Can Physiotherapy Permanently Cure Plantar Fasciitis Without Custom Orthotics?
Yes and NO. While custom orthotics provide immediate offloading for severe cases, physiotherapy is the definitive cure. By restoring ankle dorsiflexion, mobilizing the plantar fascia, and strengthening the intrinsic foot muscles, physical therapy rebuilds your foot's natural shock-absorbing capacity.
The "Glass Shard" in the Heel
There are few sensations more painful than the first few steps out of bed in the morning. For many Torontonians—especially those who spend their days on their feet or those who have recently increased their running volume—that first step feels like a glass shard or a dull, deep ache stabbing directly into the heel.
This is Plantar Fasciitis. It is one of the most common, yet frequently misunderstood, pathologies we treat at Rehab Mechanics. Patients are often told to "roll a frozen water bottle under your foot" or buy expensive, passive arch supports. While these provide temporary relief, they do not resolve the mechanical failure of the foot. To truly defeat plantar fasciitis, you must restore the mobility of your ankle and the intrinsic strength of your arch.
Structural Analysis: The Mechanics of Foot Pain
The plantar fascia is not just a strip of tissue; it is a vital, high-tension ligament that controls the entire biomechanical function of your foot.
The Windlass Mechanism
The plantar fascia connects your heel bone (calcaneus) to the base of your toes.
The Arch Spring: When you step down, the fascia stretches like a high-tension spring to absorb the shock of your weight.
The Lever: When you prepare to push off your toes, the fascia winds tightly, turning your foot into a rigid, powerful lever for walking or running.
The Failure of the Shock Absorber
Plantar fasciitis is not "inflammation" (itis). It is actually plantar fasciopathy—a state of chronic cellular degeneration caused by repetitive mechanical overload.
Ankle Stiffness: If your ankle (talocrural joint) is stiff and cannot bend forward (dorsiflexion), your foot is forced to compensate. The arch collapses inward (overpronation) to allow the foot to move forward.
The Sheer Force: This constant, aggressive collapse places massive tensile stretching forces on the fascia, leading to microscopic tears, scar tissue build-up, and localized bone-spur development.
Primary Source Proof: Biomechanical Rehabilitation
Scientific literature supports the use of progressive mechanical loading and ankle mobilization as the most effective path to curing chronic heel pain, proving that passive arch support is insufficient for long-term resolution.
The Rehab Mechanics Foot Reconstruction Protocol
We treat plantar fasciitis by rebuilding the mechanical health of the entire leg, starting from the ground up.
Phase 1: Tissue Decompression and Shockwave Therapy
Before we strengthen, we must clear the fibrotic, scarred tissue.
Shockwave Therapy: We use high-energy acoustic waves to break down the dense, painful scar tissue in the fascia and stimulate new, healthy blood vessel growth in the degenerated heel.
Myofascial Release: Deep, manual release of the calf muscles (gastrocnemius and soleus). If your calf is tight, your ankle cannot move, and your fascia will remain under constant tension.
Phase 2: Ankle Dorsiflexion Restoration
We must restore the joint's ability to bend, which is the root cause of the arch collapse.
Manual Joint Mobilizations: Our physiotherapists use hands-on techniques to force the talocrural joint to glide properly, ensuring the ankle can bend freely without relying on arch collapse.
Dynamic Calf Stretching: Progressive lengthening of the posterior chain to ensure full ankle range of motion during walking.
Phase 3: The Rathleff Protocol (High-Load Strengthening)
We rebuild the foot's structural integrity using heavy loading.
The Rathleff Protocol: A specific, heavy-load strength protocol using a rolled towel under the toes to maximally activate the plantar fascia while performing calf raises. This has been clinically proven to be the most effective intervention for resolving heel pain.
Intrinsic Foot Strengthening: Exercises like "foot doming" or toe-splaying to rebuild the tiny, dormant muscles inside the foot that are designed to support your arch, rendering the need for permanent orthotics obsolete.
Restore Your Foundation
You do not have to live with the morning hobble. By rebuilding your ankle mobility and foot strength, you can permanently resolve heel pain.
Book a comprehensive foot and ankle assessment today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:

Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.



Can Physiotherapy Fix Shoulder Impingement Without Surgery?
Yes. Physiotherapy is the most effective treatment for shoulder impingement syndrome. By correcting scapular dyskinesis, restoring thoracic mobility, and strengthening the rotator cuff to hold the arm bone perfectly centralized in the socket, physiotherapy physically eliminates the friction causing your pain.
The Overhead "Catch"
For the active demographic in Queen West, your shoulder is your most important tool. Whether you are lifting a heavy barbell in the gym, playing a recreational tennis match, or reaching overhead to grab a high shelf in your apartment, the shoulder must move with fluid, frictionless precision.
When you start to feel a sharp, stabbing "catch" or "pinch" in the front of your shoulder whenever you lift your arm above head height, it is a sign that your shoulder is not moving correctly. The medical term is Shoulder Impingement Syndrome. It is incredibly common, often dismissed as "just a strain," and frequently managed incorrectly with ice and rest.
At Rehab Mechanics, we see patients who have lived with this impingement for years. They worry they have a "torn rotator cuff" and fear surgery. The reality is often much simpler: your shoulder blade is not moving in sync with your arm bone. By correcting this mechanical timing, we can eliminate the pinch immediately and prevent the development of a chronic rotator cuff tear.
Structural Analysis: The Mechanics of Impingement
To understand why your shoulder pinches, we must look at the "subacromial tunnel"—the narrow, bony bottleneck through which your tendons must travel.
The Subacromial Bottleneck
Your shoulder joint is a ball-and-socket, but the "socket" is roofed by a bony prominence called the acromion.
The Tunnel: Between the ball (the arm bone) and the roof (the acromion) is a narrow, tunnel-like space.
The Contents: Through this tunnel pass your vital rotator cuff tendons and a fluid-filled sac called the subacromial bursa.
The "Crush" Mechanism (Impingement)
In a healthy shoulder, your rotator cuff muscles pull the ball of the arm bone downward, keeping it low in the socket as you lift your arm. This keeps the tunnel wide and open.
The Breakdown: If your rotator cuff is weak, or if your shoulder blade (scapula) is stiff, the arm bone slides upward too early during the lift.
The Impingement: The top of the arm bone smashes into the roof of the tunnel (the acromion). This physically crushes the rotator cuff tendon and the bursa against the bone.
The Result: Sharp, blinding pain, often followed by a dull, throbbing ache that lasts for hours after the lift.
Primary Source Proof: Impingement Rehabilitation
Sports medicine research conclusively mandates that physiotherapy is the first-line treatment for shoulder impingement, often achieving superior long-term results compared to surgical decompression.
Download Clinical Efficacy PDF: The Efficacy of Conservative Physical Therapy versus Surgical Decompression in Shoulder Impingement Syndrome (Open Access Medical Review)
The Rehab Mechanics Corrective Protocol
We treat impingement not by massaging the painful spot, but by fixing the biomechanics of the entire shoulder girdle.
Phase 1: Decompressing the Tunnel
We must stop the bone-on-bone grinding immediately.
Posterior Capsule Mobilization: A stiff back-of-the-shoulder capsule pushes the arm bone forward into the impingement zone. Our therapists use high-grade manual glides to loosen this tissue.
Manual Release of the Pectoralis Minor: A tight chest muscle physically drags the shoulder blade into a forward tilt, narrowing the subacromial tunnel. We release this tension to restore scapular alignment.

Phase 2: Restoring Scapulothoracic Rhythm
We must teach your shoulder blade how to get out of the way of your arm bone.
Lower Trapezius and Serratus Anterior Activation: These muscles pull the shoulder blade down and back, physically opening the tunnel. We use targeted resistance work to ensure these muscles fire automatically during overhead movements.
Neuromuscular Re-education: We use tactical cueing to retrain the brain to keep the shoulder blade "set" firmly against the ribcage as you lift, preventing the "hike-and-hunch" compensation pattern.
Phase 3: Rotator Cuff Fortification
Once the joint is mechanically safe, we build the strength to hold the ball centered in the socket.
Eccentric Rotator Cuff Loading: Using targeted resistance training to rebuild the tendons. A strong rotator cuff is the only structural guarantee that the arm bone stays centralized in the socket, permanently preventing impingement.
Reclaim Your Overhead Power
Stop letting a pinching shoulder limit your training or your daily life. Fix the mechanics, and the pain disappears.
Book your comprehensive shoulder assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite orthopedic recovery in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Fix a SLAP Tear in My Shoulder Without Surgery?
Yes. Physiotherapy successfully treats SLAP tears without surgery by restoring scapular mechanics and strengthening the dynamic stabilizers of the rotator cuff. This active rehabilitation reduces the sheer force on the labrum, stabilizing the biceps anchor and allowing the shoulder to function pain-free.
The Agony of the Overhead Athlete
In Toronto’s active core, particularly among the dedicated functional fitness, CrossFit, and weightlifting communities in Liberty Village and Queen West, shoulder injuries are a constant threat. One of the most terrifying diagnoses an athlete can receive is a SLAP lesion—a specific, deep tear in the cartilage of the shoulder socket.
The symptoms are deeply frustrating: a profound, deep-seated ache inside the shoulder joint, a sharp "catching" or "popping" sensation when lowering a heavy barbell or throwing a ball, and a sudden, inexplicable loss of overhead strength. When an MRI confirms a SLAP tear, patients frequently panic, assuming their athletic career is over unless they undergo an invasive arthroscopic repair, which carries a brutal 6-to-9-month recovery timeline.
At Rehab Mechanics, we want to shift this narrative. While massive, traumatic labral avulsions may require surgery, the vast majority of degenerative or overuse SLAP tears can be managed conservatively. A tear in the labrum is often the victim of poor shoulder mechanics, not the primary culprit. By overhauling how your shoulder blade and rotator cuff handle load, expert physiotherapy can silence the pain and restore your overhead power without a scalpel.
Structural Analysis: The Mechanics of a SLAP Lesion
To understand how physical therapy can save your shoulder, we must perform a detailed biomechanical analysis of the labrum and its connection to the rest of the arm.
Anatomy of the Biceps-Labrum Complex
Your shoulder is a ball-and-socket joint, but the socket (the glenoid) is extremely shallow—often compared to a golf ball sitting on a tee.
The Labrum: To deepen this shallow socket and create a stabilizing "suction cup" effect, a ring of tough fibrocartilage called the labrum wraps around the rim of the bone.
The Biceps Anchor: The long head of your biceps tendon travels up your arm and attaches directly into the very top (the superior portion) of this labral ring.
What is a SLAP Tear?
SLAP stands for Superior Labrum Anterior and Posterior. It means the top of the cartilage ring has been torn from front to back, exactly where the biceps tendon anchors into it.
Mechanisms of Injury
SLAP tears generally occur via two distinct mechanical pathways:
1. Acute Macrotrauma
Falling onto an outstretched hand (FOOSH) on an icy Toronto sidewalk, forcing the arm bone violently up into the socket.
A sudden, heavy, eccentric load, such as catching a falling heavy object, which violently yanks the biceps tendon, tearing its anchor off the bone.
2. The "Peel-Back" Mechanism (Overuse)
This is the most common cause for weightlifters and throwing athletes.
When you repeatedly bring your arm into maximum external rotation (like the cocking phase of a baseball pitch or holding a barbell behind your neck for a back squat), the biceps tendon twists.
This twisting motion creates a massive torsional force that literally "peels back" the superior labrum off the bone, causing micro-trauma that eventually becomes a full tear.
The Biomechanical Driver: Scapular Dyskinesis
Why do some athletes get SLAP tears while others don't? It comes down to the foundation: the shoulder blade (scapula).
If your shoulder blade is "slouched" forward due to poor posture or a weak serratus anterior, the socket is angled downward.
When you reach overhead, your arm bone hits a hard stop much earlier. To achieve the overhead position, you have to force the arm past its natural limit, radically increasing the strain and "peel-back" force on the labrum and biceps anchor.
Primary Source Proof: Conservative Management
Orthopedic and sports medicine literature increasingly mandates that conservative physiotherapy, focusing on scapular stabilization and posterior capsule flexibility, should be the first-line treatment for SLAP lesions, yielding excellent functional outcomes comparable to surgery.
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for upper extremity rehabilitation.
The Rehab Mechanics SLAP Protocol
Rehabilitating a SLAP tear requires absolute precision. We cannot use generic shoulder stretches, as overly stretching a torn labrum will make it worse. We must utilize targeted "remedial mechanics" to decompress the joint.
Phase 1: Protecting the Biceps Anchor (Weeks 1-4)
The immediate goal is to reduce the inflammatory sheer force pulling on the torn cartilage.
Biceps Unloading: We temporarily eliminate all heavy, isolated biceps loading (like curls) and extreme overhead reaching.
Posterior Capsule Mobilization: A tight posterior (back) shoulder capsule pushes the arm bone forward and upward, directly crushing the superior labrum. Our physiotherapists utilize heavy Grade III/IV manual joint glides to forcefully stretch the back of the capsule, restoring the ball to the dead-center of the socket.
Pectoral Release: Deep tissue mobilization to release the tight chest muscles that are pulling the shoulder blade out of alignment.
Phase 2: Dynamic Scapular Fortification (Weeks 4-8)
We must build an indestructible foundation for the arm to move upon.
Serratus Anterior and Lower Trap Activation: We utilize exercises like "scapular punches" and Y-raises. When these muscles are strong, they rotate the shoulder blade upward with your arm, ensuring the socket stays aligned with the humerus and completely eliminating the "peel-back" impingement force on the labrum.
Closed Kinetic Chain Stability: Planks, wall slides, and medicine ball walk-outs force the shoulder to stabilize the weight of the body, training the nervous system to lock the joint into a safe, centralized position.
Phase 3: Advanced Load and Kinetic Chain Transfer (Weeks 8-12+)
A strong shoulder is useless if it cannot handle the chaotic forces of sports.
Rotator Cuff Eccentrics: Rebuilding the resilience of the rotator cuff to absorb deceleration forces so the labrum doesn't have to.
Core-to-Arm Energy Transfer: The power for a heavy lift or a throw should come from the hips and core, not the fragile shoulder joint. We train explosive kinetic linking (like rotational medicine ball throws and heavy kettlebell swings) to ensure your lower body is generating the force, protecting the torn labrum from taking the brunt of the load.
Stop Fearing the Tear
An MRI showing a SLAP tear is not a death sentence for your active lifestyle. By meticulously correcting your shoulder mechanics, you can eliminate the destructive friction and return to lifting, throwing, and living pain-free.
Book a specialized sports orthopedic assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite upper extremity rehabilitation in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does Sharp Pain in the Front of the Shoulder Mean I Tore My Bicep Tendon?
No. Sharp front shoulder pain is most commonly proximal biceps tendinopathy or impingement, not a full tear. Physiotherapy completely resolves this by correcting scapular mechanics, releasing the pectoral fascia, and applying eccentric loading to the biceps tendon to rebuild its structural integrity without surgery.
The Weightlifter's Worst Nightmare
For the dedicated strength athletes, CrossFitters, and recreational tennis players living in Queen West and Liberty Village, shoulder health is paramount. One of the most terrifying, yet incredibly common, injuries in these demographics is a sudden, sharp, burning pain located precisely at the very front of the shoulder joint, radiating slightly down the arm.
The immediate reaction is panic. Patients feel the pain directly over their bicep muscle and instantly assume they have suffered a massive, catastrophic tear of the biceps tendon that will require surgical reattachment. They stop lifting, cancel their tennis matches, and put their arm in a sling.

However, full ruptures of the biceps tendon are quite rare and usually present with a highly visible, deformed "Popeye" muscle bulge. In the vast majority of cases seen at Rehab Mechanics, this sharp, localized pain is Proximal Biceps Tendinopathy. It is an overuse injury caused by faulty shoulder mechanics that are grinding the tendon against the bone. By correcting how your shoulder blade and rotator cuff function, advanced physical therapy can eliminate the friction and permanently heal the tendon.
Structural Analysis: The Mechanics of the Biceps Tendon

To understand how to fix anterior shoulder pain, we must perform a detailed biomechanical analysis of the shoulder joint and the complex route the biceps tendon takes to get there.
The Anatomy of the Long Head of the Biceps (LHB)
Your biceps muscle has two upper attachment points (heads) that connect it to the shoulder. The "short head" attaches safely outside the joint. The "long head" is the troublemaker.
The Bicipital Groove: The Long Head of the Biceps (LHB) tendon must travel up the front of your arm bone (humerus) through a very narrow, bony trench called the bicipital groove.
The Transverse Humeral Ligament: A tight band of tissue straps the tendon down into this groove to keep it from popping out when you move.
The Intra-Articular Journey: Once it passes through the groove, the tendon literally dives inside the shoulder joint capsule to attach to the top of the socket (the labrum).
The Pathology of Friction (Tendinosis)
Because the LHB tendon makes a sharp 90-degree turn over the bone to enter the joint, it is highly susceptible to friction.
The "Victim" of Poor Mechanics
The biceps tendon rarely fails on its own; it fails because the rest of the shoulder stops doing its job.
Rotator Cuff Exhaustion: If your rotator cuff is weak, it cannot hold the ball of the shoulder tightly in the socket. The joint becomes wobbly.
The Biceps Overcompensation: The brain panics and recruits the LHB tendon to act as a secondary stabilizer. The biceps tendon is forced to pull double-duty, clamping down violently to stabilize the shoulder during a heavy bench press or overhead serve.
The Degeneration Cycle
Friction and Shearing: This constant overworking causes the tendon to grind aggressively back and forth within the narrow bicipital groove.
Angiofibroblastic Degeneration: The friction causes microscopic tears. The tendon thickens, swells, and becomes engorged with chaotic scar tissue and sensitive nerve endings. This is tendinosis—a state of cellular decay, not just simple inflammation.
Primary Source Proof: Biceps Tendinopathy Rehabilitation
Orthopedic sports medicine literature confirms that targeted conservative management—focusing on scapular retraining and eccentric tendon loading—is the highly effective gold standard for resolving proximal biceps tendinopathy, rendering surgical tenodesis unnecessary for most patients.
Review the Clinical Evidence on PubMed: Management of Proximal Biceps Tendinopathy (National Library of Medicine)
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for upper extremity rehabilitation.
The Rehab Mechanics Corrective Protocol
Treating biceps tendinopathy requires a comprehensive mechanical overhaul of the entire shoulder complex. We do not just massage the front of the arm; we fix the foundation.
Phase 1: Unloading and Pain Modulation (Weeks 1-3)
We must immediately stop the mechanical grinding to let the swollen tendon breathe.
Pectoral and Anterior Deltoid Release: Utilizing advanced manual therapy to strip the tight muscles on the front of the chest. If the shoulders are pulled forward into an internal rotation, the bicipital groove narrows drastically, crushing the tendon.
Activity Modification: Temporarily replacing heavy barbell pressing and overhead throwing with pain-free, neutral-grip exercises to maintain fitness without provoking the tendon.
Joint Mobilization: Our physiotherapists apply gentle posterior glides to the glenohumeral joint to reposition the ball centrally in the socket, taking the mechanical strain off the front of the shoulder.
Phase 2: Scapular and Rotator Cuff Reset (Weeks 4-6)
We must rebuild the primary stabilizers so the biceps tendon can stop overworking.
Lower Trapezius and Serratus Activation: Rebuilding the muscles that anchor the shoulder blade (scapula) to the ribcage. A stable shoulder blade provides a safe, wide clearance for the biceps tendon to move.
Posterior Cuff Fortification: Utilizing targeted resistance band drills to strengthen the infraspinatus and teres minor, forcing the rotator cuff to resume its job of holding the joint stable.
Phase 3: Eccentric Loading and Tendon Remodeling (Weeks 6+)
Once the mechanics are fixed, we must physically rebuild the degenerated biceps tendon.
Heavy Slow Eccentrics: Tendons heal by laying down new collagen under heavy, lengthening tension. We utilize exercises like slow, heavy dumbbell curls, focusing entirely on the 4-second lowering phase. This physically forces the chaotic scar tissue fibers to align perfectly, thickening and bulletproofing the tendon against future tears.
Kinetic Chain Integration: Ensuring that power from the hips and core transfers seamlessly through the shoulder during athletic movements, preventing the arm from absorbing isolated shock.
Stop Fearing a Tear
Do not let sharp, anterior shoulder pain convince you that your lifting or athletic career is over. By addressing the deep mechanical faults in your shoulder and progressively loading the tissue, physical therapy can reverse the tendon degeneration and restore your power.
Book a comprehensive upper extremity assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports recovery in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Fix a 'Neck Hump' and Reverse Severe Forward Head Posture?
Yes. Physiotherapy can significantly reduce or eliminate a "neck hump" by correcting severe cervicothoracic muscle imbalances. Through targeted deep neck flexor strengthening and upper thoracic mobilization, physical therapy reverses the structural adaptations of chronic forward head posture, preventing permanent spinal deformity.
The Physical Toll of the Screen-Bound Lifestyle
In the high-tech, screen-dominated hubs of Queen West and Liberty Village, the human spine is under relentless attack. Spend five minutes in a local coffee shop and you will observe a sea of professionals hunched deeply over laptops and smartphones.
Beyond the immediate neck pain and tension headaches, many individuals begin to notice an alarming physical change: a visible, hard, fleshy bump forming at the exact base of their neck. Colloquially referred to as a "neck hump" or "Dowager’s hump," this structural deformity is a source of immense physical discomfort and deep cosmetic anxiety.
Patients frequently panic, assuming they have developed a spinal tumor or a permanent, unfixable arthritic deformity. While severe, age-related osteoporosis can cause irreversible wedging of the vertebrae, the vast majority of "neck humps" in young and middle-aged urban professionals are entirely functional and biomechanically reversible. At Rehab Mechanics, we specialize in aggressive postural correction to dismantle this structural adaptation and restore your natural spinal alignment.
Structural Analysis: The Mechanics of the Cervicothoracic Junction

To effectively eliminate a neck hump, we must perform a detailed biomechanical analysis of the lower neck and upper back, a region known as the cervicothoracic junction (CTJ).
The Anatomy of the Intersection
The CTJ is the exact point where your highly mobile, lordotic cervical spine (the neck) meets your rigid, kyphotic thoracic spine (the upper back). Specifically, this occurs at the C7 and T1 vertebrae.
The Spinous Processes: The C7 vertebra naturally has a long, bony projection pointing backward (the spinous process). Even in a healthy spine, this is the bump you can feel at the base of your neck.

The Biomechanical Collapse (Tech Neck)
The human head weighs approximately 10 to 12 pounds. When you stare down at a screen, your head shifts forward out of its neutral center of gravity.
The Leverage Crisis
For every inch your head translates forward, the functional load on the muscles at the base of your neck doubles.
The Muscular Exhaustion: The muscles of the upper back (trapezius, levator scapulae) must contract continuously with massive force just to keep your head from falling onto your chest.
The "Hinge" Effect: Because the head is stuck forward, you must violently hinge your upper neck backward just to look straight ahead at your monitor. This traps the lower neck in deep flexion and the upper neck in extreme extension.
Why the "Hump" Forms
The neck hump is a brilliant, albeit ugly, biological defense mechanism.
Fibro-Fatty Thickening
Because the C7 and T1 vertebrae are being constantly pulled and subjected to massive shearing forces, the body panics. It attempts to "cast" and protect the vulnerable bone.
The body rapidly deposits a thick pad of fibro-fatty tissue directly over the prominent spinous processes.
Simultaneously, the deep fascial layers glue themselves down into dense scar tissue to prevent the spine from snapping.
The result is a hard, visible, painful lump of fat, fascia, and swollen muscle.
Primary Source Proof: Postural Rehabilitation
Clinical biomechanical research explicitly proves that targeted exercise programs designed to correct forward head posture effectively reduce muscular spasticity, realign the cervicothoracic junction, and visibly improve spinal alignment.
Review the Clinical Evidence on PubMed: Effect of an Exercise Program for Posture Correction on Muscle Spasticity and Postural Alignment
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for postural rehabilitation.
The Rehab Mechanics Postural Correction Protocol
You cannot fix a neck hump by simply "trying to sit up straight" or wearing a gimmicky posture brace from the internet. You must actively break down the fibrotic tissue and rebuild the neurological endurance of your spine.
Phase 1: Fibrotic Tissue Breakdown and Joint Unlocking
We must physically melt away the dense, protective padding.
Deep Myofascial Release: Our physiotherapists apply aggressive, targeted manual pressure and instrument-assisted soft tissue mobilization (IASTM) directly over the C7/T1 junction to break down the dense, fibro-fatty fascial adhesions.
Thoracic Spine Mobilization: If the mid-back is locked in a hunch, the neck can never sit straight. We utilize high-grade joint manipulations to forcefully restore thoracic extension (the ability to arch backward).
Pectoral Release: Lengthening the tight chest muscles that are physically dragging the shoulders forward and fueling the collapse.
Phase 2: Neuromuscular Re-Education
Once the joints are free, we must wake up the muscles that have been asleep for years.
Deep Cervical Flexor (DCF) Activation: The tiny muscles in the front of your throat are entirely dormant. We use specific biofeedback drills (like micro-chin tucks) to reactivate these stabilizers. When the DCF fires, it automatically pulls the head back over the shoulders.
Lower Trapezius Fortification: Teaching the brain to fire the muscles at the bottom of the shoulder blades, ensuring the upper back is anchored firmly downward.
Phase 3: High-Load Postural Endurance
Posture is about biological endurance. You must be strong enough to hold the correction for a 10-hour workday.
Isometric Holds: Implementing heavy farmer's carries and prone positional holds to build massive endurance in the erector spinae.
Ergonomic Integration: We assess and correct your exact desk setup, monitor height, and chair support to guarantee your workspace supports your newly restored spinal mechanics rather than destroying them.
Stand Tall and Eliminate the Hump
Do not accept a permanent structural deformity as the inevitable cost of your career. By overhauling your body mechanics and reversing the forces of forward head posture, you can eliminate the neck hump and restore a healthy, pain-free spine.
Book a comprehensive postural and biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Stop the Painful Snapping in My Hip?
Yes. Physiotherapy cures snapping hip syndrome by releasing the hypertonic psoas or IT band and rebuilding deep pelvic stabilizers. This biomechanical approach stops the tendon from violently snapping across the pelvic bone, eliminating sharp groin or lateral hip pain without surgical intervention.
The Agony of the Clicking Joint
For the active residents of Queen West, Liberty Village, and Trinity Bellwoods, staying in motion is a way of life. From local run clubs and intensive Pilates classes to recreational martial arts and dance, the hips endure an immense amount of repetitive mechanical stress.
However, many active Torontonians develop a deeply frustrating and frightening condition: a loud, audible, and painful "snap," "click," or "clunk" deep within their hip joint every time they lift their leg, run, or climb stairs.
Often dismissed by standard walk-in clinics as "just tight muscles" or incorrectly diagnosed as early arthritis, this condition is clinically known as Coxa Saltans, or Snapping Hip Syndrome. When the snapping becomes painful, it signifies a massive biomechanical friction issue that will eventually destroy the surrounding bursa and tendons if ignored.
At Rehab Mechanics, located inside the Prime Medical Centre, we specialize in advanced orthopedic problem-solving. We understand that a snapping hip is a symptom of a misaligned pelvis and imbalanced muscular tension. Through targeted "human mechanics" physical therapy, we can physically alter the tracking of your tendons, permanently silencing the snap.
Structural Analysis: The Mechanics of Coxa Saltans
To understand how to fix a snapping hip, we must perform a detailed biomechanical analysis of the pelvic girdle and identify exactly what is snapping over where. Snapping Hip Syndrome generally falls into two primary structural categories.
1. Internal Snapping Hip (The Psoas Snap)
This is the most common variation, presenting as a deep, painful "clunk" in the front of the groin when lowering the leg from a lifted position (like descending from a high step or during flutter kicks in Pilates).

The Culprit: The Iliopsoas tendon (your primary, deepest hip flexor).
The Bony Prominence: The iliopectineal eminence ( a bony ridge on the front of the pelvis) or the head of the femur.
The Friction Mechanism
When you sit at a desk for eight hours a day, the massive psoas muscle adaptively shortens and becomes rigidly tight.
As you lift your knee, the tight tendon slides off the bony ridge.
When you lower your leg, the tension skyrockets, and the tendon snaps violently back over the bone like a thick, highly tensioned rubber band.
The Collateral Damage: This violent snapping eventually crushes the iliopsoas bursa (the fluid-filled sac sitting underneath the tendon), leading to severe, chronic groin inflammation (bursitis).
2. External Snapping Hip (The IT Band Snap)
This variation presents as a sharp, visible snapping sensation on the outside of the hip, often feeling as though the hip is momentarily "popping out of its socket."
The Culprit: The Iliotibial (IT) Band or the anterior gluteus maximus tendon.
The Bony Prominence: The Greater Trochanter (the large, bony bump on the outside of your upper thigh).
The Gluteal Weakness Trigger
External snapping is rarely a problem with the IT band itself; it is a problem with the pelvic stabilizers.
The Pelvic Drop
If your gluteus medius is weak, your pelvis drops laterally when you walk or run.
This pelvic drop dramatically alters the angle of the IT band, pulling it violently tight.
As you swing your leg forward and back, the tightened fascia violently snaps back and forth over the greater trochanter, eventually causing highly painful trochanteric bursitis.
Primary Source Proof: Non-Operative Hip Kinematics
Advanced orthopedic and sports medicine literature overwhelmingly supports non-operative, biomechanical rehabilitation—focusing on tendon lengthening and lumbo-pelvic stabilization—as the definitive first-line cure for Coxa Saltans.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for hip rehabilitation.
The Rehab Mechanics Corrective Protocol
Treating a snapping hip requires absolute precision. Generic hip stretches often exacerbate the snapping. We must utilize a highly controlled, phased approach to restore perfect joint tracking.
Phase 1: Tendon Desensitization and Soft Tissue Release
Before we can rebuild the hip, we must release the structural brakes that are causing the friction.
Advanced Myofascial Release: Our physiotherapists use targeted, deep ischemic compression to release the hypertonic psoas major or the Tensor Fasciae Latae (TFL). By manually lengthening the muscle belly, we instantly reduce the tension on the snapping tendon.
Joint Mobilization: Unlocking the hip capsule itself. If the ball-and-socket joint is stiff, the femur glides forward, pushing the bony ridges directly into the tight tendons. Manual glides restore centralization.
Activity Modification: We temporarily eliminate the specific athletic movements that trigger the snap, allowing the severely crushed bursa to chemically calm down.
Phase 2: Lumbo-Pelvic Neuromuscular Re-Education
We must correct the pelvic alignment to permanently alter the tracking angle of the tendons.
Pelvic Tilt Correction: If you have an anterior pelvic tilt, the psoas is under constant stretch. We train the deep core (transversus abdominis) to pull the pelvis backward into a neutral alignment, providing massive mechanical relief to the front of the hip.
Eccentric Psoas Loading: Standard stretching is insufficient. We use specialized eccentric exercises (slowly lowering the leg against resistance) to remodel the psoas tendon, making it thicker, stronger, and more elastic so it no longer snaps over the bone.
Phase 3: Gluteal Fortification and Dynamic Control
We must build a muscular brace that stops the pelvis from dropping during walking and running.
Isolated Glute Medius Activation: Utilizing side-lying hip abductions, clamshells, and isometric holds to wake up the lateral stabilizers.
Functional Integration: Progressing to single-leg deadlifts, split squats, and dynamic step-ups. We monitor your mechanics closely to ensure your femur stays perfectly aligned, proving to your nervous system that it can handle high-load activities without the painful snapping.
Silence Your Hip Pain Permanently
You do not have to live with the fear of your hip "popping out" or the chronic, burning pain of bursitis. By analyzing and correcting your pelvic mechanics, physical therapy offers a permanent, non-surgical solution.
Book a comprehensive biomechanical hip assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports and orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does Sitting All Day Cause Gluteal Amnesia and Lower Back Pain?
Yes. Prolonged sitting causes gluteal amnesia by neurologically inhibiting the gluteal muscles. Physiotherapy reverses this neuromuscular shutdown through targeted activation drills, deep tissue release of the hip flexors, and heavy resistance training, permanently resolving the resulting lower back and knee pain.
The Postural Epidemic of the Modern Workspace
Toronto is a city driven by knowledge workers, tech innovators, and corporate professionals. While the skyline is constantly growing, the physical reality for most of these workers involves sitting immobilized in an ergonomic chair for 40 to 60 hours a week.
Over the past few years, a highly specific and alarming pattern has emerged at Rehab Mechanics. Patients arrive at our Queen West clinic complaining of chronic, nagging lower back pain, tight hamstrings, and aching knees. They stretch daily, they get massages, yet the pain always returns.
When we perform a biomechanical audit, we discover a phenomenon colloquially known as "Dead Butt Syndrome," or clinically termed Gluteal Amnesia. Because of the massive amount of time spent sitting, their brains have literally "forgotten" how to fire their glute muscles. When the largest, most powerful muscle group in the human body shuts down, catastrophic mechanical failure occurs up and down the entire kinetic chain.
Structural Analysis: The Mechanics of Gluteal Amnesia
To understand how sitting ruins your back and knees, we must perform a detailed neurological and biomechanical analysis of the hip joint.
The Phenomenon of Reciprocal Inhibition
The human nervous system operates on a principle of efficiency known as reciprocal inhibition. When a muscle on one side of a joint contracts, the brain automatically sends an inhibitory signal to the muscle on the opposite side, telling it to relax so movement can occur.
The Sitting Trap: When you sit at a desk, your hip flexors (psoas and iliacus) are placed in a shortened, contracted position for hours on end.
The Neurological Shutdown: Because the hip flexors are constantly "on," the brain sends a continuous, non-stop inhibitory signal to the opposing muscles—your gluteus maximus.
The Result: The glutes are chemically and neurologically switched "off." Over time, the neural pathways weaken, and the muscle suffers profound atrophy. You develop Gluteal Amnesia.
The Kinetic Chain Breakdown
Your glutes are the foundational engine of your body. When they go offline, the nervous system panics and recruits other, smaller muscles to do their job. This compensatory overload destroys your joints.
Lumbar Spine Overload (Lower Back Pain)
When you bend over to pick up a box or try to perform a deadlift, your glutes are supposed to drive you back up to a standing position.
The Compensation: If the glutes are amnesic, the brain forces your lower back muscles (erector spinae) and hamstrings to take 100% of the load.
The Failure: These muscles are not designed to be primary movers. They rapidly overwork, spasm, and place massive shearing forces on your lumbar spinal discs, leading to chronic back pain and eventual disc herniation.
Knee Valgus Collapse (Knee Pain)
Your gluteus medius (the side of your hip) is responsible for keeping your femur (thigh bone) straight.
The Compensation: When the glute medius shuts down, there is nothing stopping your thigh bone from rotating inward.
The Failure: Every time you take a step, your knee caves inward toward your midline (valgus collapse). This violently grinds the kneecap against the femur, causing severe anterior knee pain (Runner’s Knee) and destroying the meniscus.
Primary Source Proof: Neuromuscular Re-Education
Clinical orthopedic research explicitly proves that resolving non-specific lower back pain and lower extremity injuries requires direct neuromuscular reactivation and strengthening of the gluteal complex to reverse postural inhibition.
Download Clinical Efficacy PDF: The Efficacy of Gluteal Neuromuscular Re-Education in the Treatment of Chronic Lumbar and Patellofemoral Pain (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for biomechanical rehabilitation.
The Rehab Mechanics Corrective Protocol

Treating gluteal amnesia requires a precise "re-wiring" of the nervous system. You cannot simply go to the gym and do heavy squats; if your glutes are asleep, your lower back will just take the weight, making the injury worse.
Phase 1: Releasing the Brakes (Hip Flexor Deactivation)
We must stop the continuous inhibitory signal before we can wake the glutes up.
Deep Myofascial Psoas Release: Our physiotherapists utilize advanced, highly targeted manual therapy deep into the abdomen to physically lengthen the rigidly tight hip flexors.
Active Release Techniques (ART): Stripping the tight rectus femoris and TFL (front of the thigh) to ensure the pelvis can return to a neutral, upright alignment.

Phase 2: Neuromuscular Isolation (Waking the Dead)
We use micro-movements to force the brain to re-establish a neurological connection with the glute fibers.
Prone Glute Squeezes: Using tactile feedback (physically tapping the muscle) to help the patient consciously contract the gluteus maximus without firing the hamstrings.
Clamshells and Hydrants: Isolating the gluteus medius in side-lying positions, ensuring the pelvis remains completely still so the lower back cannot "cheat" the movement.
Phase 3: Dynamic Integration and Heavy Loading
Once the brain remembers how to use the glutes, we must rebuild their absolute strength to handle the real world.
Glute Bridging and Hip Thrusts: Progressing to heavily loaded hip extension exercises that target the glutes while the spine remains safely supported.
Functional Movement Correction: Re-teaching you how to squat, lunge, and run using a "hip hinge" pattern. We monitor your knees closely to ensure the newly awakened glutes fire automatically to prevent knee valgus.
Restart Your Engine
Do not let an office chair slowly destroy the biomechanics of your lower body. By aggressively treating gluteal amnesia, you can eliminate the compensatory forces that cause chronic back and knee pain.
Book a comprehensive biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Prevent Hip Replacement Surgery for Severe Osteoarthritis?
Yes. Physiotherapy routinely delays or prevents hip replacement surgery for osteoarthritis by strengthening the deep gluteal stabilizers. Restoring joint capsule mobility and muscular support drastically reduces bone-on-bone friction, managing chronic inflammation and returning patients to pain-free urban mobility without surgery.
The Fear of "Bone on Bone" Degeneration
For active residents in Toronto—whether you spend your weekends walking through Trinity Bellwoods, cycling along the waterfront, or simply commuting daily through Queen West—few things are as terrifying as the onset of deep, grinding hip pain.
When a patient visits a walk-in clinic and receives an X-ray showing "mild to moderate hip osteoarthritis," the conversation often immediately turns to surgical waitlists. The phrase "bone on bone" is used frequently, creating immense psychological fear. Patients assume their hip is completely destroyed, leading them to stop walking, stop exercising, and isolate themselves on the couch to "save" whatever cartilage they have left.
This "wait and deteriorate" mindset is the absolute worst thing you can do for an arthritic joint. At Rehab Mechanics, we heavily advocate for conservative orthopedic management. Your X-ray does not dictate your pain. By overhauling your body mechanics, we can train your muscles to absorb the impact of walking before it ever reaches your degenerated hip joint, successfully avoiding the operating room.
Structural Analysis: The Mechanics of Hip Osteoarthritis
To understand how to save a failing hip, we must perform a biomechanical analysis of the joint’s architecture and the reality of cartilage degradation.
The Anatomy of the Ball and Socket
Your hip (the acetabulofemoral joint) is a massive weight-bearing structure.
The Articular Cartilage: Both the head of the femur (the ball) and the acetabulum (the socket) are coated in a thick, slippery layer of articular cartilage. This cartilage acts like a Teflon coating, allowing the bones to glide with zero friction.
The Labrum and Synovium: A rubbery gasket (the labrum) seals the joint, and the synovial membrane produces a thick, egg-white-like fluid that constantly lubricates the cartilage.
The Pathology of Joint Decay (Osteoarthritis)
Osteoarthritis (OA) is not just mechanical wear and tear; it is a complex, active biological disease process.
The Cartilage Thinning Phase
Over decades of use, or secondary to old sports injuries, the water content within the articular cartilage decreases. The Teflon coating begins to fray, thin out, and eventually expose the underlying subchondral bone.
The Inflammatory Cascade
As the cartilage shreds, the debris floats inside the joint capsule.
Synovitis: The joint lining reacts to this debris by becoming violently inflamed, causing the hip to swell and ache deeply into the groin.
Osteophyte Formation: The body attempts to stabilize the wobbly, failing joint by growing new bone around the edges. These jagged bone spurs (osteophytes) physically block your range of motion, making it impossible to put on your socks or get out of a low car seat.
The Biomechanical Failure: Why the Pain Spikes
If the cartilage loss is the disease, why does the pain suddenly become unbearable? The answer lies in the muscles.
The Gluteal Shutdown
When your hip is inflamed, your brain initiates a protective reflex called Arthrogenic Muscle Inhibition. It literally shuts off the electrical signal to your gluteus medius and gluteus maximus to stop you from walking on the injured leg.
The Mechanical Crushing
Because your glutes are shut down and atrophied, they can no longer absorb the shock of your body weight. Now, every time your foot strikes the Toronto pavement, 100% of the kinetic impact bypasses the weak muscles and slams directly into the exposed, arthritic bone. This is why the pain becomes agonizing.
Primary Source Proof: Non-Operative Efficacy
Major international orthopedic guidelines and extensive peer-reviewed literature strongly mandate that comprehensive, supervised physiotherapy must be exhausted before total hip arthroplasty (surgery) is considered.
Note: The link above directs to external, peer-reviewed medical literature demonstrating our commitment to evidence-based practice and international clinical guidelines for orthopedic rehabilitation.
The Rehab Mechanics Joint Preservation Protocol
At our clinic inside the Prime Medical Centre, we do not view osteoarthritis as a surgical inevitability. We utilize an aggressive, phased biomechanical approach to build a muscular exoskeleton around your failing joint.
Phase 1: Joint Distraction and Pain Modulation (Weeks 1-4)
Before we can build strength, we must lower the severe pain threshold.
Medical Integration: We work directly with the physicians at Prime Medical Centre who may administer targeted, intra-articular anti-inflammatory injections to instantly clear the synovitis.
Manual Joint Traction: Our physiotherapists apply heavy, sustained pulling forces (distraction) to the leg. This physically separates the ball from the socket, creating a vacuum effect that pulls fresh, lubricating synovial fluid into the starving cartilage.
Capsular Stretching: Aggressively stretching the tight, fibrotic joint capsule to restore your ability to extend the hip behind you, which is critical for normal walking.
Phase 2: Isometric and Closed-Chain Loading (Weeks 4-8)
We must wake up the shut-down gluteal muscles without creating painful bone-on-bone friction.
High-Intensity Isometrics: You will push your leg maximally against an immovable resistance. The muscles fire at 100% capacity, but the joint does not bend, allowing you to build massive strength without grinding the cartilage.
Closed-Chain Activation: Utilizing targeted leg presses and wall sits to teach the nervous system to absorb body weight safely through the musculature rather than the bone.
Phase 3: Gait Retraining and Proprioception (Weeks 8-12+)
Once the muscular "brace" is built, we must ensure it works automatically when you navigate the city.
Trendelenburg Correction: We use mirror feedback and targeted cues to ensure your pelvis does not drop when you stand on the arthritic leg, eliminating the painful limping pattern.
Dynamic Shock Absorption: Training your core and hip to work synergistically during step-downs and uneven surface walking, proving to your nervous system that you are strong, capable, and no longer reliant on the damaged cartilage.
Stop the Deterioration
Do not let an X-ray dictate the rest of your active life. By correcting your structural biomechanics, you can offload the damaged joint, eliminate the chronic inflammation, and successfully keep your natural hip.
Book a comprehensive orthopedic assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced joint preservation in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
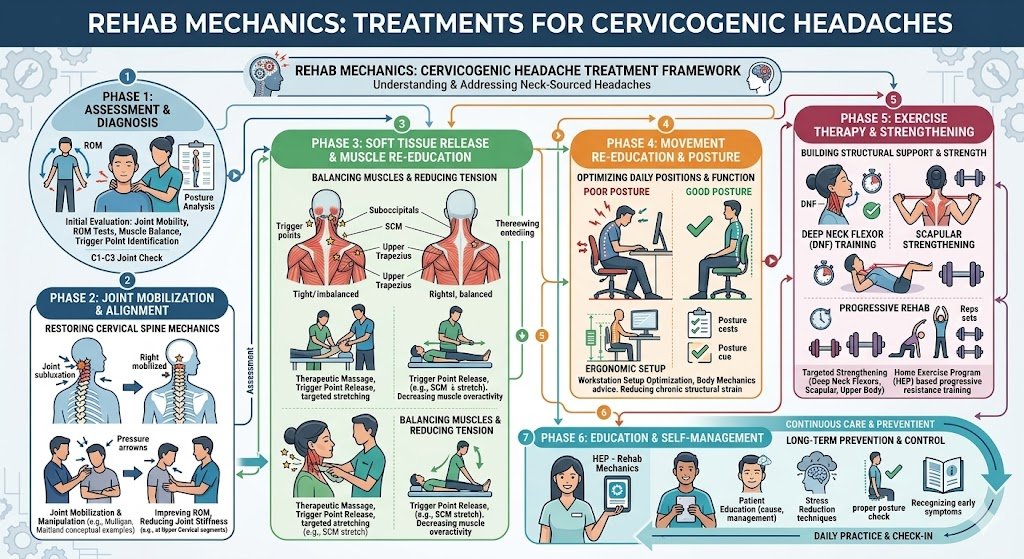
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Cure Chronic Tension Headaches from Desk Work?
Yes. Physiotherapy permanently cures tension headaches by fixing the cervical biomechanics causing them. By mobilizing stiff upper neck joints, releasing suboccipital muscle spasms, and strengthening deep neck flexors, physical therapy eliminates the structural nerve irritation that triggers chronic daily headaches.
The Headache Epidemic in Queen West
In the digital age, our lives are dictated by screens. Whether you are coding a new app in Liberty Village, analyzing spreadsheets in the Financial District, or constantly checking a smartphone, your head is perpetually tilted forward.
The physical toll of this lifestyle is catastrophic for the cervical spine, giving rise to an epidemic of chronic, agonizing head pain. Countless Toronto professionals wake up daily with a dull, vice-like pressure wrapping around their temples, an aching tightness at the base of the skull, or sharp pain radiating behind their eyes.
Often dismissed by walk-in clinics as "just stress" and treated with endless cycles of Advil or Tylenol, these are clinically classified as Cervicogenic or Tension-Type Headaches. When you search for "remedial mechanics" or "Queen Street physiotherapy" to resolve this pain, you are on the right track. At Rehab Mechanics, we know that these headaches are not a chemical imbalance in your brain; they are a direct, mechanical consequence of a failing neck structure. Fixing the spine permanently turns off the headache alarm.

Structural Analysis: The Biomechanics of a Tension Headache
To understand why stretching your neck doesn't cure a severe tension headache, we must dive deep into the neurology and biomechanics of the upper cervical spine.
The Weight of the "Tech Neck"
The human head weighs between 10 and 12 pounds. It is designed to balance perfectly on top of the cervical spine, requiring minimal muscular effort to stay upright.
The Leverage Crisis: For every inch your head translates forward to look at a monitor, the mechanical load on the muscles at the back of your neck doubles.
The Muscular Exhaustion: A severe "Tech Neck" forces the tiny muscles at the base of the skull (the suboccipitals) to hold back 30 to 40 pounds of force for 10 hours a day.
The Spasm: These muscles rapidly fatigue, lose their blood supply (ischemia), and lock into permanent, rock-hard spasms.
The Neurological Bridge (Why Your Head Hurts)
How does a knot in your neck cause pain behind your eye? The answer lies in the complex wiring of the central nervous system.
The Trigeminal-Cervical Nucleus (TCN)
The nerves that supply feeling to the upper three joints of your neck (C1, C2, and C3) merge into a massive relay station in your brainstem called the Trigeminal-Cervical Nucleus.
Crucially, the Trigeminal Nerve—which supplies sensation to your forehead, temples, and face—also plugs into this exact same relay station.
The Crossed Signal: When the joints in your upper neck are jammed and the suboccipital muscles are violently spasming, they flood the relay station with pain signals. The brain gets confused by the sheer volume of data and misinterprets the origin of the pain, projecting it forward into the head and face (Referred Pain).
The Myodural Bridge
Recent anatomical discoveries have revealed that a small band of connective tissue directly links the suboccipital muscles in the neck to the dura mater (the pain-sensitive outer covering of the brain).
When the neck muscles are in severe spasm, they literally tug on the lining of your brain, generating the sensation of a vice crushing your skull.
Primary Source Proof: Cervicogenic Decompression
Neurological and orthopedic literature unequivocally demonstrates that specific cervical spine mobilization and deep neck flexor rehabilitation are vastly superior to pharmacological management for the long-term cure of cervicogenic and tension headaches.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for cervical rehabilitation.
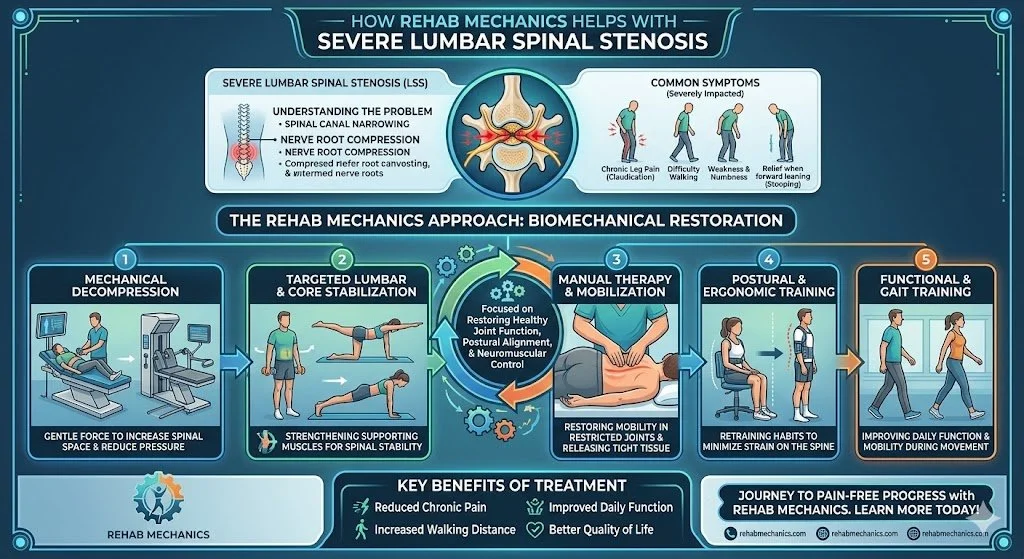
The Rehab Mechanics Headache Eradication Protocol
We do not just massage the sore muscles. Treating cervicogenic headaches requires a profound overhaul of your upper body mechanics to stop the muscles from spasming in the first place.
Phase 1: Decompressing the Neurological Bottleneck
Our first goal is to immediately cut off the pain signals flooding the brainstem.
Upper Cervical Mobilization: Our physiotherapists use precise, gentle Grade II and Grade III manual glides to un-jam the C1, C2, and C3 vertebrae. Restoring the micro-movement of these joints instantly reduces the nerve irritation causing the referred pain.
Suboccipital Ischemic Compression: We apply deep, sustained pressure directly into the base of the skull. This manually breaks the spasm in the suboccipitals, releasing the tension on the "myodural bridge" and draining the pressure from the head.
Phase 2: Restoring the Foundation (Thoracic Extension)
The neck cannot sit straight if the mid-back is hunched over.
Thoracic Spine Unlocking: Utilizing high-level joint mobilizations and foam-roller drills to aggressively restore extension in the upper back.
Pectoral Myofascial Release: Lengthening the tight chest muscles that are physically dragging the shoulders forward and fueling the poor posture.
Phase 3: Rebuilding the Deep Stabilizers
This phase ensures the headaches never return. We must build biological endurance.
Deep Cervical Flexor (DCF) Training: We utilize specific micro-movements (like chin tucks with a pressure biofeedback unit) to re-awaken the dormant muscles in the front of your throat. When these muscles fire properly, they automatically pull the head back over the shoulders, instantly taking the load off the back of the neck.
Postural Ergonomics: We review your exact desk setup, monitor height, and chair support to guarantee your Toronto workspace supports, rather than destroys, your newly restored spinal mechanics.
Turn Off the Headache Alarm
You do not have to accept daily tension headaches or rely on a permanent supply of painkillers. By diagnosing and correcting the mechanical failures in your cervical spine, you can permanently eradicate the pain.
Book a comprehensive neurological and biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does Stretching Make High Hamstring Pain and "Yoga Butt" Worse?
Yes. Aggressively stretching a high hamstring tendinopathy severely worsens the injury. The pain at your sit bone is caused by compressive friction, not muscle tightness. Physiotherapy resolves this by halting deep stretches and utilizing heavy, progressive isometric and eccentric loading to rebuild the tendon.
The Agony at the Sit Bone
Queen West and Trinity Bellwoods are vibrant epicenters for Toronto's yoga, Pilates, and active running communities. While these practices are fantastic for flexibility and cardiovascular health, they frequently lead to a highly specific, deeply frustrating overuse injury.
Patients often present at Rehab Mechanics complaining of a literal "pain in the butt." It is a deep, localized, burning ache right on the sit bone (the bony prominence you feel when sitting on a hard chair). This pain spikes aggressively when bending over to touch the toes, performing a downward dog, or sprinting uphill.
In the yoga community, this is colloquially known as "Yoga Butt." Medically, it is Proximal Hamstring Tendinopathy (PHT).
The natural, intuitive response to a tight, aching hamstring is to stretch it aggressively. Patients will spend hours forcing themselves into deep forward folds, hoping the muscle will "release." However, when dealing with PHT, stretching is the absolute worst mechanical input you can provide. To cure this stubborn tendinopathy, you must understand the biomechanics of tendon compression and stop treating the injury like a simple muscle cramp.
Structural Analysis: The Mechanics of Hamstring Compression
To successfully rehabilitate Proximal Hamstring Tendinopathy, we must perform a detailed structural analysis of the pelvic anatomy and how the hamstring tendon behaves under load.
The Ischial Tuberosity Anchor
Your hamstring is not a single muscle; it is a group of three large muscles running down the back of your thigh.
The Common Origin: All three of these massive muscles merge into a single, thick tendon at the top of your leg.
The Bony Anchor: This common tendon anchors directly into the ischial tuberosity—the thick, bony projection at the absolute base of your pelvis (your sit bone).
The Pathology of Compressive Tendinosis
Tendons are incredibly strong when pulled straight (tensile load). However, they are highly vulnerable to being compressed or wrapped around a bone.
The "Wrap-Around" Effect (Why Stretching Hurts)
When you bend forward at the waist with straight legs (like a yoga forward fold or a deadlift), your pelvis rotates forward.
The Friction Point: As the pelvis rotates, the hamstring tendon is physically dragged and wrapped tightly around the bony edge of the ischial tuberosity, much like a rope pulled tightly around a rock.
The Ischemic Crush: This violent mechanical compression squeezes the blood flow out of the tendon at the exact point it connects to the bone.
Cellular Degeneration: If you do this repetitively (e.g., hundreds of deep yoga stretches or running uphill), the tendon cells fail. They stop producing healthy Type I collagen and begin to degenerate into a chaotic, painful, and thickened mass of scar tissue.
This is why stretching feels good for about 10 minutes (as it temporarily numbs the nerve endings) but makes the structural degeneration significantly worse the next day. You are actively crushing an injured tendon.
Primary Source Proof: Tendon Rehabilitation
Orthopedic sports medicine literature is categorical: passive stretching and total rest fail to resolve proximal hamstring tendinopathy. Progressive, heavy mechanical loading is the internationally recognized gold standard for tendon regeneration.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for tendinopathy rehabilitation.
The Rehab Mechanics Corrective Protocol
At our Prime Medical Centre clinic, our protocol for PHT completely removes compressive stretching and replaces it with advanced, progressive tissue loading to rebuild the tendon from the inside out.
Phase 1: Pain Modulation and Decompression (Weeks 1-4)
The immediate goal is to stop the mechanical crushing and lower the extreme chemical sensitivity of the tendon.
The Anti-Stretch Mandate: We temporarily ban all deep forward folds, deadlifts, and prolonged sitting on hard surfaces.
Isometric Loading (The Painkiller): We utilize heavy, static holds. For example, lying on your back and pressing your heel into the floor with the knee slightly bent. The muscle fires intensely, but the hip does not bend, completely avoiding the painful wrap-around compression. Isometrics provide a massive, immediate reduction in tendon pain.
Shockwave Therapy: If the tendon has severe, chronic scarring, we apply Extracorporeal Shockwave Therapy (ESWT) to physically break down the fibrotic tissue and stimulate new blood vessel growth (neovascularization) directly at the sit bone.
Phase 2: Isotonic Loading in Neutral (Weeks 4-8)
Once the pain settles, we must rebuild the tendon's capacity to handle load, but we keep the hip out of deep flexion to protect the attachment site.
Prone Leg Curls and Glute Bridges: We utilize exercises where the hip remains relatively straight (neutral) while the hamstring works hard.
Heavy Slow Resistance (HSR): The tendon only lays down new, healthy collagen fibers when subjected to heavy, slow tension (e.g., 4 seconds lifting the weight, 4 seconds lowering it).
Phase 3: Energy Storage and Compressive Loading (Weeks 8-12)
The tendon is now strong, but we must prepare it for the real world. We slowly reintroduce the compressive movements you have been avoiding.
Gradual Deepening: We slowly reintroduce Romanian Deadlifts (RDLs) and kettlebell swings, controlling the depth to carefully train the tendon to handle being wrapped around the sit bone again.
Plyometric Integration: If you are a runner, we introduce bounding, skipping, and hill sprints. The tendon must relearn how to act like a rapid spring, storing and releasing energy without tearing.
Reclaim Your Flexibility and Strength
Do not let chronic sit bone pain force you to abandon your yoga mat, your running shoes, or your lifting routine. By understanding the mechanics of tendon compression and executing a precise loading strategy, you can completely rebuild your high hamstring.
Book a comprehensive biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports recovery in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Shockwave Therapy Dissolve Calcium Buildup in My Shoulder?
Yes. Extracorporeal Shockwave Therapy (ESWT) effectively treats calcific tendinitis without surgery. High-energy acoustic waves physically shatter the calcium deposits within the rotator cuff tendon, stimulate intense blood flow, and accelerate the body's natural cellular absorption of the painful calcification.
The Agony of the Frozen Calcium Shoulder
In the active, fast-paced neighborhoods of Queen West and Liberty Village, shoulder pain is an incredibly common complaint. Most patients assume their pain is a standard rotator cuff tear or simple muscle fatigue from overhead weightlifting, swimming, or long hours typing at a poorly positioned desk.
However, some patients experience a sudden, breathtaking spike in shoulder pain that is so agonizing they end up in the emergency room. They cannot lift their arm a single inch, and the pain disrupts their sleep entirely. When an X-ray is finally taken, the culprit is revealed: a large, dense lump of calcium sitting directly inside the rotator cuff tendon. This is known as Calcific Tendinitis.
When patients are diagnosed with this condition, they are often terrified that invasive arthroscopic surgery is the only way to "scrape" the calcium out. At Rehab Mechanics, we utilize cutting-edge physical modalities to treat this exact pathology. Extracorporeal Shockwave Therapy (ESWT) is the non-surgical gold standard for physically breaking down calcific deposits and restoring your shoulder’s structural mechanics.
Structural Analysis: The Mechanics of Calcific Tendinitis
To understand how sound waves can shatter bone-like deposits, we must perform a deep biological analysis of why your body decided to grow calcium inside a tendon in the first place.
The Anatomy of the Rotator Cuff
The rotator cuff is a group of four small muscles that stabilize the shoulder joint. The most frequently injured is the supraspinatus tendon, which runs across the top of the shoulder joint through a very narrow bony tunnel.
The Hypoxia Trigger (Lack of Oxygen)
Calcium does not randomly appear in healthy tissue. It forms as a biological response to chronic mechanical stress and a lack of oxygen (hypoxia).
The Compression: If you have poor posture (rounded shoulders), that narrow bony tunnel shrinks. Every time you reach overhead, you mechanically crush the supraspinatus tendon.
The Cellular Change: This constant crushing squeezes the blood out of the tendon. In this low-oxygen environment, the tendon cells undergo a bizarre transformation. They actually transform into bone-forming cells (chondrocytes) and begin depositing calcium salts directly into the soft tendon fibers.
The Three Phases of the Disease
Calcific tendinitis is highly unpredictable because it progresses through distinct phases, and the pain levels change drastically depending on the phase.
1. The Formative Phase
The calcium is actively being deposited. The crystal is hard and chalky. Surprisingly, this phase is often completely painless, or causes only a mild, dull ache.
2. The Resorptive Phase (The Agony)
This is when the severe, ER-visit level of pain strikes. The body realizes the calcium shouldn't be there and mounts a massive inflammatory attack to dissolve it.
The Toothpaste Effect: The hard calcium turns into a soft, toothpaste-like consistency. It swells rapidly, creating immense pressure inside the tendon and causing explosive, throbbing pain with any micro-movement.
3. The Post-Calcific Phase
The calcium is fully absorbed, and the tendon begins to heal with new collagen fibers.
Primary Source Proof: ESWT Efficacy
Orthopedic and sports medicine research universally endorses Extracorporeal Shockwave Therapy as a highly effective, non-invasive alternative to surgery for the eradication of calcific deposits in the rotator cuff.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for advanced modality rehabilitation.
The Rehab Mechanics Shockwave Protocol
We do not just hand you a generic stretching sheet for calcific tendinitis. We use advanced, clinical-grade shockwave technology to aggressively intervene in the disease process, followed by rigorous biomechanical correction.
Phase 1: Acoustic De-Calcification (ESWT)
Shockwave therapy is the absolute core of this treatment. It involves a handheld probe that delivers rapid, high-energy acoustic sound waves deep into the shoulder.
Mechanical Shattering: The high-pressure acoustic waves pass harmlessly through the soft tissue but hit the dense calcium deposit like a jackhammer. This mechanical force shatters the calcification into microscopic fragments.
Neovascularization: The trauma of the sound waves tricks the body into thinking a new injury has occurred. The body responds by growing brand-new capillary blood vessels (neovascularization) directly into the tendon. This massive influx of blood flushes away the shattered calcium fragments and provides the oxygen needed for the tendon to finally heal.
Pain Modulation: ESWT overwhelms the local nerve endings, dramatically dropping the concentration of Substance P (a pain neurotransmitter), providing significant pain relief after the session.
Phase 2: Joint Mobilization and Decompression
Once the shockwave breaks down the deposit, we must ensure the shoulder joint has the space to move without further crushing the healing tendon.
Inferior Glides: Our physiotherapists apply targeted, downward manual pressure to the humerus (arm bone). This creates physical space in the subacromial tunnel, ensuring the swollen tendon has room to glide.
Thoracic Unlocking: If your mid-back is frozen in a desk-worker slouch, your shoulder blades cannot rotate properly. We utilize high-grade spinal mobilizations to restore your thoracic extension.
Phase 3: Eccentric Loading and Neuromuscular Control
We must structurally rebuild the tendon so the calcium does not return.
Eccentric Rotator Cuff Training: Tendons rebuild their collagen optimally under slow, lengthening tension (eccentric loading). We prescribe highly specific resistance band protocols to stimulate healthy, parallel tendon growth.
Scapular Stabilization: Strengthening the serratus anterior and lower trapezius to ensure your shoulder blade pulls back and down during overhead lifting, permanently opening the bony tunnel and preventing the hypoxic crushing that started the disease.
Shatter the Pain, Avoid the Scalpel
You do not have to live with blinding shoulder pain or accept the risks of arthroscopic surgery. Advanced physical modalities like shockwave therapy can biologically erase the calcification and restore your shoulder's human mechanics.
Book a comprehensive shockwave assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite, technologically advanced orthopedic care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does Human Mechanics Physical Therapy Fix Chronic Groin Pain and Sports Hernias?
Yes. Chronic groin pain and athletic pubalgia are caused by a severe biomechanical sheer force between the abdominals and adductors. Human mechanics physical therapy resolves this by restoring pelvic balance, strengthening the core, and rebuilding the adductor tendons to withstand explosive athletic forces without surgery.
The End of the Playing Season
For the highly active demographic in Toronto—from weekend warriors playing soccer at Trinity Bellwoods to dedicated CrossFit athletes in Queen West—few injuries are as devastating and frustrating as chronic groin pain.
It often starts as a dull ache deep in the lower abdomen or inner thigh after a heavy sprint or a sudden change of direction. Over time, the pain becomes a sharp, stabbing sensation that makes sneezing, coughing, or getting out of bed excruciating. When athletes visit standard medical clinics, they are often told they have a "groin strain" or a "sports hernia" (athletic pubalgia) and are prescribed six weeks of complete rest.
However, complete rest almost never cures this condition. The moment the athlete returns to the field, the groin pain immediately flares up again. When these frustrated athletes search for "human mechanics physical therapy" or "sports rehabilitation centre," they are looking for a permanent solution. At Rehab Mechanics, we understand that a sports hernia is not a random tear; it is a profound failure of the biomechanical forces crossing the pelvis. To fix it, we must completely reconstruct your core-to-leg mechanical linkage.
Structural Analysis: The Battleground of the Pelvis
To permanently cure athletic pubalgia, we must perform a detailed structural analysis of the pubic symphysis—the joint where the two halves of your pelvis meet in the front.
The Biomechanical Tug-of-War
The pubic symphysis acts as a massive biomechanical anchor point for two of the most powerful muscle groups in the human body.
The Pull from Above: Your lower abdominal muscles (the rectus abdominis) attach to the top of the pubic bone. Their job is to pull the pelvis upward and stabilize the trunk.
The Pull from Below: Your adductor muscles (the inner thigh muscles) attach to the exact same bone from the bottom. Their job is to pull the leg inward and generate explosive lateral force.
The Mechanics of Athletic Pubalgia
A "sports hernia" is actually a misnomer; there is rarely an actual hole or herniation of the intestines. The true medical term is Athletic Pubalgia or Core Muscle Injury.
The Imbalance of Forces
The injury occurs when there is a massive imbalance in the tug-of-war at the pubic bone.
The Weak Core: In many athletes, the lower abdominal muscles become fatigued or neurologically inhibited.
The Overpowering Adductors: When an athlete makes a sudden, explosive cut on a soccer field or tennis court, the massive adductor muscles fire with tremendous force.
The Sheer Failure
Because the abdominals are too weak to anchor the top of the bone, the adductors violently rip the pubic symphysis downward. This creates massive sheer stress, leading to micro-tearing of the abdominal insertion, tearing of the adductor tendons, and severe, chronic inflammation of the pubic bone itself (Osteitis Pubis).
Treating the inner thigh alone is useless. You must rebuild the abdominal anchor to stop the sheer force.
Primary Source Proof: Sports Rehabilitation
Elite sports medicine research confirms that active, targeted strengthening of the abdominal and adductor complex is vastly superior to passive rest for resolving chronic groin pain and athletic pubalgia.
Download Clinical Efficacy PDF: The Efficacy of Active Physical Therapy and Adductor Strengthening in the Management of Athletic Pubalgia (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for sports rehabilitation.
The Rehab Mechanics Corrective Protocol
At our clinic inside the Prime Medical Centre, we treat athletic pubalgia by restoring the mechanical harmony between the upper and lower halves of your body.
Phase 1: Calming the Pubic Anchor
Before we can load the tendons, we must reduce the severe bone and tendon inflammation.
Soft Tissue De-Tethering: We use advanced manual therapy (Active Release Techniques) to strip the hyperactive adductor longus and pectineus muscles, reducing their constant, painful downward pull on the pubic bone.
Psoas and Hip Flexor Release: Tight hip flexors tilt the pelvis forward, further stretching the weakened abdominals. We must restore neutral pelvic alignment to give the core a mechanical advantage.
Phase 2: Restoring the Abdominal Anchor
We must rebuild the "pull from above" to counter the massive force of the legs.
Transversus Abdominis Activation: We utilize precise biofeedback to wake up the deep, stabilizing corset of the core.
Anti-Rotation and Anti-Extension Core Training: The core's true job is not to do sit-ups; it is to resist movement. We utilize Pallof presses, heavy loaded carries, and dead bug progressions to train the abdominals to lock the pelvis in place against the chaotic forces of the legs.
Phase 3: High-Load Adductor Remodeling (The Copenhagen Protocol)
Once the core is strong, we must rebuild the torn adductor tendons so they can handle explosive athletic forces without re-tearing.
Eccentric Adductor Loading: Tendons only thicken when subjected to heavy, eccentric loads. We utilize the evidence-based "Copenhagen Adductor Protocol," a progressive series of side-plank-based adductor raises that definitively rebuild inner thigh resilience.
Return-to-Sport Mechanics: We do not discharge you until we test your mechanics. We implement multi-directional lunges, plyometric bounding, and specific cutting drills to ensure your new core-to-leg linkage holds up on the field.
Return to Your Sport with Confidence
Do not let chronic groin pain end your athletic career or force you into unnecessary surgery. By analyzing and correcting the human mechanics of your pelvis, you can permanently resolve athletic pubalgia.
Book a comprehensive sports biomechanics assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is Remedial Physiotherapy the Only Way to Unfreeze a Frozen Shoulder?
Yes. A frozen shoulder requires highly specialized remedial physiotherapy to physically break down fibrotic capsular adhesions. Active joint mobilization, integrated medical management, and rigorous stretching protocols significantly shorten the "freezing" timeline, restoring the shoulder's full biomechanical range of motion safely.
The Agony of the Locked Joint
Of all the orthopedic conditions we treat at Rehab Mechanics in Queen West, few are as painful, frustrating, and psychologically draining as Adhesive Capsulitis, commonly known as "Frozen Shoulder."
It usually begins innocuously—a slight ache in the shoulder that mimics a mild muscle strain. Over the course of a few months, however, the pain becomes excruciating, especially at night. Then, the true nightmare begins: the shoulder physically locks. You cannot reach behind your back to put on a coat, you cannot reach overhead, and no matter how hard you or anyone else pulls on the arm, it simply will not move.
When patients frantically search for "prime physiotherapy" or "remedial mechanics" in Toronto, they are looking for a rapid cure. Unfortunately, frozen shoulder is a complex biological process that takes time to resolve. However, sitting at home and waiting for it to thaw is a massive mistake. Specialized remedial physiotherapy, particularly when integrated with medical interventions at a facility like the Prime Medical Centre, can drastically shorten the duration of the disease and permanently restore your upper body mechanics.
Structural Analysis: The Biology of the Freeze

To understand how to unfreeze a shoulder, we must perform a deep anatomical analysis of what is actually happening inside the joint capsule.
The Glenohumeral Joint Capsule
Your shoulder is a ball-and-socket joint. Surrounding this joint is a highly flexible, balloon-like sac of tissue called the joint capsule. This capsule is naturally loose, allowing your arm its massive, multi-directional range of motion.
The Pathology of Adhesive Capsulitis
For reasons that are still heavily researched (though highly correlated with metabolic conditions like diabetes, thyroid disorders, and periods of prolonged immobilization), this loose capsule becomes severely inflamed.
The Fibrotic Thickening
The body's inflammatory response causes the capsule to radically thicken and shrink. It transforms from a flexible balloon into a rigid, thick layer of fibrotic scar tissue that literally shrink-wraps itself around the ball of your upper arm bone.
The Capsular Pattern of Restriction
This shrink-wrapping creates a very specific, mechanical restriction known as a "capsular pattern."
First, you lose External Rotation (the ability to reach backward).
Next, you lose Abduction (the ability to lift the arm out to the side).
Finally, you lose Internal Rotation (the ability to reach up your back).
Because the restriction is the capsule itself, generic rotator cuff stretches or massages are entirely useless. The joint itself is tethered down.
Primary Source Proof: The Interdisciplinary Approach
Clinical orthopedic literature emphasizes that while frozen shoulder is self-limiting, combining intra-articular corticosteroid injections during the acute phase with aggressive, remedial physiotherapy yields vastly superior outcomes in pain reduction and range of motion restoration.
Download Clinical Efficacy PDF: The Efficacy of Intra-Articular Corticosteroids and Directed Manual Therapy in Adhesive Capsulitis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for capsular rehabilitation.
The Rehab Mechanics Remedial Protocol
Treating a frozen shoulder requires an understanding of its three distinct phases: Freezing, Frozen, and Thawing. Attempting the wrong treatment in the wrong phase will actually cause the capsule to thicken further.
Phase 1: The "Freezing" Phase (Pain Management)
During the first 2 to 9 months, the shoulder is actively inflaming and freezing. The pain is severe, constant, and highly irritable.
The Interdisciplinary Advantage: Because we are located inside the Prime Medical Centre on Abell Street, this is where co-management shines. We highly recommend consulting with the on-site physicians for an intra-articular corticosteroid injection. This powerful anti-inflammatory halts the active "freezing" process and provides immense pain relief.
Gentle ROM: During this phase, aggressive stretching is contraindicated (it will cause more inflammation). We use gentle, pain-free pendulum exercises and light Grade I joint mobilizations strictly to nourish the joint cartilage and prevent total decay.
Phase 2: The "Frozen" Phase (Mechanical Restoration)
Months 4 to 12. The severe, throbbing pain subsides, but the shoulder is now completely encased in rigid scar tissue. This is where remedial mechanics take over.
Aggressive Joint Mobilization: Our physiotherapists utilize high-grade (Grade III and IV) manual glides. We physically push the head of the humerus downward and backward within the socket to mechanically sheer and stretch the thickened capsular ligaments.
End-Range Stretching: Utilizing targeted, sustained stretching protocols (like the sleeper stretch and overhead pulley systems) to force the collagen fibers in the capsule to lengthen and adapt.
Phase 3: The "Thawing" Phase (Neuromuscular Rebuilding)
Months 12 to 24 (or faster with physiotherapy). The capsule begins to loosen naturally. We must rebuild the muscles that atrophied during the frozen year.
Scapular Dyskinesis Correction: Because your arm couldn't move for a year, you spent 12 months aggressively hiking your shoulder blade to compensate. We must retrain the serratus anterior and lower trapezius to stabilize the scapula correctly.
Rotator Cuff Loading: Progressively reloading the rotator cuff tendons using heavy slow resistance to ensure the shoulder joint is strong and centralized as you reclaim your full range of motion.
Accelerate Your Shoulder Recovery
You do not have to suffer through years of agonizing restriction waiting for a frozen shoulder to thaw on its own. Through integrated medical care and precise, remedial physical therapy, you can break the capsular restriction and reclaim your mechanics.
Book a comprehensive upper body assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Body Mechanics Physiotherapy Stabilize Spondylolisthesis and Spinal Slippage?
Yes. Physiotherapy stabilizes spondylolisthesis by completely overhauling your spinal mechanics. By aggressively strengthening the deep multifidus muscles, restoring pelvic alignment, and improving load transfer, physical therapy prevents further vertebral slippage, relieves nerve compression, and frequently prevents the need for spinal fusion surgery.
The Fear of a Shifting Spine
When patients in Toronto receive a diagnosis of "Spondylolisthesis" following a lumbar X-ray or MRI, the reaction is almost always one of sheer panic. The medical explanation—that one of the vertebrae in your lower back has literally slipped forward over the bone beneath it—paints a terrifying mental image of a spine on the verge of total collapse.
Patients immediately restrict their movement, terrified that bending over to pick up a box or going for a run along the Martin Goodman Trail will cause their spine to snap. They begin searching for "spinal mechanics" or "prime medical centre physical therapy," desperate for an alternative to highly invasive spinal fusion surgery.
At Rehab Mechanics, we want to dispel this fear. While spondylolisthesis is a serious structural defect, the human body is incredibly adaptable. Unless the slippage is catastrophically severe (Grade 3 or 4 with progressive neurological loss), the spine can be biologically stabilized. By applying advanced body mechanics physical therapy, we can build a muscular brace so strong that it completely compensates for the bony instability, allowing you to return to heavy lifting, sports, and a pain-free life.
Structural Analysis: The Mechanics of Spinal Slippage
To understand how physical therapy prevents spinal surgery, we must perform a deep biomechanical analysis of how and why a vertebra slips out of place.
The Anatomy of the Defect
Spondylolisthesis most commonly occurs in the lower lumbar spine, typically where the L4 vertebra meets L5, or where L5 meets the sacrum (S1).
The Pars Interarticularis
The back of each vertebra has a small, thin bridge of bone called the pars interarticularis. This bridge connects the upper facet joints to the lower facet joints, locking the vertebrae together like a chain.
The Stress Fracture (Spondylolysis)
In highly active populations (such as gymnasts, weightlifters, or those with physically demanding jobs in downtown Toronto), repetitive arching of the lower back places immense stress on this bony bridge. Over time, this stress can cause a micro-fracture. When the bone breaks, it is called spondylolysis.
The Slippage (Spondylolisthesis)
Once the bony bridge is broken, the structural lock is gone. Because the lower spine sits on a naturally downward-sloping angle (the sacral slope), gravity and body weight slowly push the broken vertebra forward. This forward slip is spondylolisthesis.
The Neurological Consequences
When the vertebra slips forward, it begins to narrow the spinal canal and the neural foramina (the holes where the nerves exit).
Nerve Root Compression: The slipping bone physically pinches the exiting nerve roots, causing severe sciatica, numbness, or a deep burning sensation down the back of the legs.
The "Hinge" Effect: Because the bony lock is broken, that specific segment of the spine becomes hypermobile. It wiggles and hinges excessively with every step you take, causing acute, stabbing muscle spasms as your brain desperately tries to stabilize the area.
Primary Source Proof: Stabilizing the Slippage
Orthopedic surgical guidelines now strongly mandate that a rigorous course of specific, flexion-biased lumbar stabilization must be exhausted before spinal fusion is considered for low-grade spondylolisthesis.
Download Clinical Efficacy PDF: The Efficacy of Specific Core Stabilization Exercise in the Treatment of Lumbar Spondylolisthesis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for spinal rehabilitation.
The Rehab Mechanics Corrective Protocol
Treating spondylolisthesis is entirely different from treating a standard herniated disc. In fact, many standard back stretches will make this condition worse. We must utilize highly specific "remedial mechanics" to anchor the spine.
Phase 1: Halting the Extension Overload
The absolute most important rule of rehabbing a slipped vertebra is avoiding spinal extension (arching the back). Arching pushes the bone further forward.
Flexion-Biased Posture: We immediately teach you how to maintain a slightly flattened lower back. This physically opens up the nerve holes and pulls the slipped vertebra backward into a safer position.
Psoas Release: The deep hip flexors (psoas) attach to the front of the lumbar spine. If they are tight, they actively drag the slipping vertebra forward. We use advanced manual therapy to release this massive muscle, instantly reducing the sheer force on the spine.
Phase 2: Building the Internal Brace
Since the bone is broken, the muscles must take over 100% of the stabilization duties.
Transversus Abdominis (TVA) Isolation: This is the deepest abdominal muscle. We use precise biofeedback to train your brain to fire the TVA instantly before you move. This acts as a rigid, internal weight belt that locks the slipping segment in place.
Multifidus Fortification: The multifidus muscles are tiny, powerful stabilizers that run directly up the spine. In patients with spondylolisthesis, these muscles undergo rapid fatty atrophy. We utilize targeted, isometric holds to resurrect these dormant muscles.
Phase 3: Dynamic Biomechanical Integration
A strong core is useless if your body mechanics fall apart when you walk or lift.
Hip Hinge Mechanics: We must teach your body to bend purely at the hip joints, rather than bending at the unstable spinal segment. You will relearn how to squat and deadlift using the massive power of your glutes and hamstrings, completely bypassing the lower back.
Anti-Extension Core Training: Utilizing exercises like heavy farmer's carries, dead bugs, and plank variations to train the core to resist any forces that try to pull the spine into an arch.
Secure Your Foundation
You do not have to live in fear of your spine failing. By systematically upgrading your body mechanics and building a biological brace, you can safely manage spondylolisthesis and avoid invasive fusion surgery.
Book a comprehensive spinal biomechanics assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author

Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Fix Chronic Jaw Pain and TMJ Dysfunction?
Yes. Temporomandibular Joint (TMJ) dysfunction is a mechanical failure often linked to cervical spine posture. Physiotherapy cures TMJ pain by releasing hyperactive jaw muscles, restoring upper neck mobility, and correcting the biomechanical alignment of the skull and jawbone.
The Hidden Mechanics of Jaw Pain
If you wake up with a dull, throbbing headache, experience sharp clicking when you chew, or find it painful to fully open your mouth, you are likely suffering from Temporomandibular Joint (TMJ) Dysfunction.
Many Toronto residents assume that because the jaw is filled with teeth, any pain in that area must be handled exclusively by a dentist. While dental night guards can protect your teeth from the damage of grinding (bruxism), they do not fix the structural muscles and joints that are actually causing the jaw to deviate, click, and lock.
When patients seek advanced "human mechanics physical therapy" at Rehab Mechanics, they are often shocked to learn that their chronic jaw pain is fundamentally a mechanical, orthopedic issue. The jaw is a joint, just like a knee or a shoulder. Furthermore, its function is intimately tied to the posture of your neck. By addressing the deep musculature of the face and the alignment of the cervical spine, specialized physiotherapy can permanently resolve TMJ pain.
Structural Analysis: The Biomechanics of the Jaw
To understand how physical therapy cures jaw pain, we must perform a biomechanical analysis of the TMJ and its connection to the rest of the kinetic chain.
The Anatomy of the TMJ
The Temporomandibular Joint is one of the most complex joints in the human body.
The Hinge and Glide: When you open your mouth, the jawbone (mandible) doesn't just hinge open; it must also glide forward out of its socket to allow for a wide stretch.
The Articular Disc: Sitting between the jawbone and the skull is a tiny, cartilaginous disc. Its job is to absorb the massive shock of chewing and ensure a smooth, frictionless glide.
The Mechanics of TMJ Dysfunction
TMJ pain occurs when the muscles controlling the jaw become severely imbalanced, usually pulling the jawbone out of alignment and crushing that delicate articular disc.
The "Tech Neck" Connection
The most common driver of TMJ dysfunction in urban professionals is forward head posture ("Tech Neck").
The Pull of the Neck: When you stare at a laptop, your head shifts forward. This violently stretches the muscles on the front of your neck, which attach directly to your jawbone.
The Downward Drag: This constant, unnatural tension physically pulls the lower jaw backward and downward.
The Muscular Spasm (Masseter and Pterygoids)
To prevent your mouth from hanging open due to this downward drag, your primary chewing muscles—the Masseter and the deep Pterygoids—must work in constant, low-level overdrive to keep your jaw shut.
Over time, these muscles form dense, agonizing trigger points (muscle knots). Because one side usually gets tighter than the other, the jawbone gets pulled off-center. Now, every time you open your mouth, the misaligned jawbone snaps over the articular disc, causing a loud, painful "click."
Primary Source Proof: TMJ and Cervical Rehabilitation
Clinical orthopedic research explicitly links TMJ dysfunction with cervical spine pathology and highlights the superiority of targeted physiotherapy in managing both systems simultaneously.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for maxillofacial and cervical rehabilitation.
The Rehab Mechanics TMJ Protocol
Treating the TMJ requires a highly specialized, inside-out approach. At our Prime Medical Centre clinic, we systematically reset the mechanics of your head, neck, and jaw.
Phase 1: Advanced Intra-Oral Release
We must release the primary structural brakes holding the jaw out of alignment. Because the most important jaw muscles are located inside the mouth, this requires specialized intra-oral therapy.
Lateral and Medial Pterygoid Release: The physiotherapist uses a gloved hand to gently reach inside the mouth and apply sustained pressure to the tiny, hyperactive muscles behind the cheek. This often provides instant, profound relief from jaw locking.
Masseter and Temporalis Deactivation: Using deep, external myofascial release on the side of the face and temples to eliminate the trigger points that cause massive tension headaches.
Phase 2: Restoring Cervical Arthrokinematics
We must fix the foundation that the jaw rests upon.
Upper Cervical Mobilization: Un-jamming the C1 and C2 vertebrae at the base of the skull. A stiff upper neck severely alters the neurological resting tone of the jaw muscles.
Postural Decompression: Utilizing gentle manual traction to restore the natural curve of the neck, taking the stretching pressure off the anterior neck muscles and allowing the jaw to rest in a neutral position.
Phase 3: Neuromuscular Re-Education (Mandibular Tracking)
Once the joints are mobile and the muscles are relaxed, we must teach the jaw how to open smoothly again.
Rocabado's 6x6 Exercises: We prescribe highly specific micro-movements designed to retrain the brain's motor control over the jaw.
Mid-Line Tracking: Utilizing mirrors and controlled resistance to ensure the jawbone hinges and glides perfectly straight, preventing it from deviating to one side and clicking over the articular disc.
Deep Cervical Flexor Training: Rebuilding the deep neck muscles to permanently correct the "Tech Neck" posture, ensuring the root cause of the TMJ drag never returns.
Stop Suffering from Chronic Face and Jaw Pain
You do not have to live with a clicking jaw, painful chewing, or daily tension headaches. By correcting the structural mechanics of your head and neck, you can eliminate the forces destroying your TMJ.
Book a specialized TMJ and cervical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite human mechanics rehabilitation in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.

His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Cure Chronic, Unexplained Body Pain?
Yes. Chronic, widespread pain is often driven by central sensitization—a hypersensitive nervous system. Advanced physiotherapy utilizes graded motor imagery, pain neurophysiology education, and progressive mechanical loading to recalibrate your nervous system and permanently dial down chronic pain signals.
The Nightmare of Daily Chronic Pain
For patients dealing with chronic, daily pain, navigating the medical system is often an incredibly demoralizing experience. You have sharp pain in your back, aching in your knees, and tension in your neck. You visit your doctor, they order MRIs, blood work, and X-rays, but all the scans come back "normal."
When patients in Toronto search for "chronic pain management" or click on our "defeating daily chronic pain" resources, they are looking for validation. The fact that the scans are clean does not mean the pain is "all in your head." Your pain is 100% real. However, the source of the pain has shifted.
At Rehab Mechanics, we specialize in the complex neurology of pain. We understand that if you have been in pain for more than 3 to 6 months, you are no longer dealing with a simple tissue injury (like a sprained ankle). You are dealing with an overprotective nervous system. Curing chronic pain requires a radical shift in treatment: we must stop treating the muscles and start treating the central nervous system.
Structural Analysis: The Mechanics of Central Sensitization
To understand how to defeat chronic pain, we must perform a deep analysis of how your brain processes danger signals.
The Alarm System Metaphor
Pain is not an input; it is an output. Pain is an alarm system created by your brain to protect you from perceived danger.
Acute Pain: If you touch a hot stove, the nerves in your hand send a "danger" signal to your brain. Your brain processes that danger and outputs "pain" to force you to move your hand. Once the burn heals, the alarm system resets.
Chronic Pain (Sensitization): In cases of chronic pain, the original injury (e.g., a minor lower back strain) heals entirely within 6 to 8 weeks. However, the alarm system never resets.
The Hypersensitive Nervous System
Central Sensitization occurs when your spinal cord and brain become hyper-excitable. The alarm system becomes so sensitive that it triggers a massive pain response to completely harmless activities.
Allodynia and Hyperalgesia
This neurological rewiring leads to two specific clinical phenomena:
Allodynia: Feeling pain from a stimulus that should not normally provoke pain (e.g., light pressure, a cold breeze, or simply bending over to tie your shoe).
Hyperalgesia: An exaggerated, agonizing pain response to a mildly uncomfortable stimulus.
The Cycle of Fear and Avoidance
When normal movement hurts, patients naturally stop moving. This is called "fear-avoidance." Unfortunately, absolute rest weakens the muscles, stiffens the joints, and makes the brain more hypersensitive, creating a devastating downward spiral of chronic disability.
Primary Source Proof: Pain Neurophysiology
Contemporary pain science and neurological research explicitly mandate that chronic pain must be treated through a biopsychosocial model, prioritizing nervous system recalibration over passive, tissue-based treatments.
Download Clinical Efficacy PDF: The Efficacy of Pain Neuroscience Education and Graded Exposure in the Treatment of Chronic Centralized Pain (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for chronic pain rehabilitation.
The Rehab Mechanics Chronic Pain Protocol
Treating central sensitization requires a complete departure from traditional physical therapy. We do not chase the pain with ice packs and massage; we actively rewrite the brain's danger software.
Phase 1: Pain Neuroscience Education (PNE)
The first step in curing chronic pain is understanding it.
De-Threatening Movement: We spend significant clinical time teaching you how your nervous system works. Once you deeply understand that the pain you feel when bending over does not mean your spine is tearing, the fear drastically decreases.
The Neurological Shift: Lowering the fear response instantly decreases the amount of adrenaline and cortisol in your bloodstream, which chemically lowers the volume of the pain alarm.
Phase 2: Graded Motor Imagery and Desensitization
We must slowly prove to your brain that movement is safe.
Tactile Desensitization: Using various textures and gentle manual therapies to re-accustom the hyperactive nerves to normal touch without triggering an alarm.
Visualization: In severe cases, we have patients visualize performing a painful movement without actually doing it. This activates the motor cortex in the brain without triggering the pain response, laying the groundwork for safe movement.
Phase 3: Graded Exposure and Progressive Loading
This is the physical cure. We systematically expose your body to the mechanical loads you have been avoiding.
Finding the Baseline: We find the exact amount of exercise you can do without triggering a massive flare-up (your baseline).
Micro-Progressions: We slowly, methodically increase the physical demand (e.g., progressing from lifting 2 lbs to 5 lbs).
Biological Resilience: Over time, this graded mechanical loading builds incredibly strong tissues while simultaneously proving to your nervous system that it no longer needs to sound the pain alarm.
Break the Cycle of Chronic Pain
You do not have to let an overprotective nervous system dictate the boundaries of your life. Through integrated medical care and advanced biomechanical rewiring, you can reclaim your active lifestyle.
Book a comprehensive chronic pain assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced interdisciplinary care in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Do I Really Need to Do My Prescribed Home Physiotherapy Exercises?
Yes. In-clinic physiotherapy unlocks joint mobility and reduces acute pain, but your home exercises permanently rewire your nervous system. Failing to perform prescribed home exercises prevents your tissues from building long-term load capacity, virtually guaranteeing your injury will return.
The "167-Hour" Rehabilitation Rule
A common scenario at Rehab Mechanics in Queen West involves patients experiencing profound relief after a clinical session, only to return a week later complaining that their stiffness and pain have crept back. When asked if they completed their prescribed home exercise program (HEP), the answer is frequently a sheepish, "I didn't have time."
This highlights a fundamental misunderstanding of how the human body heals. We call it the "167-Hour Rule." There are 168 hours in a week. If you spend one hour in our clinic receiving advanced manual therapy, joint mobilizations, and shockwave therapy, you feel fantastic. However, you spend the remaining 167 hours of the week in the exact same postures, performing the exact same repetitive movements that caused your injury in the first place.
When patients search our site for "why are your prescribed home physiotherapy exercises so important," they are looking for the biomechanical truth. Your time in the clinic acts as the catalyst; it removes the physical roadblocks to healing. But the actual reconstruction of your tendons, muscles, and neurological pathways happens entirely through the consistent, daily mechanical loading provided by your home exercises.
Structural Analysis: The Biology of Tissue Remodeling
To understand why home exercises are non-negotiable, we must analyze the biological principles of tissue repair and adaptation.
Mechanotransduction: How Cells Respond to Load
Tendons, ligaments, and muscle fibers do not heal simply because time passes. They heal through a process called mechanotransduction.
The Mechanical Signal: When you perform a specific resistance exercise, you apply mechanical tension to the damaged cells.
The Chemical Conversion: The cells convert this mechanical stretch into biochemical signals.
Collagen Synthesis: These biochemical signals instruct your DNA to produce new, healthy collagen fibers to repair micro-tears and thicken the tissue.
The Requirement for Frequency
Mechanotransduction is highly dependent on frequency.
The Half-Life of Healing: The cellular signal that triggers collagen production only lasts for about 36 to 48 hours after an exercise session.
The Consistency Factor: If you only exercise once a week in the clinic, your tissues spend five days in a dormant, non-healing state. By doing your home exercises every day (or every other day, as prescribed), you keep the collagen-building signal turned "on" continuously.
Neuromuscular Re-Education (Neuroplasticity)
Chronic pain physically changes your brain. It alters your motor cortex, causing you to move dysfunctionally to avoid pain.
Rewiring the Brain
Manual therapy cannot rewire a brain. Only repetitive movement can.
Motor Engrams: When you perform a corrective exercise—like a deep cervical flexor chin tuck for "Tech Neck" or a glute bridge for lower back pain—you are firing a specific neurological pathway.
Repetition is Key: To make this new, healthy movement pattern automatic (a motor engram), your nervous system requires thousands of repetitions. Your home exercise program provides the necessary volume to overwrite the old, painful movement habits.
Primary Source Proof: Exercise Adherence
Clinical sports medicine and orthopedic research unequivocally demonstrate that patient compliance with a home exercise program is the single greatest predictor of long-term success and reduced recurrence rates in musculoskeletal rehabilitation.
Download Clinical Efficacy PDF: The Impact of Home Exercise Compliance on Long-Term Functional Outcomes in Musculoskeletal Physiotherapy (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for patient adherence.
The Rehab Mechanics Prescription Model
At our Prime Medical Centre location, we do not hand you a generic photocopy of 15 different stretches. We believe in precision, minimalism, and structural integration.
Phase 1: Micro-Dosing Movement
When you are in acute pain, the thought of a 30-minute workout is daunting.
The Strategy: We prescribe "micro-doses" of exercise. These are one or two highly specific movements (e.g., isometric holds) that take less than 60 seconds to perform.
The Implementation: We ask you to perform these micro-doses multiple times throughout your workday—such as every time you take a sip of water or stand up from your desk. This prevents tissue stiffness without causing fatigue.
Phase 2: Progressive Overload
As your tissue heals, your exercises must become harder. Doing the same light resistance band exercise for six weeks will result in a plateau.
Tissue Capacity: We progressively increase the load (weight), volume (reps), or complexity of your home exercises.
The Goal: We must push your tissues slightly beyond their current capacity to force them to adapt and grow stronger, ensuring they can handle the chaotic forces of the Toronto urban lifestyle.
Phase 3: Integration into Daily Life
The ultimate goal of a home exercise program is for it to cease being an "exercise" and become a permanent biomechanical habit.
Functional Phasing: We transition your isolated clinical exercises into complex, real-world movements (like squats, deadlifts, and loaded carries).
The Autopilot Effect: By this phase, your nervous system automatically fires the correct stabilizing muscles, permanently protecting your joints from future injury.
Commit to Your Own Recovery
Physiotherapy is not something that is "done to you"; it is a partnership. We provide the biomechanical blueprint, the manual therapy, and the clinical guidance. You provide the consistency.
Take control of your structural health. Book a comprehensive assessment with our clinical team today and get a customized movement blueprint. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
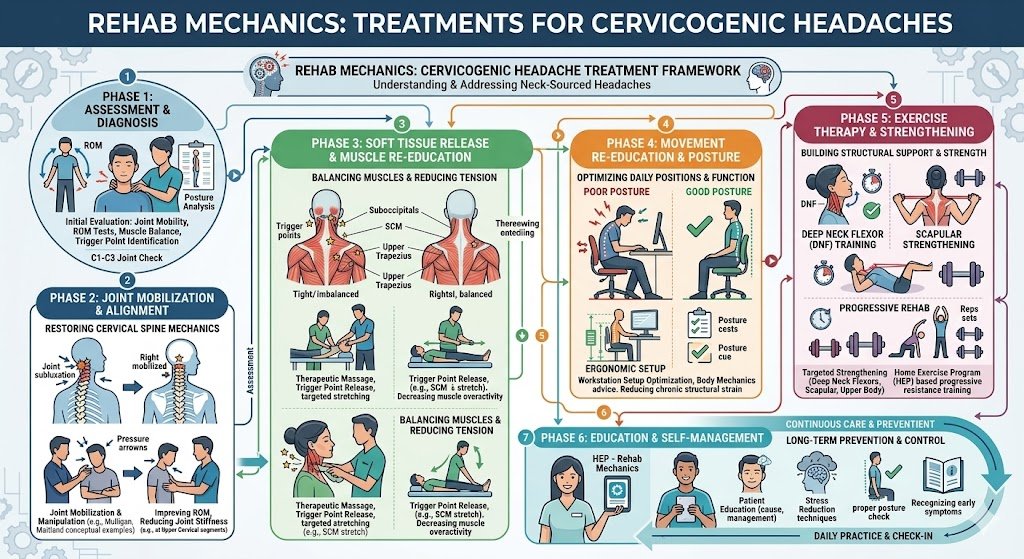
Can Physiotherapy Prevent Surgery for a Hip Labral Tear?
Yes. Advanced physiotherapy effectively manages hip labral tears and Femoroacetabular Impingement (FAI) without surgery. By correcting pelvic mechanics, improving joint capsule mobility, and strengthening deep hip stabilizers, physical therapy stops the bone-on-bone friction that destroys the labrum.
The Agony of the "C-Sign" Hip Pain
For the highly active demographic in Trinity Bellwoods and Queen West, hip pain is a frequent and devastating issue. Runners, weightlifters, and even chronic desk workers often experience a deep, pinching pain in the front of their groin that refuses to go away with stretching.
When a patient cups their hand around the side of their hip—forming a "C" shape with their thumb and index finger—to point out where it hurts, it is a classic clinical indicator. This is known as the "C-Sign," and it strongly suggests intra-articular hip joint pathology, most commonly a labral tear driven by Femoroacetabular Impingement (FAI).
When these patients search for a "sports rehabilitation centre" or "prime physiotherapy" in Toronto, they are often terrified that arthroscopic hip surgery is their only option. At Rehab Mechanics, we heavily focus on conservative orthopedic management. While massive structural tears may require surgery, the vast majority of labral pain can be completely resolved by fixing the biomechanical faults that cause the hip to impinge in the first place.
Structural Analysis: The Mechanics of a Hip Impingement
To understand how physical therapy saves the hip joint, we must perform a detailed anatomical analysis of FAI and labral pathology.
The Acetabular Labrum
Your hip is a deep ball-and-socket joint.
The Anatomy: The "ball" is the head of your femur (thigh bone), and the "socket" is the acetabulum (part of your pelvis).
The Gasket: The labrum is a ring of tough fibrocartilage that lines the rim of the socket. It acts like a rubber gasket, deepening the socket to create a suction seal that holds the fluid inside the joint and provides massive structural stability.
The Mechanics of FAI (Femoroacetabular Impingement)
A labral tear rarely happens from a single trauma. It usually happens because the bones of the hip joint are abnormally shaped and constantly grind against each other, a condition known as FAI.
The Two Types of Friction
Cam Impingement: The ball (femoral head) is not perfectly round. It has a bony bump on it. When you bend your knee up to your chest (like in a deep squat or running), that bony bump violently grinds against the edge of the socket, tearing the labrum.
Pincer Impingement: The socket (acetabulum) has too much overhang. It physically pinches the neck of the femur during normal movement, crushing the labrum in between the bones.
The Biomechanical Escalation
While you cannot exercise away an abnormal bone shape, you can control how the femur moves within the socket. If your deep gluteal stabilizers are weak, the head of the femur glides forward and upward during movement, drastically increasing the bone-on-bone collision. Physiotherapy teaches the joint to remain centralized, eliminating the friction.
Primary Source Proof: Conservative Orthopedics
Orthopedic surgical literature increasingly mandates that a trial of targeted, biomechanical physiotherapy is the gold standard of care before arthroscopic hip surgery is considered for FAI and labral tears.
Download Clinical Efficacy PDF: Conservative Physiotherapy Management of Femoroacetabular Impingement and Hip Labral Tears (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for sports rehabilitation.
The Rehab Mechanics FAI Protocol
We treat labral tears by altering the biomechanics of the pelvis and femur to maximize the clearance space within the joint capsule.
Phase 1: Creating Joint Space and Pain Relief
The immediate goal is to stop the pinching and calm the acutely inflamed labral tissue.
Capsular Mobilization: If the back of your hip capsule is stiff, it physically pushes the femur forward into the painful impingement zone. Our physiotherapists utilize heavy manual mobilizations and joint tractions to stretch the posterior capsule, instantly restoring joint space.
Hip Flexor Release: The psoas and rectus femoris run directly over the front of the hip joint. When tight, they compress the joint severely. We use deep myofascial release to un-tether these structures.
Activity Modification: We implement strict, temporary avoidance of deep hip flexion (like deep squats or sitting in low chairs) to prevent further mechanical crushing of the torn labrum.
Phase 2: Neuromuscular Re-Centering
We must build a dynamic muscular corset to hold the femur perfectly in the center of the socket.
Deep Rotator Activation: Just like the rotator cuff in the shoulder, the hip has deep internal stabilizing muscles (the obturators and gemelli). We prescribe specific isometric holds to wake these muscles up, allowing them to pull the femoral head firmly into the socket.
Gluteus Medius Fortification: This is the primary lateral stabilizer of the pelvis. Utilizing heavy, banded lateral walks and clamshell progressions to ensure the pelvis does not drop and cause the femur to impinge during walking or running.
Phase 3: Advanced Load and Sport Integration
Once the hip is centralized and pain-free, we rebuild its capacity to handle the explosive forces of the Toronto sports lifestyle.
Heavy Slow Resistance (HSR): Utilizing controlled deadlifts, step-ups, and split squats to strengthen the entire posterior chain without forcing the hip into painful, deep flexion angles.
Core-Pelvic Synchronization: The core and the hip must work as one unit. We integrate dynamic core stabilization drills to ensure the pelvis does not tilt forward during athletic movements, which is the primary trigger for FAI flare-ups.
Protect Your Hip Joint Naturally
A diagnosis of a labral tear or FAI does not automatically mean your active life is over, nor does it guarantee a trip to the operating room. By meticulously correcting your hip mechanics, you can eliminate the destructive friction and heal naturally.
Book a specialized orthopedic hip assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite sports rehabilitation in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is Scapular Dyskinesis the Hidden Cause of Your Shoulder Pain?
Yes. Scapular dyskinesis—the abnormal movement of your shoulder blades—forces the rotator cuff to overwork and tear. Physiotherapy restores proper scapular mechanics by strengthening the serratus anterior and lower trapezius, instantly relieving impingement and permanently curing chronic shoulder pain without the need for surgery.
The Shoulder Joint is a Biomechanical Illusion
When residents of Queen West experience sharp pain while lifting a coffee mug or reaching for a high shelf, they naturally assume the problem lies entirely within the shoulder joint itself. They ice the top of their arm, rub anti-inflammatory cream into their deltoid, and hope for the best.
However, the human shoulder is a biomechanical illusion. The actual ball-and-socket joint of the shoulder is incredibly shallow. Its entire foundation, stability, and movement capacity rely completely on a floating bone on your back: the scapula (shoulder blade).
When patients search for "human mechanics physical therapy" or "queen street physiotherapy" to fix stubborn shoulder pain, they are looking for a clinician who understands this connection. At Rehab Mechanics, we frequently diagnose a condition called Scapular Dyskinesis. This simply means your shoulder blade is moving incorrectly. If your shoulder blade moves poorly, your rotator cuff is guaranteed to fail.
Structural Analysis: The Mechanics of Scapular Dyskinesis
To permanently resolve upper body pain, we must perform a biomechanical analysis of the scapulo-humeral rhythm—the intricate dance between the arm bone and the shoulder blade.
The Foundation of the Arm
The scapula is the structural base for your entire arm. It is suspended purely by a complex web of 17 different muscles attaching it to the ribcage and spine.
The Moving Platform: When you lift your arm overhead, the ball-and-socket joint does not do all the work. The scapula itself must upwardly rotate and tilt backward to make room for the arm bone to rise.
The Synchronization: This synchronized movement is called the scapulo-humeral rhythm. For every 2 degrees your arm lifts, your shoulder blade must rotate 1 degree.
The Breakdown: What Causes Dyskinesis?
Scapular dyskinesis occurs when the muscles stabilizing the shoulder blade become chronically imbalanced, usually due to the modern "Tech Neck" desk posture.
The Weak Serratus Anterior
The serratus anterior is a fan-shaped muscle that wraps around your ribs. Its primary job is to hold the shoulder blade flat against your ribcage during movement.
The "Winging" Effect: When the serratus anterior becomes weak, the inner edge of the shoulder blade pops off the ribcage. This is clinically referred to as "scapular winging."
Loss of Upward Rotation: A weak serratus cannot properly rotate the scapula upward when you reach overhead.
The Rotator Cuff Impingement
Because the shoulder blade fails to rotate upward out of the way, the heavy bone of the upper arm (humerus) smashes directly into the roof of the shoulder blade (the acromion).
This violent, repetitive smashing crushes the delicate rotator cuff tendons trapped in between. The resulting sharp, stabbing pain is known as Subacromial Impingement. Treating the torn tendon is useless if you do not fix the scapular dyskinesis that caused the crushing in the first place.
Primary Source Proof: Scapular Kinematics
Orthopedic sports medicine literature explicitly mandates that rehabilitating scapular kinematics is an absolute prerequisite for treating rotator cuff tendinopathy and shoulder impingement syndrome.
Download Clinical Efficacy PDF: The Role of Scapular Kinematics in the Rehabilitation of Rotator Cuff Tendinopathy and Shoulder Impingement (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for upper extremity mechanics.
The Rehab Mechanics Corrective Protocol
At our clinic inside the Prime Medical Centre, we do not focus solely on the rotator cuff. We rebuild the entire scapular foundation.
Phase 1: Releasing the Scapular Brakes
Before the shoulder blade can move correctly, we must release the tight muscles anchoring it down.
Pectoralis Minor Release: This small chest muscle attaches directly to the front of the scapula. When tight from desk work, it violently pulls the shoulder blade into a forward tilt. We use deep myofascial release to lengthen this tissue.
Levator Scapulae Deactivation: The muscle running from the neck to the top of the shoulder blade often goes into severe spasm, hiking the shoulder up to the ear. Targeted trigger point therapy forces this muscle to relax.
Thoracic Spine Mobilization: If your mid-back is frozen in a hunched position, the shoulder blade cannot glide over it. We perform aggressive joint mobilizations to restore thoracic extension.
Phase 2: Neuromuscular Re-education (The Force Couples)
We must teach the brain how to fire the correct muscles in synchrony to stabilize the moving platform.
Serratus Anterior Activation: We utilize exercises like "scapular push-ups" and wall slides to isolate and wake up this crucial stabilizing muscle, instantly stopping the shoulder blade from winging.
Lower Trapezius Strengthening: The lower traps are responsible for pulling the shoulder blade down and away from the impingement zone. We prescribe targeted Y-raises and prone lifts to rebuild this neglected muscle group.
Phase 3: Dynamic Integration and Load Tolerance
The final phase ensures your shoulder mechanics hold up under real-world stress.
Closed Kinetic Chain Exercises: Utilizing medicine ball walk-outs and plank variations to force the scapula to stabilize the entire weight of the upper body.
Rhythmic Stabilization: The physiotherapist applies unexpected, multidirectional forces to your arm while you hold it in space. This trains the nervous system to react instantly, firing the scapular stabilizers to protect the joint during chaotic, athletic movements.
Rebuild Your Upper Body Mechanics
Do not let chronic shoulder impingement lead to a complete rotator cuff tear. By fixing your scapular dyskinesis, you can eliminate the mechanical friction destroying your tendons.
Book a comprehensive biomechanical upper body assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Fixing Your Pelvic Tilt Cure Chronic Lower Back Pain?
Yes. Anterior pelvic tilt dramatically compresses the lumbar spine, causing chronic lower back pain. Biomechanical physiotherapy corrects this by releasing tight hip flexors and strengthening the deep core and glutes, restoring neutral alignment and eliminating the structural nerve compression causing your pain.
The Hidden Epidemic of Postural Back Pain
If you are a professional working in downtown Toronto, you are likely sitting for eight to ten hours a day. Over time, you may notice a deep, aching tightness in your lower back that simply will not go away. You might try stretching your back, applying heat pads, or getting generic massages, but the pain always returns the moment you sit back down at your desk.
When local residents search for "body mechanics physiotherapy" or "remedial mechanics," they are often unknowingly suffering from a profound postural distortion known as an Anterior Pelvic Tilt (APT).
At Rehab Mechanics, located in Queen West, we understand that lower back pain is rarely a problem with the back itself. It is a mechanical problem with the pelvis. Your pelvis acts as the foundational bowl upon which your spine rests. If that foundation is tilted out of alignment, the spine is subjected to massive, unnatural shearing forces. Fixing the mechanics of your pelvis is the definitive cure for this type of chronic lumbar pain.
Structural Analysis: The Mechanics of Anterior Pelvic Tilt
To permanently resolve lumbar pain, we must perform a biomechanical analysis of how the muscles of the hip control the alignment of the spine.
Lower Crossed Syndrome
Medical professionals refer to the muscular imbalance that causes an anterior pelvic tilt as "Lower Crossed Syndrome."
The Cross Pattern: This syndrome is characterized by a specific cross-pattern of overactive (tight) muscles and underactive (weak) muscles in the lumbo-pelvic region.
The Culprits: The hip flexors (front of the hips) and the erector spinae (lower back muscles) become chronically tight.
The Victims: The gluteus maximus (buttocks) and the transversus abdominis (deep core) become elongated, weak, and neurologically inhibited.
The Physics of the Tilt
When you sit at a desk all day, your hip flexors—specifically the massive psoas major muscle—are kept in a shortened position.
The Forward Pull
Over time, these muscles adaptively shorten. Because the psoas attaches to the front of your lumbar spine and the top of your femur, its tightness pulls the front of your pelvis downward and forward.
Spinal Compression
When the front of the pelvis tips forward, the lower back is forced into extreme hyperextension (a deep, exaggerated arch).
Facet Joint Jamming: This severe arch forcefully jams the delicate facet joints of the lower spine together, causing sharp, localized pain.
Disc Degeneration: The unnatural angle places extreme compressive force on the posterior aspect of the intervertebral discs, radically increasing the risk of a herniated disc or sciatica.
Primary Source Proof: Kinematic Rehabilitation
Clinical orthopedic research unequivocally demonstrates that targeted strengthening of the lumbo-pelvic-hip complex is vastly superior to passive treatments for resolving chronic, non-specific low back pain.
Download Clinical Efficacy PDF: The Efficacy of Pelvic Biomechanical Correction and Core Stabilization in Chronic Non-Specific Low Back Pain (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for spinal and pelvic rehabilitation.
The Rehab Mechanics Corrective Protocol
Treating an anterior pelvic tilt requires a rigorous, phased approach to rewire your nervous system and release structural handbrakes. We do not just rub the sore muscles; we rebuild your biological foundation.
Phase 1: Releasing the Brakes (Advanced Soft Tissue Release)
Before we can strengthen the weak muscles, we must unlock the tight ones. You cannot strengthen a muscle if its opposing muscle is locked short.
Psoas Release: Our physiotherapists utilize advanced, deep myofascial release techniques to break down fibrotic tissue in the psoas and iliacus muscles deep within the abdomen.
Lumbar Decompression: We utilize manual traction and targeted joint mobilizations to un-jam the compressed facet joints in the lower back, providing immediate relief from the sharp, pinching pain.
Quadriceps Lengthening: Specifically targeting the rectus femoris (the front thigh muscle that attaches to the pelvis), restoring normal length to stop it from pulling the pelvis downward.
Phase 2: Neuromuscular Re-education (Core Activation)
Once the pelvis is free to move, we must teach your brain how to hold it in a neutral position.
Posterior Pelvic Tilting: We guide you through micro-movements to actively tilt the pelvis backward, flattening the severe arch in the lower back.
Transversus Abdominis (TVA) Activation: The TVA is your body's internal weight belt. We use specific breathing drills and biofeedback to train this muscle to fire continuously, acting as a rigid brace for the lumbar spine.
Dead Bug Progressions: A crucial exercise that trains the core to remain completely stable and neutral while the arms and legs are moving.
Phase 3: Structural Fortification (Gluteal Strengthening)
The final phase permanently cements your new posture by building massive strength in the posterior chain.
Isolated Glute Bridges: Forcing the gluteus maximus to contract forcefully while the hip flexors are stretched, reversing the mechanics of Lower Crossed Syndrome.
Heavy Slow Resistance (HSR): We progress to heavy, functional movements like Romanian Deadlifts (RDLs) and kettlebell swings. This proves to your nervous system that your spine and pelvis can safely handle heavy, dynamic loads in the real world.
Ergonomic Integration: We provide strict guidelines for modifying your Toronto workspace, ensuring you do not undo your physical therapy during your 9-to-5 workday.
Restore Your Structural Integrity
Do not accept chronic back pain as a normal consequence of working in an office. By addressing your foundational body mechanics, you can permanently eliminate the hidden forces destroying your lumbar spine.
Book a comprehensive biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.