically inhibited.
The DNFs are essentially the intrinsic "core muscles" of your cervical spine. Corrective exercise protocols focus heavily on isolating and strengthening these muscles.
The primary intervention is the Cranio-Cervical Flexion exercise (often simplified as a highly specific "chin tuck"). Patients are taught to create a subtle "double chin" without aggressively jamming the head backward or engaging the large superficial neck muscles (like the SCM). This highly controlled micro-movement trains the body to stabilize the heavy skull directly over the shoulders, permanently correcting the forward-head posture that caused the mechanical overload in the first place.
Ergonomic Optimization
Even the best manual therapy will fail if the patient returns to an environment that enforces terrible posture for 8 hours a day. Our physiotherapists provide robust ergonomic coaching, including:
Monitor Height: Ensuring the top third of the computer screen is directly at eye level to prevent constant neck flexion.
The 20-20-20 Rule: Taking a break every 20 minutes to look at an object 20 feet away for 20 seconds. This simple act frequently breaks the sustained isometric tension on the suboccipital muscles.
Thoracic Extension: Utilizing tools like a lumbar roll or a foam roller to keep the mid-back (thoracic spine) upright, as a slumping upper back forces the neck to compensate.
Treatment Phase Breakdown for Cervicogenic Headaches
Rehabilitation PhasePrimary Interventions & ModalitiesClinical Objective
Phase 1: Symptom Down-Regulation
Suboccipital myofascial release, gentle cervical traction, postural offloading, ischemic compression.
Reduce acute nerve irritation, alleviate active headache intensity, and relax hypertonic neck musculature.
Phase 2: Joint Restoration
Specific upper cervical (C1-C3) joint mobilizations (e.g., SNAGs), Thoracic spine manipulation (to improve upper back extension).
Un-jam restricted facet joints, restoring full, pain-free rotation and flexion of the neck, confirmed via the CFRT test.
Phase 3: Motor Control & Stabilization
Deep Neck Flexor (DNF) strengthening, Cranio-Cervical Flexion exercises, Scapular retraction training.
Correct the structural imbalance (Upper Cross Syndrome) and build the localized muscular endurance necessary to hold the heavy skull upright without fatigue.
Phase 4: Functional Resilience & Ergonomics
Dynamic upper body strengthening, multi-planar resistance band exercises, strict desk setup modifications.
Ensure the neck and shoulders can tolerate high-volume daily loading (e.g., 8-hour computer workdays) without triggering a headache relapse.
Author Biography
Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist.
Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:
The content provided in this article is for general educational and informational purposes only and does not constitute formal medical advice. Severe headaches can occasionally be a symptom of serious medical pathology, including vascular issues or high blood pressure. Individual responses to physiotherapy vary, and Rehab Mechanics does not guarantee specific treatment outcomes. An in-person assessment is legally and clinically required to rule out red flags, definitively diagnose the specific cause of head or neck pain, and obtain informed consent before commencing care.