Overcoming Epicondylitis: Targeted Treatments for Tennis and Golfer’s Elbow
Chronic elbow pain is uniquely frustrating and surprisingly debilitating. Because our hands are our primary tools for interacting with the world, it severely hinders our fundamental ability to grip objects, lift heavy groceries, twist tight doorknobs, pour coffee, and perform the most basic, everyday manual tasks without wincing.
At Rehab Mechanics, we provide highly specialized, scientifically validated, and aggressively progressive clinical protocols to thoroughly resolve both Tennis Elbow and Golfer's Elbow efficiently, getting you back to your sport, your instrument, or your workday without nagging pain.
Defining Epicondylitis
"Epicondylitis" is the formal clinical medical term for a highly specific, very common form of tendinopathy that occurs directly at the elbow joint. It is characterized by deep, aching pain, highly localized inflammation, and most importantly, progressive cellular micro-tearing and degeneration of the vital tendons.
These tendons serve a crucial purpose: they bundle together and attach your powerful, bulky forearm muscles to the prominent, palpable bony bumps (the epicondyles) on either side of your lower humerus at the elbow. When these anchor points fail, the entire forearm mechanism is compromised.
Lateral vs. Medial Epicondylitis
While they share very similar, almost identical pathological mechanisms and cellular tissue degradation processes, they affect distinctly different tendon groups based entirely on your specific, repetitive movement patterns.
Lateral epicondylitis (commonly known worldwide as Tennis Elbow) affects the common extensor tendons on the outer, lateral side of the elbow. In contrast, medial epicondylitis (Golfer's Elbow) affects the common flexor tendons on the inside, medial aspect of the elbow, closest to your body. Both conditions severely impact grip strength, but trigger pain on opposite sides of the joint.
Biomechanics of the Forearm
Despite their sporty, highly specific nicknames, these conditions are very rarely caused by playing tennis or golf alone; they are classic, textbook chronic repetitive strain injuries (RSI).
Any daily activity that requires heavy, sustained, or highly repetitive gripping combined with rapid wrist extension or flexion can severely and chronically overload these delicate tendons. In our bustling Queen West clinic, we see this most often from poor, un-ergonomic typing setups, repetitive mouse clicking for 8 hours a day, heavy, uncontrolled weightlifting, and manual trades like construction, carpentry, or plumbing.
Micro-trauma in Extensor Tendons
In the case of Tennis Elbow, this relentless, repetitive, daily stress causes microscopic trauma specifically in the Extensor Carpi Radialis Brevis (ECRB) tendon, a relatively small muscle responsible for cocking the wrist back and stabilizing it during gripping.
Because tendons inherently suffer from poor, limited blood flow, the body's natural, biological healing cascade struggles to repair these microscopic tears fast enough to keep up with the daily damage. This leads to a permanent state of "failed healing" (clinically called tendinosis), characterized by chronic, low-grade aching pain, severe structural weakening, and physical disorganization of the tendon's collagen fibers, making it highly susceptible to sudden rupture.
Evidence-Based Treatment at Rehab Mechanics
Passive, old-school treatments like simply resting completely, popping anti-inflammatories, or blindly icing the elbow are almost never enough to cure chronic, degenerative epicondylitis; they merely mask the symptoms temporarily while the tissue continues to degrade.
Our clinic utilizes advanced, active loading strategies and cutting-edge modalities to physically remodel, thicken, and strengthen the damaged tendon tissue from the inside out, creating a permanent, resilient fix.
Comprehensive Load Management
The first crucial, non-negotiable step in our clinical protocol is identifying and temporarily modifying the specific daily activities that are actively aggravating your elbow. We do not want you to stop moving or immobilize the arm, but we must strictly control the strain.
Once the acute, highly painful flare-up is managed through manual therapy and modalities, we implement a highly specific, carefully progressive loading protocol. This is designed to safely build stress capacity and mechanical tolerance back into the tendon without causing further destructive micro-trauma or setting you back to square one.
Eccentric Strengthening Programs
The absolute cornerstone of modern, evidence-based tendon rehabilitation is eccentric exercise. This is a highly specific protocol that focuses on heavily, slowly loading the muscle while it is actively lengthening under tension, rather than shortening (concentric).
This specific, high-tension mechanical stress uniquely stimulates the tendon cells (tenocytes) to synthesize new, healthy collagen. Furthermore, the eccentric tension actively aligns those brand-new tissue fibers properly along the line of stress, smoothing out the disorganized scar tissue and rebuilding the tendon thicker, stronger, and far more resilient than before the injury.
The Tyler Twist Protocol
For our patients suffering from debilitating Tennis Elbow, we frequently utilize specialized clinical tools like the Theraband FlexBar to teach, cue, and execute the "Tyler Twist."
This specific, highly researched eccentric exercise protocol has been clinically proven in multiple, peer-reviewed sports medicine studies to dramatically reduce elbow pain, restore dense, healthy muscle tissue, and massively improve functional grip strength in patients suffering from even the most stubborn, long-standing cases of lateral epicondylitis. It puts the power of healing directly into the patient's hands.
The Road to Recovery: Comprehensive Rehabilitation After a Knee Injury or Replacement
The knee is an incredibly complex, but inherently vulnerable joint. Whether you've suffered a sudden, devastating sports injury on the soccer field, twisted it awkwardly stepping off a slippery Toronto streetcar in the winter, or recently undergone major joint replacement surgery due to severe, bone-on-bone osteoarthritis, the path back to normalcy is challenging.
However, regaining full, confident, and pain-free knee function runs directly through focused, progressive, and targeted physiotherapy. At Rehab Mechanics, we guide you through every phase of tissue healing, mobility restoration, and strength building.
Vulnerabilities of the Knee Joint
To truly understand why knee injuries are so prevalent, you must understand its architectural predicament. The knee is a massive, major weight-bearing hinge joint, precariously situated directly between the body's two longest and most powerful lever arms: the femur (the heavy thigh bone) and the tibia (the shin bone).
Because it is caught in the middle of these two massive bones, this anatomy subjects the knee joint to absolutely massive rotational, shearing, and compressive forces during any dynamic movement, jumping, heavy lifting, or sudden changes of direction. It is essentially a hinge trying to perform in a multi-directional world, making it highly susceptible to torque-related trauma.
Common Knee Injuries Explained
Unlike the hip, which sits in a deep, highly stable bony socket, the knee relies heavily on soft tissues—ligaments, tendons, and cartilage—for its stability rather than deep bony architecture.
Consequently, acute injuries generally involve traumatic, tearing damage to the meniscus (the two critical, C-shaped pads of tough fibrocartilage that act as vital shock absorbers and joint lubricators between the bones) or the four primary stabilizing ligaments (the ACL, PCL, MCL, and LCL) that strap the bones together like strong ropes and prevent excessive, dangerous shifting.
Ligamental Tears
Tears to the crucial ligaments, particularly the highly discussed Anterior Cruciate Ligament (ACL), dramatically and instantly compromise the entire structural stability of the joint. Patients often report hearing a loud "pop" followed by massive swelling, and the knee often feels like it will "give out" or buckle under your own body weight.
Depending on the severity (from a mild Grade I sprain to a complete Grade III rupture), these injuries may require specialized rigid bracing, extensive conservative rehab to strengthen surrounding muscles to compensate for the lost ligament, or complex, invasive surgical reconstruction. Regardless of the path chosen (surgical or conservative), all scenarios absolutely require meticulous, rigorous, months-long physiotherapy management to restore function safely and prevent early-onset arthritis.
The Mechanism of a Pivot-Shift Injury
The classic, most common way to completely tear an ACL in sports is via a non-contact "pivot-shift" mechanism. This usually occurs during a sudden, rapid deceleration combined with a violent change of direction—such as planting the foot firmly on the turf while the upper body twists and the knee violently collapses inward (a state called dynamic valgus).
Rehabilitating this devastating injury requires far, far more than just strengthening the quadriceps muscles on leg extension machines. It requires completely re-training the central nervous system's neuromuscular control, proprioception (body awareness), and landing mechanics to recognize and actively, reflexively prevent this dangerous valgus collapse from ever happening again upon return to sport.
Post-Operative Physiotherapy at Rehab Mechanics
For patients whose structural damage is so severe that it necessitates orthopedic surgery (like an ACL reconstruction, meniscus repair, or joint replacement), rigorous, supervised post-operative physiotherapy is undeniably the single most critical factor in determining the long-term success of the procedure.
A great surgeon can fix the anatomy, but physiotherapy restores the function. Our protocols are designed to minimize permanent, restrictive scar tissue, safely guide the healing graft, and dictate whether you will safely return to your normal, active lifestyle or be plagued by chronic stiffness.
Total Knee Replacements (TKR)
We successfully guide countless older Toronto patients through the arduous, highly painful, but ultimately life-changing and highly rewarding process of Total Knee Replacement (TKR) rehabilitation.
Our early clinical focus in the days and weeks immediately following surgery is paramount: safely controlling the massive, pooling post-operative swelling, managing the acute surgical pain, preventing the formation of highly dangerous deep vein thrombosis (blood clots), and safely, progressively loading the brand-new titanium and plastic joint to build tissue tolerance and bone integration.
Restoring Range of Motion
The absolute primary, most time-sensitive, and often most painful goal immediately following a TKR is restoring full, active knee extension (the ability to lock the leg completely straight) and deep knee flexion (bending).
This window of opportunity is incredibly short; if aggressive, daily mobility work isn't done early, dense, fibrotic scar tissue (arthrofibrosis) can rapidly form inside the joint capsule. This scar tissue acts like internal superglue, permanently cementing the knee into a bent, severely restricted position that will cause a lifelong, painful limp and make ascending stairs nearly impossible.
Patellar Mobilization Techniques
To facilitate that deep, necessary bending required for normal, everyday activities like smoothly climbing stairs, getting out of a low car seat, or picking something off the floor, the kneecap (patella) must be able to glide smoothly, effortlessly, and without grinding up and down over the new prosthetic joint mechanism.
Our physiotherapists utilize highly specific, manual patellar mobilization techniques to actively stretch the tight, surgical retinaculum and forcefully prevent the kneecap from adhering to the underlying healing tissues. By breaking up these early adhesions, we ensure the newly reconstructed knee regains its fluid, natural, and pain-free biomechanics, allowing for a full return to functional life.
Navigating Rotator Cuff Injuries: From Frozen Shoulder to Full Mobility
Shoulder pain is uniquely disabling and deeply frustrating. Because human beings rely on our arms and hands for almost everything we do in a day, a compromised shoulder can make incredibly simple daily tasks feel completely impossible. Reaching for a high shelf in the kitchen, putting on a winter coat, or even trying to find a comfortable position to sleep on your side become monumental, painful hurdles.
At Rehab Mechanics, we specialize in diagnosing and systematically rehabilitating the highly complex, delicate machinery of the shoulder complex, with a particular, specialized expertise in managing and healing debilitating rotator cuff injuries.
Anatomy of the Shoulder Complex
The human shoulder is technically a ball-and-socket joint (the glenohumeral joint), but it is very structurally different from the ball-and-socket of the hip. Unlike the deep, incredibly stable bony socket of the hip joint, the shoulder's socket is incredibly shallow—often compared by anatomists to a golf ball sitting precariously on a small golf tee.
This unique, evolutionary design is a trade-off: it grants the shoulder an incredible, nearly 360-degree range of motion, allowing us to throw, swim, and climb. However, it comes at a steep physiological cost: it makes the joint inherently unstable and prone to subluxation. To prevent dislocation, the shoulder relies almost entirely on a complex, perfectly timed web of dynamic muscles, tendons, and ligaments for its structural support, rather than deep bones.
The Four Rotator Cuff Muscles
The most critical of these dynamic stabilizers is the famous rotator cuff. This is not a single muscle, but a unified group of four relatively small but incredibly vital muscles: the supraspinatus, infraspinatus, teres minor, and subscapularis (often remembered by the acronym SITS).
Together, their tendinous attachments blend together to form a literal "cuff" that completely surrounds the head of the upper arm bone (humerus). It is a common misconception that these muscles primarily lift the arm. In reality, they act as a dynamic, intelligent corset. Their primary job is to fire rapidly and reflexively, pulling the head of the humerus firmly and securely down into the center of the shallow socket, stabilizing the joint while the much larger prime movers (like the massive deltoid and pectoral muscles) execute the heavy lifting and wide arm movements.
Mechanisms of Injury
Because these four muscles are remarkably small relative to the forces they manage, and because they are constantly working under high tension to prevent dislocation, they are highly susceptible to fatigue, micro-trauma, and severe injury.
Rotator cuff injuries typically fall into two distinct, broad categories. The first is acute, traumatic tears resulting from a sudden, forceful event, such as bracing for a fall with an outstretched hand, a violent tackle in rugby, or a sudden, uncontrolled heavy lifting accident. The second, and far more common category, is degenerative tendinopathy and micro-tearing caused by years of repetitive overhead motions (like painting or pitching), poor workplace ergonomics, and chronic postural rounding that shrinks the space in the shoulder joint.
Acute Tears vs. Degenerative Wear
While massive, full-thickness acute tears often cause complete loss of function and may require evaluation by an orthopedic surgeon for surgical repair, the vast majority of shoulder pain we see stems from degenerative wear, subacromial impingement syndrome, and partial-thickness tears.
These chronic conditions are highly responsive to specialized, conservative physiotherapy. Our primary clinical focus is on halting the vicious impingement cycle, drastically improving the biomechanics and resting posture of the shoulder blade (scapula), and systematically rebuilding the tensile strength and endurance of the rotator cuff tendon through targeted loading, all without exacerbating the already fraying, inflamed tissue.
The Spectrum of Shoulder Conditions We Treat
Beyond standard, simple tendonitis and bursitis (inflammation of the fluid-filled sac in the shoulder), our clinicians have the extensive experience and expertise required to handle highly complex, stubborn shoulder pathologies. We treat conditions that severely limit daily function, cause agonizing, sleep-depriving night pain, and threaten a patient's independence. We utilize a precise, constantly evolving mix of advanced manual therapy, joint mobilization, and progressive corrective exercise.
Frozen Shoulder (Adhesive Capsulitis)
Often misdiagnosed by primary care physicians or walk-in clinics as a simple rotator cuff tear, a "frozen shoulder" (clinically known as Adhesive Capsulitis) is a distinctly different, deeply frustrating, and poorly understood pathology.
It occurs when the strong, flexible connective tissue capsule that completely surrounds and encapsulates the shoulder joint inexplicably becomes severely inflamed, thickens dramatically, and eventually contracts and shrinks tightly around the bone. This process literally "freezes" the joint in place, severely and agonizingly restricting all planes of movement, particularly external rotation (the ability to reach behind your back or head).
The Three Stages of Frozen Shoulder
Treating a frozen shoulder requires immense patience and precise, strategic clinical timing; aggressively stretching the joint at the wrong stage will only inflame it further and prolong the disease.
Rehabilitation must be perfectly tailored to the specific stage of the condition:
The "Freezing" stage (lasting 2-9 months, characterized by severe, progressive, sharp pain and intense muscle spasms, especially at night).
The "Frozen" stage (lasting 4-12 months, where the acute pain lessens slightly, but the joint becomes rigidly stiff, immobile, and functionally useless).
The "Thawing" stage (lasting 5-24 months, where the capsule slowly begins to loosen and mobility gradually returns).
The "Thawing" Phase Interventions
During the critical "thawing" phase, our physiotherapists step in to aggressively but safely mobilize the stiffened glenohumeral joint and accelerate the recovery timeline.
We employ advanced, highly specific capsular stretching techniques, precise joint glides, and deep soft tissue release to the surrounding musculature to rapidly accelerate the breakdown of the thick capsular adhesions. We guide you safely and progressively back to your full, natural range of motion, ensuring you regain your independence and quality of life as quickly as physiologically possible.
Demystifying Shockwave Therapy: A Revolutionary Approach to Chronic Pain Relief
For patients struggling with incredibly stubborn, chronic injuries that have simply not responded to traditional treatments—like months of standard stretching, repetitive icing routines, or cortisone injections—Rehab Mechanics offers a powerful, technologically advanced, and scientifically backed solution: Extracorporeal Shockwave Therapy (ESWT).
If you feel like you have hit a wall in your recovery journey, or if your doctor has told you that you simply have to "live with the pain," this modality might be the exact biological catalyst your body desperately needs to overcome the plateau. It is rapidly becoming the gold standard in modern sports medicine and orthopedic rehabilitation.
The Science Behind Shockwave Therapy
Despite its somewhat intimidating name, modern shockwave therapy does not involve electrical shocks passing through your body. There is no electrocution or electrical stimulation involved. The technology actually originated from lithotripsy, the medical procedure used in hospitals since the 1980s to break up painful kidney stones without invasive surgery.
Instead of electricity, ESWT utilizes highly focused, high-energy acoustic (sound) waves generated by a specialized pneumatic handpiece. These mechanical sound pulses travel rapidly and are delivered directly through the skin into targeted, injured deep tissues to aggressively trigger, reboot, and accelerate the body's natural, biological healing cascades.
Mechanism of Action
The core philosophy of shockwave therapy is biological regeneration, not just symptom masking. When these powerful acoustic waves penetrate the dense, injured tissue (like a thick, scarred Achilles tendon or a rigid plantar fascia), they create highly controlled micro-traumas at the cellular level.
This intentional, microscopic damage is completely safe, but it is enough to stimulate a robust, localized inflammatory response. Essentially, the body has a tendency to "ignore" chronic injuries after a few months, deciding to just adapt around the dysfunctional tissue rather than heal it. Shockwave therapy violently interrupts this complacency. It tricks the central nervous system into recognizing an old, stagnant injury as a brand new, acute one, forcibly re-initiating the healing sequence in tissues that had completely stopped trying to repair themselves.
Cellular Level Healing
The mechanical pressure and sheer physical force of the acoustic shockwaves work physically as well as biologically. They act like a microscopic jackhammer to actively break down hard calcifications (calcium deposits), dense fibrotic adhesions, and restrictive, disorganized scar tissue that build up over years of chronic inflammation.
This scar tissue is vastly inferior to healthy tissue; it is rigid, lacks elasticity, physically restricts normal joint mobility, and causes painful, microscopic friction within joints, tendons, and ligaments during daily movement. By physically shattering these blockages, shockwave therapy restores the smooth, gliding nature of the body's connective tissues, drastically reducing localized friction and pain.
Neovascularization and Tissue Regeneration
Perhaps the most profound, exciting, and well-documented biological effect of shockwave therapy is a physiological process called neovascularization—the literal formation and growth of brand new microscopic blood vessels.
Chronic injuries, particularly in thick tendons and ligaments, are plagued by notoriously poor blood supply, which starves the tissue of necessary healing factors and oxygen. Shockwave dramatically increases this local capillary network. Within weeks of treatment, the area is flooded with fresh blood supply, vital oxygen, and regenerative nutrients (like growth factors and stem cells). This newly accelerated biological environment acts as the crucial foundation for the synthesis of new collagen and the total regeneration of healthy, elastic tendon and muscle fibers.
Conditions Treated with Shockwave
At our state-of-the-art clinic located conveniently inside the Prime Medical Centre on Abell Street, our therapists are specially trained to use shockwave therapy to effectively treat a wide array of the most stubborn, frustrating musculoskeletal conditions that plague active Torontonians. These include but not exclusive to chronic tendinosis, plantar fasciitis, tennis and golfers elbow.
Tendinopathies and Chronic Pain
Tendons are thick, fibrous cords that attach powerful muscle bellies to rigid bone. Because they inherently have a very poor blood supply compared to muscles, they are notoriously slow to heal and highly prone to chronic degeneration (tendinopathy).
Shockwave is now globally considered a gold-standard, first-line modality for chronic tendinopathies—such as patellar tendinitis (jumper's knee), proximal hamstring tendinopathy (runner's butt), and lateral epicondylitis (tennis elbow)—that have frustratingly lingered for six months or even multiple years without improvement from rest alone.
Plantar Fasciitis and Achilles Tendinopathy
Lower extremity, foot, and ankle injuries respond remarkably well to this specific acoustic modality, arguably better than any other part of the body. By deeply penetrating and breaking down the stiff, highly fibrotic tissue in the inflamed plantar fascia or the thick, load-bearing Achilles tendon, we can rapidly alter the tissue state.
Patients who have limped for months often find that shockwave rapidly reduces the excruciating morning stiffness and sharp, stabbing weight-bearing pain that define these debilitating conditions. It aggressively breaks the cycle of chronic inflammation and restores the natural elasticity required for normal walking mechanics and running gait.
Real Patient Outcomes
It is important to set proper expectations: while the treatment itself can be briefly uncomfortable (feeling like a rapid, deep tapping or snapping against the skin), patients typically experience a significant, measurable reduction in pain and an immediate, profound increase in mobility after just 3 to 5 targeted sessions, spaced about 5 to 7 days apart.
However, at Rehab Mechanics, we do not rely on machines alone. Shockwave heals the tissue, but it does not fix the bad habits that caused the injury in the first place. When seamlessly combined with our detailed biomechanical movement assessments, custom orthotics, and progressive, load-bearing strength training, shockwave therapy provides a comprehensive and permanent exit strategy from chronic pain, ensuring the injury does not return.
Understanding Sciatica: Causes, Symptoms, and Comprehensive Physiotherapy Solutions
Sciatica is unequivocally one of the most debilitating and distressing conditions we treat at Rehab Mechanics. The sharp, electric, shooting pain can bring daily life to a grinding halt, making simple acts like putting on socks, driving a car, or even sleeping feel like monumental tasks. The anxiety of not knowing when the pain will strike can be just as exhausting as the physical discomfort itself.
Many patients walk into our clinic terrified that they will need spinal surgery or will be dependent on painkillers for the rest of their lives. However, with the right targeted physiotherapy interventions, precise diagnostics, and a commitment to movement rehabilitation, resolving the root cause and achieving lasting relief is entirely possible.
What Exactly is Sciatica?
A common misconception is that "sciatica" is a specific medical diagnosis. In reality, sciatica is not a diagnosis in itself, but rather a descriptive symptom of an underlying mechanical issue. It refers to a specific type of nerve pain that radiates along the path of the sciatic nerve—the longest and thickest nerve in the human body, roughly the width of a man's thumb at its largest point.
This nerve branches from your lower back (the lumbar spine), runs deep through your hips and buttocks, and travels all the way down the back of each leg to your feet. Because the nerve spans such a massive geographical area of the body, irritation at its root in the back can be felt as agonizing pain in the calf or tingling in the toes. This is often confusing for patients who feel severe leg pain but have absolutely no back pain whatsoever.
Root Causes of Sciatic Nerve Pain
To effectively and permanently treat sciatica, we cannot simply mask the pain with medication; we must act as biomechanical detectives to first uncover exactly what structure is physically compressing, pinching, or chemically irritating the nerve. The culprit is almost always mechanical in nature, usually stemming from a structural failure in the lumbar spine.
Alternatively, sciatica-like symptoms can stem from severe tension in the deep gluteal musculature, a condition often referred to as Piriformis Syndrome. The piriformis is a small, external rotator muscle deep in the buttocks. In about 20% of the population, the sciatic nerve actually pierces directly through this muscle rather than running underneath it. When the piriformis spasms due to overuse (like long-distance running) or underuse (like sitting on a hard wallet all day), it acts like a vice grip on the nerve, perfectly mimicking true spinal sciatica.
Discogenic Injuries
The absolute most common cause of true sciatica is a discogenic injury originating in the lower back (typically at the L4-L5 or L5-S1 spinal levels, which bear the most mechanical load). The intervertebral discs are robust, shock-absorbing pads sitting between the vertebrae. They are built like jelly donuts, with a tough outer ring and a soft, gelatinous center.
When these discs become damaged—often due to years of poor lifting mechanics, prolonged sitting with a flexed spine, or sudden trauma—they can deform and physically encroach on the tiny, rigid space (the intervertebral foramen) reserved for the exiting nerve roots that eventually form the sciatic nerve. Even a millimeter of displacement in this tightly packed area can cause monumental pain.
Herniated vs. Bulging Discs
It is important to understand the clinical distinction between disc injuries. A bulging disc occurs when the tough, fibrous outer layer of the disc (the annulus fibrosus) weakens and physically protrudes outward, much like a hamburger patty sticking out of its bun. This usually causes a dull, aching pain and mild radicular symptoms.
A herniated disc is far more severe; it happens when this outer layer actually tears, allowing the soft, jelly-like inner core (the nucleus pulposus) to leak out. Both conditions physically compress the sciatic nerve, but the leaked material in a herniation is highly acidic to nervous tissue. It causes a massive, highly painful chemical inflammatory response, essentially "burning" the nerve root. This leads to intense radicular pain, numbness, tingling, and even profound muscle weakness in the leg, such as foot drop, where the patient cannot lift their toes while walking.
Physiotherapy for Sciatica at Rehab Mechanics
At our Toronto Queen West clinic, we specialize in non-invasive, highly effective, conservative treatments for sciatica. Surgery should always be a last resort, as spinal procedures carry immense risks and often fail to resolve the underlying mechanical failures.
Our primary clinical focus is on "centralizing" the pain. Centralization is a phenomenon where we use specific, repeated movements to draw the radiating leg pain back up the leg, into the buttocks, and eventually isolate it in the lower back. While having more back pain sounds counterintuitive, centralization is the definitive clinical hallmark of a healing nerve root. Once the dangerous leg symptoms resolve and the nerve is safe, we can actively stabilize the spine.
Our Treatment Strategy
We do not believe in a one-size-fits-all approach. Throwing a standard sheet of stretches at a sciatica patient often makes them substantially worse, especially if they are doing forward-bending stretches (like touching their toes) that actually increase disc pressure.
We utilize a customized, multidisciplinary combination of manual therapy, movement retraining (like the highly structured McKenzie Method of Mechanical Diagnosis and Therapy), and cutting-edge modalities. This multifaceted strategy works rapidly to reduce local nerve irritability, naturally decrease the inflammatory response, and mechanically resolve the underlying compression without the need for aggressive pharmaceuticals or prolonged bed rest, which is actually detrimental to recovery.
Manual Therapy and Spinal Decompression
Our hands-on manual therapy techniques aim to safely mobilize the stiff segments of the lumbar spine, relieve the intense, protective muscle spasms that lock up the lower back, and gently create vital anatomical space around the compromised nerve root.
Through targeted manual traction and specific joint mobilizations (Mulligan concepts), we can create negative pressure within the disc space. This vacuum effect can theoretically help draw bulging disc material back toward the center of the disc and away from the highly sensitive nerve root. We also utilize deep tissue release on the compensatory muscles—such as the QL (quadratus lumborum) and hip flexors—that have tightened up in an attempt to splint and protect the injured spine.
At-Home Nerve Gliding Exercises
To actively complement your in-clinic treatment and accelerate recovery, we prescribe highly specific nerve gliding (sometimes called neural flossing or nerve mobilization) exercises. When a nerve is irritated, it becomes inflamed and can become "sticky," adhering to the surrounding muscles and fascia. Because a healthy nerve needs to slide gracefully through the body as you move, a tethered nerve pulls painfully, resulting in shooting electrical pain.
These gentle, oscillatory micro-movements—such as seated slump glides or supine sciatic flossing—help safely mobilize the sciatic nerve through its protective sheath. By gliding the nerve back and forth like dental floss, we reduce tethering, clear out localized inflammatory swelling, and restore its natural excursion. This empowers you to actively manage and abort flare-ups independently from the comfort of your own home, giving you control over your recovery.
The Ultimate Guide to Correcting Postural Dysfunction in the Modern Workplace
Understanding Postural Dysfunction
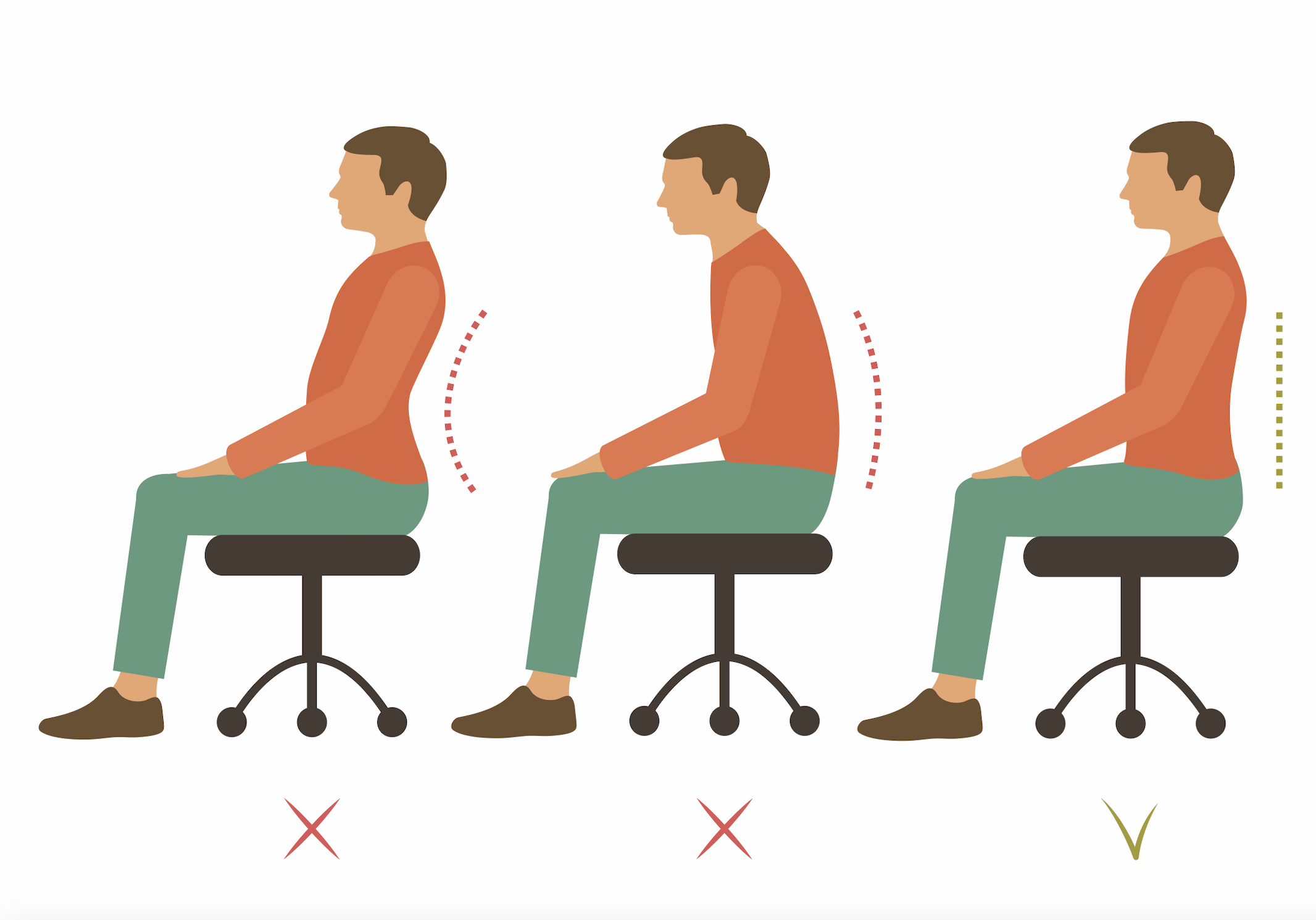
Postural dysfunction occurs when our spine and its accompanying joints deviate from their natural, neutral alignment for extended periods. This isn't just about looking "slouched"; it is a systemic biomechanical failure. This continuous deviation places unnatural, asymmetrical stress on ligaments, tendons, and muscles, leading to a cascade of painful symptoms across the body. When one area of the body falls out of alignment, the nervous system forces other areas to compensate, creating a domino effect of tension and fatigue.
Furthermore, poor posture significantly impacts your physiological and psychological state. Slouching physically compresses the diaphragm, limiting your lung capacity and forcing you into shallow, "apical" chest breathing. This shallow breathing signals to your nervous system that you are in a state of stress, subtly elevating your heart rate and cortisol levels. Over time, this creates a devastating feedback loop where physical misalignment feeds emotional fatigue, and fatigue further degrades your physical posture.
The Anatomy of the Spine Under Stress
The human spine is a marvel of biological engineering, designed with three natural, alternating curves (cervical lordosis, thoracic kyphosis, and lumbar lordosis) to act as a coiled spring. These curves are essential to absorb shock, distribute the weight of the head and torso evenly, and allow for explosive athletic movement. When these curves are compromised—either flattened out or exaggerated—the biomechanics of the entire body shift. This shift causes compensatory patterns that inevitably lead to joint degeneration, nerve compression, and significantly reduced mobility.
The muscles designed for quick, dynamic movements are suddenly forced to act as postural stabilizers, a job they inevitably fail at, resulting in painful spasms. For instance, your powerful latissimus dorsi and trapezius muscles are meant to pull and lift, not to hold your spine upright against gravity for ten hours a day. When forced into this stabilizing role, these muscles become ischemic (starved of blood flow) and develop dense, fibrotic trigger points that radiate pain into your neck, shoulders, and even down your arms.
The Impact of Modern Lifestyles
Our rapid transition to desk-bound, screen-heavy lifestyles over the last two decades has absolutely devastated our natural biomechanics. The human body evolved to walk, run, climb, and carry, not to sit statically for 8 to 12 hours a day. Prolonged sitting causes the hip flexors (psoas and iliacus) to chronically shorten, the gluteal muscles to essentially fall asleep (gluteal amnesia), and the shoulders to aggressively round forward.
This combination completely alters our center of gravity, placing immense shearing forces on the lower back discs and forcing the upper back muscles to fight a losing battle against gravity. In an urban environment like Toronto, this is compounded by the "commuter posture"—sitting on transit, carrying heavy messenger bags or unevenly loaded backpacks, and rushing through concrete streets. Your body adapts to the positions it spends the most time in; if you spend 80% of your day curled into a C-shape over a keyboard, your fascia and muscles will literally remodel themselves to lock you into that dysfunctional shape.
The "Tech Neck" Phenomenon
"Tech neck," or anterior head carriage, is a specific and highly destructive manifestation of poor posture where the head continuously juts forward toward a screen. In a neutral position, the adult head weighs about 10 to 12 pounds. However, physics dictates that for every single inch the head moves forward past the neutral shoulder line, the weight borne by the delicate cervical spine effectively doubles. This means looking down at a smartphone can place up to 60 pounds of force on the neck.
This relentless strain leads to chronic tension headaches, temporomandibular joint (TMJ) irritation, and premature discogenic injuries, such as bulging discs and pinched nerves in the cervical spine. If left unaddressed for years, the body responds to this excessive localized stress by laying down extra bone to reinforce the unstable area. These are known as osteophytes, or bone spurs. Once these bone spurs form, they can permanently narrow the space available for nerves exiting the neck, turning a correctable muscular issue into a permanent, irreversible structural pathology.
The Rehab Mechanics Approach to Posture
At Rehab Mechanics on Abell Street, we understand that simply telling a patient to "sit up straight" or "pull your shoulders back" is entirely ineffective. Posture is heavily influenced by the nervous system and long-standing muscular adaptations; it cannot be fixed by willpower alone. Trying to force yourself into "good posture" usually just results in arching the lower back excessively, which creates an entirely new set of problems.
We utilize a comprehensive, science-based approach combining advanced soft tissue therapy, specifically calibrated corrective exercises, and effective modalities to physically and neurologically restructure your postural habits from the ground up. Our goal is not to give you a rigid, military-style posture, but rather a dynamic, resilient, and relaxed neutral posture that requires minimal energy to maintain.
Comprehensive Biomechanical Assessment
Our experienced physiotherapists begin your journey with a thorough, full-body assessment of both your static posture and dynamic movement patterns. We look beyond the site of pain. We analyze individual joint mobility, precise muscle length and tension, and your baseline neurological function. By watching you perform fundamental movements like squats, lunges, and overhead reaches, we can pinpoint the exact muscular imbalances and joint restrictions that are secretly driving your poor posture and subsequent pain.
We also conduct a detailed ergonomic audit of your daily life. We discuss your desk height, monitor placement, the type of chair you use, and how often you take breaks. Often, we find that a patient's pain is continuously triggered by a monitor that is set 15 degrees too far to the left, or a chair that places their knees higher than their hips, which posteriorly tilts the pelvis and flattens the lumbar curve.
Targeted Clinical Interventions
Once the specific imbalances are accurately identified, we deploy targeted, hands-on clinical treatments to manipulate the tissues. We utilize techniques like active release, trigger point therapy, and joint mobilizations to release chronically overactive, tight muscles (such as the upper trapezius and pectorals) and stimulate underactive, inhibited ones (such as the lower trapezius and deep cervical flexors).
This manual reset is crucial for creating the physical space and joint freedom required to adopt a new, healthy posture. Think of it like trying to open a door with a rusted hinge; you cannot simply push harder. You must first clear the rust and lubricate the joint. Our manual therapy "clears the rust" from your soft tissues, removing the restrictive fascial adhesions that physically block you from standing up straight.
Corrective Exercise Protocols
Following manual therapy, we prescribe highly specific, progressive corrective exercises. These aren't your typical, generic gym stretches; they are tailored neuromuscular re-education drills. We focus on endurance over absolute strength, retraining your core, scapular stabilizers, and deep neck flexors to maintain your newly acquired alignment unconsciously.
By integrating these precise micro-movements into your daily routine—often right at your desk—we ensure that your body naturally defaults to a healthy, upright position without you having to constantly think about it. Exercises like "wall angels" and "chin tucks" become your daily medicine. We empower you with the physical literacy to understand when your posture is failing and the immediate tools to correct it before it translates into a painful spasm.
Ergonomics and Beyond: Managing Carpal Tunnel and De Quervain’s Tenosynovitis
In our modern, hyper-connected, fast-paced digital world, our hands, wrists, and thumbs endure an absolutely incredible, unnatural amount of repetitive daily stress. We swipe, type, click, and text thousands of times a day.
Consequently, painful, nerve-wracking, and severely limiting wrist injuries like Carpal Tunnel Syndrome and De Quervain’s Tenosynovitis are skyrocketing across all demographics, from young gamers to older administrative workers. However, Rehab Mechanics offers highly specialized, conservative, and ergonomic solutions designed to rapidly alleviate trapped nerve pain and restore full, pain-free hand and wrist function.
The Complexity of the Wrist
The human wrist is not a simple, single joint like a door hinge, but rather an incredibly complex, tightly packed, and highly articulated structural intersection. It is composed of eight intricately shaped, pebble-like small carpal bones, tightly bound together by a massive, complex web of rigid, interwoven ligaments.
Most importantly, it serves as a crowded, incredibly narrow anatomical conduit for all the vital, highly sensitive flexor tendons, major nerves, and blood vessels traveling from the powerful muscles of the forearm directly into the palm of the hand and the tips of the fingers. There is absolutely no extra room in this anatomical chokepoint.
Carpal Tunnel Syndrome (CTS)
Carpal Tunnel Syndrome (CTS) is by far the most well-known, frequently diagnosed, and heavily researched compression neuropathy of the upper extremity.
It is distinctly and unmistakably characterized by intense numbness, painful "pins and needles" tingling (paresthesia), deep burning pain, and eventual severe muscle weakness. Crucially, these symptoms specifically target the thumb, index finger, middle finger, and exactly half of the ring finger—which perfectly maps to the exact sensory distribution pathway of the median nerve. If your pinky finger is numb, it is generally not Carpal Tunnel, but a different nerve issue.
Anatomy of the Carpal Tunnel
The carpal tunnel itself is a rigid, unforgiving, extremely narrow passageway located on the palm side (volar aspect) of your wrist. It is formed by the curved carpal bones acting as the floor and walls, and a thick, incredibly tight, unyielding ligament (the transverse carpal ligament) acting as the solid roof.
When the protective, slippery sheaths (synovium) surrounding the nine flexor tendons that run through this crowded tunnel become inflamed and swell—very often due to poor typing ergonomics, sustained, awkward wrist flexion angles, or repetitive, forceful gripping—they rapidly run out of physical space. This swelling aggressively compresses the soft, delicate, vital median nerve that is hopelessly trapped within this rigid, bony box.
Median Nerve Compression Dynamics
Prolonged, unrelieved physical compression of the median nerve is incredibly destructive to the nervous system. It literally starves the nerve of vital blood flow (ischemia), physically strips the nerve of its protective, conductive myelin sheath, and severely disrupts vital axonal transport (the essential flow of nutrients and chemical signals up and down within the nerve).
Left untreated for too long, this chronic compression leads to permanent, irreversible sensory loss, the chronic, clumsy dropping of coffee cups and keys, and visible, permanent wasting away (atrophy) of the fleshy thenar muscles at the base of the thumb. Early, aggressive, conservative physiotherapy intervention is absolutely vital to halt this progression and prevent permanent nerve damage and the need for surgical release.
De Quervain’s Tenosynovitis
Commonly, yet somewhat inaccurately, referred to in pop culture as "Gamer's Thumb," "Texting Thumb," or "Mommy Thumb" (due to the highly awkward wrist mechanics required when repeatedly lifting heavy, growing infants), De Quervain’s Tenosynovitis is a highly painful, acute inflammatory condition.
It aggressively targets the tendons located specifically on the thumb side of your wrist, causing severe, sharp, breathtaking pain during simple gripping, tight pinching, or any forceful rotational wrist movements, such as pouring a heavy kettle, turning a stiff door key, or opening a tight jar.
The Mechanics of Thumb Tendinopathy
This specific, agonizing condition involves the severe inflammation, thickening, and subsequent swelling of the tight synovial sheath (the slick, protective tunnel) that surrounds and strictly houses two highly specific tendons responsible for controlling the outward and upward movement of the thumb: the extensor pollicis brevis and the abductor pollicis longus.
When this narrow sheath swells due to friction and overuse, these tendons experience massive, painful resistance and friction every single time the thumb moves, leading to agonizing pain that can radiate up the forearm.
Clinical Diagnosis and Finkelstein's Test
In our clinic, we can highly accurately diagnose this specific condition through a thorough, hands-on physical assessment and targeted provocative orthopedic testing, prominently utilizing a widely recognized clinical maneuver called Finkelstein’s test.
In this test, the patient tucks their thumb securely inside a closed fist, wrapping their fingers over it, and sharply deviates the wrist downward toward the pinky finger (ulnar deviation). If this specific movement elicits a sharp, blinding, "electric" pain directly over the radial styloid (the bony bump on the thumb side of the wrist), the test is strongly positive for De Quervain's.
Comprehensive Physiotherapy Management
Surgical release of these inflamed tissues should only be considered if all conservative measures strictly fail after months of effort. Comprehensive, conservative treatment for both CTS and De Quervain's at Rehab Mechanics includes immediate, aggressive workplace ergonomic redesign (like vertical mice and split keyboards).
We also utilize highly specific resting splinting recommendations to protect the area during sleep, aggressive deep soft tissue massage and active release of the tight forearm flexors and extensors, and specialized, targeted neuro-dynamic gliding exercises explicitly designed to gently free the trapped nerves and tendons from their restrictive surrounding tissues without causing further irritation.
Debunking the MRI Myth in Physical Therapy
Rethinking the Need for an MRI
Many individuals assume that a comprehensive MRI is the only pathway to kick-starting physical therapy. This belief often stems from the notion that advanced imaging is necessary to pinpoint the source of pain, yet in many cases, a thorough physical assessment can offer equally valuable insights. In this guide, you'll discover why the MRI myth persists and explore how focused clinical evaluations, rather than expensive imaging tests, can effectively guide your rehabilitation process.
Understanding your body’s mechanics doesn’t always demand high-tech diagnostics. Instead, consider these key points:
Clinical Assessment: Hands-on evaluations often reveal movement restrictions and muscle imbalances.
Cost and Time Efficiency: Skipping unnecessary imaging can reduce delays and expenses.
Local Expertise: Many community-based therapists use proven manual techniques to deliver swift recovery.
Read on to learn practical, actionable approaches that debunk the idea that complex imaging is a prerequisite for effective therapy. This introduction lays the groundwork for a deeper conversation on optimizing your recovery strategy without relying on extensive MRI scans.
Unlocking the Power of MRI in Diagnostics
Magnetic Resonance Imaging (MRI) stands as one of the most sophisticated techniques in medical diagnostics, using strong magnetic fields and radio waves to create intricate images of the body’s internal structures. This non-invasive imaging tool is indispensable in revealing details about soft tissues, organs, and joints that other diagnostic methods might overlook. Its high-resolution capabilities are particularly valuable in detecting conditions ranging from ligament injuries to subtle abnormalities in the brain and spine.
When approaching MRI as a diagnostic method, keep these key points in mind:
Safety and Precision: With no exposure to ionizing radiation, MRIs offer precise imaging without many associated risks.
Versatility: They are effective for evaluating a wide range of issues including musculoskeletal injuries, neurological conditions, and inflammatory diseases.
Local Accessibility: Many clinics and imaging centers in urban and suburban areas now provide convenient, high-quality MRI services, ensuring patients receive accurate assessments quickly.
Understanding how MRI operates not only helps clarify its role in comprehensive healthcare but also empowers you to ask informed questions about your diagnostic options.
Rethinking Diagnostic Imaging Before Therapy
Before diving into an active physical therapy plan, it's important to understand that MRIs aren’t always a prerequisite for effective treatment. Many seasoned physiotherapists prioritize detailed patient history and a comprehensive physical evaluation over immediate imaging, especially when the signs and symptoms suggest common musculoskeletal issues. This approach not only minimizes unnecessary delays but also helps reduce the healthcare costs for patients across local communities.
Consider these practical points:
Thorough Clinical Assessment: A hands-on evaluation by a skilled therapist can identify functional impairments without the need for advanced imaging.
Timely Intervention: Starting targeted therapy based on physical findings can accelerate recovery and prevent further injury.
Resource Optimization: Avoiding immediate MRIs supports efficient use of medical resources, making advanced imaging available for cases where it’s truly warranted.
By emphasizing clinical judgment and evidence-based practice, patients receive personalized care that addresses their unique needs. Additionally, local clinics and therapy centers are increasingly adopting these protocols, ensuring that treatment plans are both practical and effective. This proactive approach not only streamlines the path to recovery but also educates patients on the value of functional assessments.
Speeding Recovery: Embrace Early Physical Therapy
Starting physical therapy before MRI results are available can pave the way for a faster recovery and more efficient intervention. Delaying treatment in hopes of diagnostic clarity often hinders timely rehabilitation. Early physical therapy focuses on addressing pain, mobility issues, and functional limitations that can be alleviated through targeted exercises and manual techniques. By initiating treatment promptly, you can prevent the escalation of injury and improve overall outcomes.
Key benefits include:
Accelerated recovery: Engage in customized mobility exercises sooner to restore strength and flexibility.
Minimized discomfort: Early intervention targets pain relief through hands-on therapy and structured rehabilitation strategies.
Proactive management: Address movement imbalances and muscle weaknesses before they lead to more serious complications.
Localized support: In urban centers and suburban areas alike, nearby clinics offer community-based programs designed to meet your specific recovery goals.
Utilizing early physical therapy in the local area ensures that you receive expert guidance quickly, enabling your body to begin healing right away. This approach not only preserves functional fitness but also empowers you with practical strategies to maintain mobility and reduce the risk of future injuries.
FAQ: Demystifying MRI Use in Physical Therapy
What does an MRI actually show about my injury? MRIs provide detailed images of the body’s soft tissues and bones. However, they capture the static structure and may not reveal dynamic or functional issues, which are crucial for effective physical therapy. A thorough clinical exam often complements these images to create a complete picture.
Is an MRI needed before starting physical therapy? Not necessarily. Many patients can begin therapy based on clinical findings alone. MRIs are typically reserved for complex cases where the source of pain or dysfunction remains unclear after a physical examination.
Can MRI results sometimes lead to misguided treatment plans? Yes, sometimes the detailed images can introduce uncertainty if interpreted without context. It’s essential that physical therapists integrate MRI findings with hands-on assessments to tailor interventions.
How do physical therapists utilize MRI data in treatment planning? Therapists use MRI results to confirm structural issues, but they emphasize functional testing and patient history to devise a customized rehabilitation plan.
What alternatives exist for injury assessment? Beyond MRIs, clinical tests, range-of-motion analyses, and strength evaluations are valuable tools in crafting effective physical therapy strategies.
Decoding the Criteria for MRI Necessity in Physical Therapy
Healthcare providers use a systematic approach to determine when an MRI is truly necessary in physical therapy cases. Initially, clinicians conduct a comprehensive evaluation, combining a detailed patient history with an extensive physical examination. They assess symptoms such as persistent pain, restricted range-of-motion, and neurological signs, which serve as red flags for potential structural damage.
The decision-making process often includes:
Symptom Analysis: Reviewing the intensity, duration, and progression of discomfort.
Physical Testing: Performing targeted maneuvers to pinpoint areas of concern.
Clinical Judgment: Balancing diagnostic imaging with conservative treatment options.
Providers consider whether the benefits of an MRI outweigh the risks and costs, factoring in the likelihood of finding actionable abnormalities. For example, patients experiencing acute trauma or those with unusual neurological deficits may be prioritized for imaging. This careful, step-by-step assessment not only helps in avoiding unnecessary tests but also promotes efficient recovery strategies. In urban centers and local clinics, this protocol ensures that imaging resources are used judiciously, ultimately enhancing patient care and therapeutic outcomes.
Wrapping Up: Embrace Clarity and Confident Choices
As you reach the end of this discussion, it’s vital to reflect on the key insights that have emerged. The longstanding myth linking MRI scans directly to finding the root cause of pain is debunked when viewed through the lens of contemporary physical therapy practices. Instead of relying solely on imaging, modern treatment emphasizes comprehensive evaluations and tailored exercise programs that address the underlying mechanics of discomfort.
Moving forward, consider taking these actionable steps:
Engage in an in-depth discussion with your healthcare provider to explore a thorough physical assessment.
Prioritize finding local professionals who practice evidence-based methodologies.
Keep an open mind about alternative diagnostic approaches that focus on functional movement and recovery.
Arming yourself with accurate information and expert advice is the first step towards a more effective rehabilitation journey. Remember, personalized physical therapy can offer a more practical and holistic approach to managing pain. Take charge of your health by analyzing your options and consulting trusted professionals—empower yourself to make informed decisions and embrace a future of improved wellness.