Splinted again - no rest for the wounded! You will thank yourself later.
Should I Stop Running if I Have Severe Shin Splints?
No. Total rest weakens tissues. Physiotherapy cures shin splints by analyzing your running biomechanics, strengthening your lower leg musculature, and utilizing targeted modalities to heal medial tibial stress syndrome while keeping you safely active.
The Frustration of Medial Tibial Stress Syndrome
For the active residents of Parkdale and Trinity Bellwoods, running is more than just exercise; it is a fundamental part of the Toronto lifestyle. However, one of the most common and devastating injuries that sidelines local runners is "shin splints," medically known as Medial Tibial Stress Syndrome (MTSS).
The typical cycle is incredibly frustrating. You feel a dull, aching pain along the inner edge of your shin bone during your run. You ignore it. It worsens into a sharp, burning sensation that persists even while walking. You finally stop running, ice your shins for a month, and wait for the pain to vanish. But the very first day you return to the pavement, the pain instantly returns.
At Rehab Mechanics, we see this exact cycle weekly. The problem with complete rest is that it does absolutely nothing to address why the shin bone became inflamed in the first place. Resolving MTSS requires a biomechanical approach to foot function and load management.

Structural Analysis: What Causes Shin Splints?
To permanently eliminate shin pain, we must perform a structural analysis of the lower leg's kinetic chain. Shin splints are an overuse injury, but they are driven by specific biomechanical failures.
The Anatomy of MTSS
The pain you feel is the result of excessive pulling forces on the periosteum (the thin layer of tissue covering the bone) of the tibia (shinbone).
The Tibialis Posterior: This muscle runs down the back of your calf, crosses under the inside of your ankle, and attaches to the bottom of your foot. Its primary job is to hold up your foot arch.
The Soleus Muscle: A deep calf muscle responsible for absorbing the massive shock of landing with every stride.
Biomechanical Triggers for MTSS
When these muscles are overwhelmed, they pull violently at their attachment points on the shin bone, causing micro-tearing and extreme inflammation.
Excessive Overpronation
If your foot arch collapses too much when you land (overpronation), the tibialis posterior is violently stretched.
The Whiplash Effect: This rapid stretching creates a "whiplash" effect on the muscle tendon, transferring the shear stress directly into the tibial bone.
Weak Hip Stabilizers
If your gluteus medius (side hip muscle) is weak, your knee will collapse inward (knee valgus) when your foot strikes the ground.
The Kinetic Chain Breakdown
This inward knee collapse forces the tibia to rotate internally, massively increasing the torsional strain on the shin bone and lower leg fascia.
Primary Source Proof: Running Kinematics
Our approach to treating running pathologies rejects passive rest in favor of active, evidence-based rehabilitation protocols.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for running-related rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating MTSS effectively requires a progressive, phased approach. We do not just treat the shin; we rebuild the entire leg.
Phase 1: Acute Load Management and Inflammation Control
We do not prescribe total rest, but we do prescribe relative rest.
Activity Modification: We will temporarily replace pavement running with pain-free cross-training (like cycling or deep-water running) to maintain your cardiovascular fitness while the periosteum heals.
Manual Soft Tissue Release: Using targeted massage and instrument-assisted techniques to release the hypertonic (overly tight) soleus and tibialis posterior muscles, reducing their pull on the bone.
Shockwave Therapy: For chronic, stubborn cases, we may utilize shockwave therapy to stimulate blood flow and cellular repair directly at the tibial attachment site.
Phase 2: Structural Strengthening
This is where the cure happens. We must increase the load capacity of your lower leg.
Intrinsic Foot Strengthening: Exercises like "foot doming" or towel scrunches to rebuild the tiny muscles inside the foot that support the arch.
Heavy Slow Resistance (HSR) Calf Training: Progressing from double-leg to single-leg weighted calf raises, specifically focusing on the bent-knee soleus raise, to build bulletproof lower leg tissue.
Gluteal Activation: Clamshells, lateral band walks, and single-leg deadlifts to stabilize the pelvis and prevent the knee from caving inward during the running stride.
Phase 3: Gait Retraining and Return to Run (RTR)
Before you return to Trinity Bellwoods, we must fix the way you run.
Cadence Modification: Increasing your step rate by just 5% to 10% drastically reduces the impact force on the shin bone with each step.
Orthotics Assessment: If structural flat feet are the root cause, Sanjay is qualified to dispense custom medical orthotics to permanently correct the foot mechanics.
Graded RTR Program: Providing a strict, interval-based running schedule to progressively re-introduce mechanical load to the tibia without triggering a relapse.
Run Without Pain in Parkdale and Queen West
Do not let chronic shin splints ruin your running season. Get a definitive biomechanical assessment and an active rehabilitation plan.
Book an appointment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible from Parkdale, Queen West, and Liberty Village.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.

Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Lat and Pec muscle tightness: fixing chronic issues
Can Physiotherapy Fix Chronic Lat and Pec Muscle Tightness?
Yes. Physiotherapy effectively resolves chronic latissimus dorsi and pectoral tightness. Targeted manual therapy and specific corrective exercises restore proper upper body biomechanics, relieving shoulder impingement, improving posture, and preventing complex rotator cuff injuries.
The Hidden Culprits of Upper Body Pain
When Toronto residents search for solutions to shoulder pain or upper back stiffness, they often focus entirely on the joint itself. However, the true source of chronic upper body dysfunction frequently lies in the massive muscle groups that control the torso and connect to the arms: the latissimus dorsi (lats) and the pectoralis major and minor (pecs).
At Rehab Mechanics, we frequently analyze GSC data showing an increase in local searches for "lat therapy" and "pec" related issues. Whether you are a dedicated weightlifter training in Queen West, an office worker hunched over a desk for ten hours a day, or a tradesperson performing repetitive overhead movements, these two muscle groups are notoriously prone to adaptive shortening.
Understanding how to treat and rehabilitate these muscles is a cornerstone of human biomechanics. We do not just massage the sore spot; we structurally analyze and rebuild your upper body kinetic chain.
Structural Analysis: The Biomechanics of Lats and Pecs
To understand why tight lats and pecs cause such profound mechanical dysfunction, we must perform a deep dive into the anatomical roles these muscles play in the human body.
The Pectoralis Group
Located on the front of your chest, the pec major and minor are powerful internal rotators and flexors of the shoulder joint.
The Postural Impact: When you spend hours looking at a computer screen, your shoulders round forward. This sustained position physically shortens the pectoral fibers.
The Mechanical Consequence: Chronically tight pecs pull the scapula (shoulder blade) forward and downward into an anterior tilt.
The Chain Reaction: This anterior tilt dramatically reduces the subacromial space—the tiny gap where your rotator cuff tendons pass through the shoulder joint.
Subacromial Impingement
When the space is reduced by tight pecs, reaching overhead causes the shoulder bones to pinch the bursa and rotator cuff tendons, leading to sharp, stabbing pain known as impingement syndrome.
The Latissimus Dorsi
The lats are the largest muscles in your upper body, sweeping from your lower spine and pelvis all the way up to attach to the front of your humerus (upper arm bone).
The Anatomical Anchor: Because they attach to both the pelvis and the arm, they are a massive biomechanical bridge.
The Restriction: When the lats become tight from heavy pulling exercises or prolonged sitting, they restrict shoulder flexion.
The Compensatory Movement: If your lats are tight and you try to reach straight up, your arms will physically stop moving at a certain angle. To get your hands overhead, your brain will force your lower back to over-extend (arch aggressively), shifting the stress from the shoulder directly into the lumbar spine.
The "Lat-Shoulder-Spine" Triad
This is why lat tightness is a leading, yet frequently misdiagnosed, cause of lower back pain in athletes and desk workers alike.

Primary Source Proof: Upper Body Kinematics
Our clinical interventions for pec and lat dysfunction are rooted in proven anatomical and biomechanical science.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for postural rehabilitation.
The Rehab Mechanics Treatment Protocol
Resolving lat and pec tightness requires a multi-phased approach that combines aggressive tissue release with targeted neurological re-education.
Phase 1: Advanced Soft Tissue Release
We must manually restore the resting length of the shortened muscle fibers before strengthening the opposing muscles.
Active Release Techniques (ART): Pinning the tight fascial bands of the pec minor while actively moving the patient's arm overhead to sheer apart scar tissue adhesions.
Latissimus Myofascial Mobilization: Deep tissue release along the lateral rib cage and posterior axillary fold to restore scapular upward rotation.
Instrument-Assisted Soft Tissue Mobilization (IASTM): Utilizing specialized tools to break down chronic, dense fibrotic tissue in the muscle bellies.
Phase 2: Restoring Joint Arthrokinematics
Once the muscular "brakes" are released, we address the joint capsules.
Thoracic Spine Extension: Mobilizing the mid-back to ensure the spine can extend properly, taking the load off the lats.
Glenohumeral Mobilization: Gently stretching the posterior capsule of the shoulder joint to restore centralized rotation of the humerus.
Phase 3: Corrective Loading and Neuromuscular Control
This is the most critical phase for long-term resolution. We must strengthen the muscles that directly oppose the lats and pecs.
Scapular Retraction Training: Prescribing exercises like prone T-raises and face-pulls to strengthen the rhomboids and middle trapezius, physically pulling the shoulders back into a neutral alignment.
Lower Trapezius Activation: Utilizing wall slides and Y-raises to train the lower traps to depress the scapula, fighting the upward pull of tight upper traps and lats.
Eccentric Loading: Safely lengthening the lats and pecs under load (e.g., controlled dumbbell pullovers or slow eccentric chest flies) to build tissue capacity at end-range motion.
Integrate Your Care at Prime Medical Centre
If you are dealing with chronic shoulder impingement, a tight back, or poor posture, do not wait for the rotator cuff to tear. Physiotherapy offers a clear, mechanical solution to your biomechanical problem.
Book an upper body biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering comprehensive, interdisciplinary healthcare in the heart of Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.

Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Comprehensive diagnoses: doctor and physio teamwork
Should I See Both a Medical Doctor and a Physiotherapist for Chronic Back Pain?
Yes. Co-managing chronic lower back pain with both a physician and a physiotherapist yields the highest recovery rates. Doctors handle acute pain management and diagnostic imaging, while physiotherapists rebuild spinal stability and correct the mechanical tissue dysfunctions that are actually causing the pain.
The Trap of Siled Healthcare
One of the most frustrating experiences for a patient suffering from chronic lower back pain is bouncing between different healthcare providers who do not communicate with each other. You see your family doctor, who prescribes muscle relaxants. Weeks later, you see a massage therapist who rubs the sore muscles. Eventually, you might try a chiropractor or a physiotherapist.
This fragmented, "siloed" approach to healthcare often leads to repetitive assessments, conflicting advice, and prolonged suffering. Chronic back pain is rarely a simple, one-dimensional problem. It involves neurological pain signaling, mechanical joint dysfunction, and muscular deconditioning.
At Rehab Mechanics, we believe the gold standard for patient care is an integrated, interdisciplinary model. This is exactly why we operate closely alongside the medical doctors inside the Prime Medical Centre on Abell Street. By bridging the gap between medicine and rehabilitation, we drastically streamline your path to recovery.
The Medical vs. Mechanical Pain Models
To understand why both a doctor and a physiotherapist are necessary, you must understand the two distinct angles from which back pain must be attacked: the medical (chemical/neurological) and the mechanical (structural).
The Role of the Medical Doctor
Physicians are the gatekeepers of your systemic health. When you experience severe, acute back pain, their role is critical in the early stages.
Red Flag Screening: Doctors rule out serious, non-musculoskeletal causes of back pain, such as kidney infections, systemic diseases, or severe spinal cord compression.
Diagnostic Imaging: If necessary, physicians can order X-rays, MRIs, or CT scans to identify structural anomalies like severe disc herniations or spinal stenosis.
Pharmacological Management: During acute flare-ups, inflammation and muscle spasms can be so severe that movement is impossible. Doctors can prescribe targeted NSAIDs, muscle relaxants, or neuropathic pain modulators to lower the pain threshold enough for physical rehabilitation to begin.
The Role of the Registered Physiotherapist
While medication alters the way your brain perceives pain, it does not fix the physical tissue. That is the realm of physiotherapy.
The Mechanical Fix
Once the acute pain is chemically managed, the physiotherapist steps in to identify and correct why the spine failed in the first place.
Structural Rehabilitation
Physiotherapists conduct a functional, biomechanical audit. We look for joint stiffness, pelvic asymmetry, weak deep-core stabilizers (transversus abdominis), and poor lifting mechanics. Through manual therapy, targeted joint mobilization, and highly specific corrective exercise, we rebuild the structural integrity of the spine.
Primary Source Proof: Interdisciplinary Efficacy
Extensive clinical literature proves that multidisciplinary biopsychosocial rehabilitation is vastly superior to standard medical care alone for chronic low back pain.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for integrated back pain management.
The Synergy of the Prime Medical Centre
Operating within the Prime Medical Centre on Abell Street in Queen West allows us to provide a seamless, collaborative patient experience. Here is how this structural integration benefits you:
1. Instant Communication
If our physiotherapists identify a neurological "red flag" during a physical assessment (such as sudden numbness in the saddle region or foot drop), we do not have to fax a report and wait two weeks. We can walk down the hall and consult directly with a physician to expedite advanced imaging or specialist referrals.
2. Coordinated Treatment Plans
Your care is not contradictory. If your doctor administers a localized corticosteroid injection to reduce joint inflammation, our physiotherapy team knows exactly when it occurred. We can then perfectly time your progressive loading and core strengthening exercises to maximize the "window of opportunity" provided by the injection.
3. Holistic Patient Care
Chronic pain takes a massive psychological toll. By having your medical management, pharmacological needs, and physical rehabilitation housed under one collaborative roof, your stress and anxiety regarding the logistics of your healthcare are significantly reduced.
Stop Guessing with Your Spine
If you have been relying solely on pain medication or endless passive treatments without seeing long-term improvement, it is time for a comprehensive, interdisciplinary approach.
Rebuild your spine with the combined expertise of medicine and biomechanical physiotherapy. Book an assessment with our clinical team today. We are located right inside the Prime Medical Centre at 68 Abell Street in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials

Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Runner’s knee and the IT Band ‘syndrome’'
Is Physiotherapy Effective for Treating Runner’s Knee and IT Band Syndrome?
Yes. Rest alone rarely cures Runner's Knee or IT Band Syndrome. Physiotherapy provides a permanent solution by correcting faulty hip biomechanics, strengthening weak gluteal muscles, and using manual release techniques to reduce the friction forces causing inflammation on the outside of the knee.
The Plight of the Toronto Runner
From the paths of Trinity Bellwoods to the long stretches of the Martin Goodman Trail, Toronto has a massive, dedicated running community. But as the mileage increases, so do the overuse injuries.
Two of the most frustrating, stubborn conditions that sideline runners are Patellofemoral Pain Syndrome (Runner’s Knee) and Iliotibial (IT) Band Syndrome. These conditions are characterized by a sharp, burning pain either behind the kneecap or on the outer edge of the knee joint.
Many runners try to manage these issues by taking a few weeks off, icing their knees, and stretching their hamstrings. Invariably, the moment they return to their regular mileage, the pain returns immediately. At Rehab Mechanics, we see this cycle constantly. To break it, you have to stop treating the knee and start looking at the mechanics of the hip and foot.
The Biomechanics: Why the Knee is the Victim
In the kinetic chain of the human leg, the knee is a relatively simple hinge joint caught between two highly mobile, complex joints: the hip and the ankle. In almost all cases of running-related knee pain, the knee is not the culprit; it is the victim of poor mechanics above or below it.
Understanding IT Band Syndrome (ITBS)
The Iliotibial band is a thick, fibrous band of fascia that runs down the outside of your thigh, attaching from your pelvis to just below your knee.
The Friction Problem: During running, the IT band repeatedly snaps back and forth over the lateral femoral epicondyle (the bony bump on the outside of the knee).
The Root Cause: The IT band itself does not contract. Its tension is dictated by the muscles it attaches to at the hip—specifically the Tensor Fasciae Latae (TFL) and the Gluteus Maximus. When your deep gluteal stabilizers are weak, your pelvis drops, your knee caves in, and the TFL overworks, pulling the IT band violently tight against the knee bone.
Understanding Runner's Knee (PFPS)
Patellofemoral Pain Syndrome is characterized by an aching pain under or around the kneecap (patella).
The Tracking Issue
The patella is supposed to glide smoothly up and down within a specific groove on the femur (thigh bone) as you bend and straighten your leg.
The Patellar Derailment
If your quadriceps muscles are imbalanced, or if your hip drops causing your femur to rotate inward, the kneecap is pulled out of its groove. It grinds against the underlying bone, wearing away the cartilage and causing deep, throbbing inflammation.
Primary Source Proof: Running Kinematics
Our clinical approach to treating running pathologies is heavily backed by sports science and biomechanical research, moving away from passive treatments towards active strengthening.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for running-related knee rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating these conditions effectively requires a thorough structural analysis and a multi-phased rehabilitation protocol. Here is how we get our Queen West and Parkdale runners back on the pavement:
1. Advanced Soft Tissue Release
You cannot stretch the IT band—it is as strong as a truck tire. However, you can release the muscles attached to it.
Myofascial Release: We use deep manual therapy to release the overactive TFL, vastus lateralis (outer quad), and tight hip flexors.
Joint Mobilization: Ensuring the patella has normal glide and the ankle joint has adequate dorsiflexion.
2. Hip and Core Fortification
This is the core of the cure. We must rebuild the muscular brakes of your lower body.
Gluteus Medius Activation: The Glute Medius is the most important muscle for a runner. It keeps the pelvis level when you are on one leg. We use targeted, isolated exercises (like clamshells and lateral band walks) to "wake it up."
Eccentric Quadriceps Loading: Building the capacity of the quadriceps to absorb the shock of downhill running without irritating the patellar tendon.
3. Gait Retraining and Load Management
Once the tissue is healed and the muscles are activated, we must fix the way you run.
Cadence Manipulation: Often, simply increasing a runner's step rate (cadence) by 5-10% dramatically reduces the impact forces on the knee joint.
Return-to-Run (RTR) Scheduling: We prescribe exact running intervals (combining walking and running) to progressively reload the tendons safely without triggering an inflammatory relapse.
Don't Let Knee Pain End Your Running Season
If you are dealing with sharp knee pain that ruins your runs, stop resting and hoping for a miracle. Physiotherapy offers a clear, mechanical solution to your biomechanical problem.
Book a running assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible from Parkdale, Queen West, and Liberty Village.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Biomechanical assessments and injury prevention
Does a Full Biomechanical Assessment Prevent Future Sports Injuries?
Yes. A comprehensive biomechanical assessment identifies hidden muscular imbalances, joint restrictions, and faulty movement patterns before they cause tissue failure. By mapping your kinematics, physiotherapists implement preventative loading strategies to protect vulnerable ligaments, tendons, and joints from catastrophic injury.
The Flaw in "Wait and See" Healthcare
In the world of sports and active living, the traditional medical model is entirely reactive. You run until your Achilles tendon tears, you lift until your lower back spasms, or you play tennis until your elbow burns. Then, and only then, do you seek treatment.
At Rehab Mechanics in Toronto, we fundamentally disagree with this approach. Injuries rarely happen out of nowhere. They are almost always the final result of thousands of subtle, faulty, repetitive movements. A ligament finally snaps not because of one bad step, but because a stiff ankle and a weak hip forced that ligament to absorb loads it was never designed to handle for months prior.
If you are serious about your physical longevity—whether you are a marathon runner, a CrossFit athlete, or simply someone who wants to play with their kids without pain—a clinical biomechanical assessment is the most important investment you can make in your body.
What is Biomechanics?
Biomechanics is the study of the structure, function, and motion of the mechanical aspects of biological systems. In physiotherapy, it means analyzing the human body as a complex machine of levers (bones), pulleys (tendons), and motors (muscles).
The Kinetic Chain Concept
Your body does not operate as a series of isolated parts; it operates as a deeply connected "kinetic chain."
Interdependence: A problem in your foot will inevitably dictate how your knee moves. A stiff mid-back will force your shoulder to overcompensate.
The Path of Least Resistance: The nervous system is incredibly smart. If a primary muscle is weak, the brain will instantly recruit secondary muscles to get the job done. This is called a "compensatory pattern."
The Cost of Compensation: While compensations keep you moving in the short term, they overload secondary tissues, leading to inevitable breakdown and chronic pain.
Ground Reaction Forces
Every time your foot strikes the ground, energy travels up your leg. A biomechanical assessment analyzes how efficiently your body absorbs and dissipates these ground reaction forces.
Faulty Shock Absorption
If you overpronate (foot arch collapses) severely, your tibia rotates inward, placing massive torsional shear stress on the meniscus and ACL in the knee. The knee pain is just the symptom; the foot mechanics are the root cause.
Primary Source Proof: Preventative Kinematics
Our preventative screening protocols are rooted in advanced kinematic research and sports medicine data.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for biomechanical screening and injury prevention.
Inside a Rehab Mechanics Biomechanical Assessment
When you book a biomechanical assessment at our Queen West clinic, we conduct a top-to-bottom structural audit. Here is the structural analysis of our process:
1. Static Postural Mapping
Before you even move, your resting posture tells a story. We look for:
Leg length discrepancies.
Pelvic tilts (anterior or posterior) that alter spinal mechanics.
Scapular winging or forward head posture.
2. Joint Range of Motion (ROM) Testing
We isolate every major joint to ensure it has the requisite mobility to perform safely.
Ankle Dorsiflexion: Crucial for squatting and running down stairs. A lack of ankle mobility is a primary driver of knee pain and plantar fasciitis.
Hip Internal/External Rotation: A stiff hip forces the lower back to twist excessively during sports like golf or tennis.
Thoracic Spine Extension: Necessary for overhead lifting and shoulder health.
3. Functional Movement Screening
This is the dynamic portion of the exam. We watch how your nervous system coordinates complex movements.
Overhead Squat Analysis: Reveals tightness in the lats, weakness in the core, and mobility restrictions in the hips and ankles simultaneously.
Single-Leg Loading: Squatting on one leg instantly highlights gluteal weakness (indicated by the knee caving inward, known as knee valgus).
Gait and Running Analysis: We evaluate your strike pattern, cadence, and pelvic drop to identify inefficiencies in your stride.
4. Custom Orthotics and Modalities
If your assessment reveals structural foot abnormalities that cannot be corrected by exercise alone (such as rigid flat feet or severe overpronation), Sanjay is licensed to dispense custom-molded orthotics. These devices alter the biomechanical angles of the foot, instantly changing the kinetic chain all the way up to the spine.
Stop Waiting for the Injury to Happen
Don't wait until you are sidelined from your favorite activities to address your body's mechanics. Identify the weak links in your kinetic chain now, and build a more resilient, efficient body.
Book a comprehensive biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Physio and tech neck
Can Physiotherapy Actually Fix "Tech Neck" and Chronic Desk Posture Pain?
Yes. Physiotherapy effectively resolves "tech neck" and postural pain by addressing the biomechanical root causes. Through targeted manual therapy, cervical joint mobilization, and specific deep neck flexor strengthening, physiotherapy reverses the tissue adaptations caused by prolonged sitting and screen time.
The Liberty Village and Queen West Epidemic
The Queen West and Liberty Village neighborhoods are hubs for Toronto's tech professionals, creatives, and remote workers. While the lifestyle is vibrant, the physical toll of sitting at a laptop for 8 to 10 hours a day is severe.
We see hundreds of local residents walking into Rehab Mechanics suffering from the exact same symptom profile: chronic tension at the base of the skull, burning pain between the shoulder blades, and a nagging stiffness that simply won't release with basic stretching or massage.
This condition, colloquially known as "Tech Neck," is not just muscle tightness. It is a fundamental, biomechanical adaptation to sustained poor posture. If left untreated, it leads to premature spinal degeneration, tension headaches, and chronic nerve irritation.
The Biomechanics of "Upper Crossed Syndrome"
To understand why simple stretching doesn't cure desk pain, we have to look at the structural changes happening in your upper body. Medical professionals refer to this specific postural deviation as "Upper Crossed Syndrome."
The Pattern of Muscle Imbalance
When you lean forward to look at a screen, a predictable cross-pattern of muscle tightness and weakness develops:
The Tight Muscles: Your pectoral (chest) muscles and upper trapezius/levator scapulae (neck) become chronically shortened and hyperactive.
The Weak Muscles: Your deep cervical flexors (the small muscles in the front of your neck) and your lower/middle trapezius and rhomboids (mid-back) become elongated, weak, and inhibited.
The Physics of a Forward Head
For every inch your head moves forward out of neutral alignment, the functional weight of your head on your cervical spine doubles.
The Strain on the Cervical Spine
A human head weighs roughly 10-12 pounds. If your head shifts forward by just two inches while looking at your monitor, the musculature of your upper back and neck has to contract continuously to hold up 30-32 pounds of force.
Joint Compression and Disc Stress
This sustained isometric contraction inevitably leads to failure. The neck muscles develop dense myofascial trigger points (knots), and the excessive downward pressure begins to compress the delicate cervical discs and facet joints, eventually leading to early-onset osteoarthritis and pinched nerves.
Primary Source Proof: Postural Biomechanics
Our clinical interventions are based on proven anatomical and biomechanical science, not temporary fads. We focus on structural correction.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for postural rehabilitation.
The Rehab Mechanics Solution: Structural Analysis
Treating Tech Neck requires a multi-pronged approach. You cannot simply rub the sore muscles and expect long-term relief; you must correct the underlying imbalance.
1. Advanced Manual Soft Tissue Therapy
Before we can strengthen the weak muscles, we must release the structural brakes.
Myofascial Release: We use targeted manual techniques to break down the dense, fibrotic tissue in the pectorals and upper trapezius.
Trigger Point Therapy: Deactivating the hypersensitive nodules in the neck muscles that refer pain up into the head (causing tension headaches).
Joint Mobilization: Gently mobilizing the stiff thoracic (mid-back) and cervical (neck) spinal segments to restore proper rotation and extension.
2. Corrective Exercise Prescription
This is where the permanent fix happens. We must re-educate your nervous system to hold your skeleton correctly.
Deep Cervical Flexor Activation: Micro-movements (like chin tucks) that wake up the dormant stabilizing muscles in the front of the neck.
Scapular Retraction Training: Strengthening the rhomboids and lower traps to pull the shoulder blades back and down, taking the load off the neck.
Thoracic Extension Drills: Reversing the "C-curve" of the mid-back using foam rollers and targeted mobility exercises.
3. Ergonomic Optimization
You cannot out-rehab 40 hours a week of terrible posture. We provide practical, actionable advice on setting up your home or office workstation.
Monitor Height: Ensuring the top third of your screen is at eye level.
Arm Support: Ensuring your elbows rest comfortably at 90 degrees to offload the trapezius muscles.
Micro-Breaks: Implementing strategies for regular postural resets throughout the work day.
Reclaim Your Comfort and Focus
Do not accept chronic neck and shoulder pain as a normal part of your career. It is a mechanical problem with a mechanical solution.
If you live or work in the Queen West or Liberty Village area, take the first step toward a pain-free workday. Book a comprehensive postural assessment with our team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Physio and car accidents
Should I Start Physiotherapy Right Away After an Ontario Car Accident?
Yes. Early physiotherapy intervention after a motor vehicle accident (MVA) prevents acute whiplash from becoming a chronic pain condition. Immediate treatment accelerates tissue repair, reduces scar tissue, and ensures seamless navigation of Ontario’s statutory accident benefits schedule.
The Hidden Danger of Auto Collision Injuries
Motor vehicle accidents, even those at low speeds in downtown Toronto traffic, transfer immense kinetic energy into the human body. Because the adrenaline response masks immediate pain, many people walk away from a crash feeling "fine," only to experience crippling stiffness, headaches, and radiating pain 48 to 72 hours later.
At Rehab Mechanics, we frequently see patients who delayed seeking treatment for weeks, hoping the pain would simply fade. Unfortunately, delaying care often leads to abnormal scar tissue formation, chronic joint restriction, and prolonged suffering.
Our clinic, located at 68 Abell Street, specializes in complex MVA rehabilitation, seamlessly guiding patients through both their physical recovery and the complex Ontario insurance paperwork.
Understanding the Biomechanics of Whiplash
Whiplash Associated Disorders (WAD) are the most common injuries sustained in a rear-end collision. Understanding the mechanics of the injury explains why early intervention is critical.
The Kinematic Sequence of a Crash
When your vehicle is struck, your body undergoes a rapid, unnatural sequence of movements:
Phase 1: The S-Curve: Your lower spine is pushed forward by the seat, but your head remains momentarily stationary. This forces the neck into an unnatural "S" shape, shearing the lower cervical discs.
Phase 2: Hyperextension: The head violently whips backward over the headrest, tearing anterior neck ligaments and muscles (like the longus colli).
Phase 3: Hyperflexion: The head is thrown violently forward, straining the posterior neck muscles, the upper trapezius, and the delicate facet joints of the spine.
Micro-Tearing and the Inflammatory Cascade
This rapid sequence causes microscopic tearing in the muscle fibers, ligaments, and fascia.
The body responds immediately by flooding the area with inflammatory fluids.
While inflammation is a natural part of healing, excessive inflammation in the tight spaces of the cervical spine causes nerve compression and severe pain.
Without early physiotherapy, the body repairs these micro-tears with disorganized, rigid scar tissue.
Primary Source Proof: MVA Clinical Guidelines
Our approach to auto injury rehabilitation is strictly governed by peer-reviewed research and provincial regulatory guidelines. We do not guess with your recovery.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for musculoskeletal treatments following motor vehicle accidents.
Our MVA Treatment Protocol: A Structural Analysis
Navigating recovery after an accident requires a phased, progressive approach. We do not simply apply heat packs and send you home. We rebuild your structural integrity.
Phase 1: Acute Pain & Inflammation Management (Weeks 1-3)
The immediate goal is to calm the nervous system and control the inflammatory cascade without completely immobilizing the joints.
Gentle Range of Motion (ROM): Safe, guided movements to prevent joint capsules from freezing.
Pain-Relief Modalities: Application of clinical-grade modalities (like TENS or specific interferential currents) to block pain signals.
Soft Tissue Mobilization: Extremely light manual therapy to encourage lymphatic drainage and reduce swelling in the deep neck muscles.
Phase 2: Restoring Biomechanical Function (Weeks 4-8)
Once the acute pain subsides, we focus on breaking down fibrotic scar tissue and restoring normal joint mechanics.
Targeted Joint Mobilizations: Restoring the natural glide of the spinal facet joints.
Deep Tissue Release: Addressing the trigger points that have developed in the trapezius, levator scapulae, and suboccipital muscles.
Motor Control Re-training: Teaching the brain how to recruit the deep neck flexors properly, rather than relying on the over-strained superficial muscles.
Phase 3: Strengthening and Work Hardening (Weeks 8+)
The final phase ensures that your body is strong enough to handle the demands of your daily life and job without relapsing.
Progressive Loading: Introducing resistance bands and light weights to rebuild muscular endurance.
Postural Endurance Training: Ensuring the spine can maintain alignment during prolonged sitting or standing.
Functional Simulation: Replicating the physical demands of your specific occupation to ensure a safe, confident return to work.
Navigating the Ontario Insurance Maze
One of the most stressful aspects of a car accident is dealing with insurance companies. The Ontario auto insurance system (regulated by FSRA) is notoriously complex.
How Rehab Mechanics Helps
We handle the administrative burden so you can focus entirely on your physical recovery.
Direct Billing: We bill auto insurers directly through the Health Claims for Auto Insurance (HCAI) portal.
Treatment Plans (OCF-18): We draft and submit comprehensive, medically sound treatment plans to your adjuster to ensure your care is fully funded.
Interdisciplinary Coordination: Operating within the Prime Medical Centre, we collaborate directly with medical doctors to ensure your injuries are thoroughly documented from day one.
Don't Let an Accident Dictate Your Future
The first 14 days following a motor vehicle collision are the most critical window for determining your long-term recovery trajectory. Ignoring the stiffness today can lead to chronic spinal degeneration tomorrow.
Take control of your recovery. Book a comprehensive MVA assessment with our team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible by the Queen streetcar.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Cracking the Back Pain Myth
Will core muscles (intercostal and abdominal) alleviate back pain?
YES. Absolutely!
Many people assume that a rock-solid core automatically negates back pain, but this notion is too simplistic. While strengthening your abs can support overall stability, back pain is a multifaceted issue that involves muscles, ligaments, and even joint alignment. This section delves into the common misconception and sets the stage for exploring practical strategies that go beyond just crunches or planks.
Understanding the root causes of back pain involves dissecting several factors:
Muscular Imbalance: Overemphasis on abdominal exercises can neglect other crucial muscle groups.
Postural Misalignment: Chronic habits, both at work and during exercise, contribute to discomfort.
Lack of Flexibility: Not incorporating adequate stretching exercises may limit range of motion and exacerbate strain.
In community centers and local gyms, trainers are increasingly emphasizing balanced routines that blend strengthening with targeted stretching and mobility work. As you read on, you’ll discover actionable tips and step-by-step guidance on refining your approach to alleviating back pain safely. Prepare to challenge a common myth while learning to safeguard your body against persistent discomfort through a well-rounded, holistic strategy.
Strength Beyond the Abs: Unlocking True Back Relief
It’s time to debunk the idea that strong abs alone can cure back pain. While a robust set of abdominal muscles can enhance core strength, they are merely one piece of the puzzle. Effective relief comes from combining proper posture, balanced muscle engagement, and dynamic stretching exercises to support overall core stability. The spine depends on coordinated efforts from surrounding muscles—back, obliques, and even lower body—to reduce strain and maintain alignment.
Consider these key strategies:
Posture Correction: Adopt ergonomic practices during daily activities to lessen spinal pressure.
Integrated Core Workouts: Strengthen multiple core areas, not just the abs, for better back support.
Regular Stretching: Incorporate stretching exercises into your routine to promote flexibility and alleviate tension.
Practical actions include performing exercises that target both stability and mobility, while being mindful of posture at work or home. By focusing on a holistic approach, residents can enjoy long-term back health and reduced pain. Embrace this comprehensive plan to move beyond the myth and achieve effective, lasting relief.
Uncover the Full Spectrum of Core Strength
Dealing with back pain requires more than just a focus on the abs. A holistic core strategy considers all supporting muscles, promoting a balanced alignment that can ease discomfort and enhance mobility. When you address the issue comprehensively, you’re not just targeting pain—you’re empowering your body for long-term strength and stability.
Rather than isolating the abs, incorporate exercises that activate the obliques, lower back, and deep stabilizers. This balanced approach helps distribute loads evenly, reducing strain on any one area. Consider these practical tips:
Integrated Movements: Engage in compound exercises like planks or bird-dogs that work multiple core muscles simultaneously.
Lifestyle Adjustments: Incorporate routine movement breaks during long hours of sitting to alleviate tension.
Local Wellness Practices: Explore community-based fitness classes that emphasize core stability and overall flexibility.
Taking steps towards a comprehensive core-strengthening routine not only targets back pain but also fosters improved posture and functional fitness. Embrace this multidimensional approach to transform everyday movements into opportunities for a healthier, more resilient body.
Build a Resilient Core and Healthy Back: A Step-by-Step Guide
For those determined to bust the myth that chiseled abs alone solve back pain, a comprehensive approach to core and back strength is essential. Follow these steps for an effective routine:
Begin with a warm-up: Engage in 5 minutes of light cardio and dynamic stretching to increase circulation and loosen up the muscles. Tip: Focus on movements like arm circles and leg swings to prepare your body.
Activate your core: Start with exercises such as planks and side planks that promote deep abdominal stability. Tip: Maintain proper alignment to protect your lower back.
Strengthen your back: Incorporate back extension movements and bridges to target the lumbar muscles. Tip: Ensure slow, controlled movements and avoid overexertion.
Enhance mobility: Conclude your routine with stretching exercises focused on the back and hips, which relieve tension and improve flexibility. Tip: Gentle yoga poses, like child’s pose, can help balance core strength and back health.
This step-by-step guide not only improves overall core resilience but also helps alleviate chronic back discomfort—ideal for anyone seeking to improve their posture and functional movement, whether you’re at home or in local fitness centers.
Frequently Asked Questions: Busting Core Strength Myths
Q1: Why might focused ab exercises not fully address back pain? Traditional ab exercises target superficial muscles and often neglect deeper stabilizers that support the spine. A comprehensive approach includes strengthening the entire core—incorporating obliques, lower back muscles, and pelvic stabilizers—to truly relieve and prevent back discomfort.
Q2: How does overall core strength improve back stability? A balanced core routine provides essential support to the spine, enhancing posture and reducing undue stress on back muscles. This holistic approach minimizes imbalances that can lead to chronic pain, allowing for more effective movement and injury prevention.
Q3: Can stretching exercises contribute to back pain relief? Absolutely. Incorporating controlled stretching routines, both dynamic and static, helps maintain flexibility and ease muscle tension. This approach supports the natural function of the core and back, especially in active local training centers.
Q4: What role do stabilization exercises play in a safe regimen? Stabilization exercises help strengthen both deep and superficial core muscles. They offer structured support to the spine, reduce injury risk, and enhance overall mobility.
Q5: How should a balanced core program be structured? Consider integrating:
Dynamic warm-ups
Targeted stabilization drills
Controlled stretching routines This comprehensive plan promotes functional support and effective pain management.
Bringing It All Together: Redefine Your Approach to Core Strength
As we wrap up our discussion, it’s clear that focusing on core strength is about more than just targeting back pain—it’s about cultivating overall health and resilience. Understanding that a strong core improves balance, stability, and functional movement is key to long-term wellbeing. Even if many assume that crunches alone can resolve back pain, a comprehensive approach that includes proper stretching, mobility exercises, and strength training is essential.
Key takeaways include:
Holistic Core Development: Build a robust foundation that supports your entire body.
Practical Integration: Incorporate stretching exercises and targeted strength training into your routine.
Actionable Next Steps: Evaluate your current fitness regimen, identify gaps, and create a balanced workout plan that includes core, flexibility, and stability work.
Remember, enhancing core strength isn’t an overnight process; it’s a consistent effort that pays off with improved movement and reduced injury risk. Empower yourself by adopting a well-rounded approach that goes beyond simple solutions. Stay motivated, keep progressing, and make sure your routine aligns with your long-term fitness goals.
Author Biography Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our clinical team here.
The Hidden Connection between grip strength and cardio
Uncover the Hidden Connection
Imagine if the strength of your grip could say more about your cardiovascular health than you ever thought possible. Recent insights suggest that the force behind your hand clench might reflect underlying factors that influence your heart’s performance. In this exploration, we dive into how grip strength serves as a window into broader health dynamics, offering clues that extend well beyond muscular endurance.
Many enthusiasts and health professionals now consider grip strength as a straightforward yet powerful indicator of overall wellness. As you read on, you’ll learn how a firm handshake relates to improved blood circulation and enhanced heart function. This section outlines key areas, including:
Simple self-assessments: How you can test your grip to gauge your health.
Daily practices: Easy exercises to improve hand and overall fitness.
Regional health insights: Emphasizing community-based fitness tips that resonate on a local level.
By connecting the dots between physical strength and cardiovascular well-being, this discussion sets the stage for practical strategies to monitor and potentially enhance your heart health, inspiring a proactive approach to everyday fitness.
Unlocking Insights Through Grip Strength
Measuring grip strength offers more than a glimpse into arm power—it provides valuable insight into overall cardiovascular health. Typically, a dynamometer is used to assess hand force, offering a simple yet effective metric for physical strength. Clinicians often consider grip strength as a potential biomarker for heart performance, as a stronger grip may reflect better muscle quality and improved circulation.
Understanding why grip strength matters for heart health involves examining key biological mechanisms. For example, robust hand muscles can indicate healthy muscle mass distribution, which supports proper blood flow dynamics. Additionally, adequate strength in the hands may be associated with balanced inflammatory responses in the body, further contributing to cardiovascular efficiency.
Key factors to consider include:
Muscle Quality: Healthier muscle tissue supports sustained circulation.
Circulatory Function: A strong grip may indirectly indicate efficient heart performance.
Screening Simplicity: Quick and non-invasive, grip strength tests serve as an accessible screening tool.
Local health practitioners in community centers often rely on these measurements as a first step in evaluating long-term heart health. Integrating regular grip strength assessments into wellness routines provides actionable insights for maintaining both muscular and cardiovascular vitality.
Unmasking the Connection: How Hand Strength Reflects Cardiovascular Health
Emerging data indicates that grip strength may serve as a subtle indicator of heart health. Researchers have observed a notable association between a firm grip and lower blood pressure readings, suggesting that stronger hand muscles could be linked to better vascular function. This area of study highlights how simple, everyday tests can offer insights into more complex cardiovascular markers.
Key observations include:
A robust grip is often correlated with enhanced overall muscle tone, which may improve blood circulation.
Regular assessments of grip strength can potentially help in early identification of elevated heart disease risk.
Innovative methodologies in local health centers demonstrate that routine grip exercises might support cardiovascular well-being.
For those interested in proactive wellness measures, incorporating hand-strengthening routines into regular exercise may not only enhance your physical performance but also contribute to maintaining healthy blood pressure levels. As you explore this emerging field, consider practical strategies such as resistance training and ergonomic practices in daily activities to support both muscle strength and heart health. Embrace these insights to foster a more holistic approach to wellness in your community.
Elevate Your Grip and Heart Health: A Step-by-Step Guide
Strengthening your grip is more than just a fitness milestone—it can have far-reaching benefits for overall heart health. Embrace these practical steps to enhance your grip, improve circulation, and support daily wellness.
Warm Up Properly: Begin with 5 to 10 minutes of light cardio, such as brisk walking or jumping jacks, to boost blood flow. Tip: Focus on loosen-up routines that gently activate your muscles.
Incorporate Grip-Focused Exercises:
Squeeze stress balls or therapy putty for 2 sets of 15 reps.
Use hand grippers, progressing in resistance over time. Tip: Start slow and increase intensity gradually to avoid strain.
Combine with Upper Body Workouts: Engage in exercises like push-ups and rows that enhance both grip and overall strength. Tip: Maintain proper form to maximize benefits.
Mind Your Posture and Breathing: Keeping an upright posture during exercises improves circulation and supports cardiovascular health. Tip: Practice deep, controlled breaths to complement your efforts.
Implement these actionable steps regularly to build not just a stronger grip, but a healthier heart.
Common Questions About Grip Strength and Heart Health
Q1: How does grip strength relate to overall heart health? Grip strength is more than just a measure of hand power—it can serve as an indicator of cardiovascular wellness. A strong grip often mirrors muscle integrity and circulatory health, factors that are linked to overall cardiovascular function.
Q2: Why is grip strength considered a useful screening tool? Evaluating grip strength can offer valuable insights into muscle endurance and vascular condition. It is used as a simple, non-invasive method that may help identify early signs of heart-related issues across various age groups, including communities in local health centers.
Q3: Can improving grip strength lead to better heart health? While direct causation is complex, enhanced grip strength through resistance training is often part of an overall fitness program that benefits both muscular and cardiovascular systems, promoting balanced physical health.
Q4: What practical exercises can boost grip strength safely? Incorporate exercises such as hand squeezes, farmer’s walks, and light kettlebell workouts. These routines can be adjusted to suit localized fitness programs and community wellness initiatives.
Q5: How should I monitor progress in grip strength training? Regular assessments using standardized grip dynamometers at local gyms or clinics can help track improvements and support a proactive approach to your heart health.
Revitalize Your Heart Health with Grip Strength Monitoring
As we wrap up our discussion, it’s clear that tracking grip strength is more than just a measure of hand power—it’s an insightful indicator of overall cardiovascular well-being. Integrating regular grip strength tests into your health routine can reveal subtle changes in muscle function and help you gauge your heart health over time.
Understanding that a strong grip often reflects robust circulatory and muscular systems, consider taking these actionable steps:
Monitor your grip strength periodically using standardized tools.
Incorporate strength training and mobility exercises focused on your upper body.
Consult healthcare professionals in your local area to discuss your results and learn tailored strategies.
By keeping a close eye on grip strength, you can better recognize early signs of decline and adjust your exercise routine or lifestyle accordingly. This holistic approach not only improves cardiovascular endurance but also enhances overall physical resilience. Stay proactive about your well-being; each small effort contributes to a healthier, more active future. Keep pushing forward, and let your grip strength be a gateway to maintaining a vibrant heart and body.
Author Biography Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our clinical team here.
Stable Pelvic Floor - your foundation!
Build a Strong Foundation for Athletic Performance
When heavy lifts challenge your limits, a stable pelvic floor is essential to maintaining control and preventing unexpected leaks. As an athlete, you need more than raw strength—balanced core support and pelvic health are vital for peak performance. In this section, learn why nurturing the muscles that support your bladder and lower back matters, especially when the pressure ramps up during intense workouts.
Consider these key points:
Stability in Motion: A conditioned pelvic floor offers better support during lifts, reducing the risk of leakage.
Performance Edge: Proper engagement helps maintain proper alignment and reduces injury risk.
Every Athlete's Concern: From local gym enthusiasts to competitive lifters, pelvic floor awareness is a game changer.
By focusing on this often-overlooked muscle group, you not only enhance your lifting capability but also safeguard your long-term health. Expect insights on practical exercises, daily routines, and tips for integrating pelvic floor training seamlessly into your regimen. As you move forward, discover how small adjustments can lead to remarkable improvements in both confidence and performance in your local training community.
Empower Your Athletic Performance with Pelvic Floor Strength
The pelvic floor may seem hidden, but its impact on athletic performance is profound. A strong pelvic floor not only supports core stability but also enhances overall physical resilience during intense workouts. Understanding the physiological role of these muscles can lead to significant improvements in training outcomes and daily activities.
A well-conditioned pelvic floor contributes to:
Enhanced Core Engagement: The connection between deep abdominal muscles and the pelvic floor creates a supportive framework that stabilizes the lower back during lifts.
Improved Posture and Balance: Strength in this area helps maintain proper alignment, reducing the risk of injuries.
Controlled Breathing: Integrated pelvic floor exercises can promote better respiratory control, essential for sustaining peak performance.
For athletes and fitness enthusiasts in your local community, incorporating targeted pelvic floor exercises into your routine can lead to tangible benefits. Regular practice not only minimizes leaks during exertion but also promotes a more robust structure for power generation. Embrace a comprehensive workout that includes these lesser-known yet vital muscles, and experience the enhanced control and stability that can transform your training sessions.
Uncovering the Root Causes
When tackling challenges like unexpected urinary leakage during intense lifting sessions, it’s essential to understand the underlying biomechanical factors. Muscle imbalances and improper bracing techniques often play significant roles. Many gym-goers notice leaks when certain stabilizing muscles, particularly those comprising the pelvic floor, are not firing correctly during heavy lifts.
Improper bracing may occur when the core muscles, including the diaphragm, spine stabilizers, and pelvic floor, do not work in harmony. This misalignment can lead to reduced intra-abdominal pressure, compromising both core stability and control. A few contributing factors include:
Muscle Imbalances: Overdeveloped superficial muscles might overshadow deeper, stabilizing ones.
Faulty Breathing Techniques: Inadequate diaphragmatic breathing can reduce the effectiveness of bracing.
Lack of Targeted Training: Routine workouts may neglect pelvic floor conditioning, leaving these essential muscles under-trained.
For those in local communities or urban fitness centers, integrating pelvic floor exercises and proper core bracing routines into your fitness regimen can prove beneficial. Emphasizing coordination between core muscles and improving technique during lifts may significantly reduce leakage incidents, allowing you to maintain strength and confidence throughout your workouts.
Strengthen Your Core: Step-by-Step Pelvic Floor Activation
Elevate your athletic performance with a systematic approach to pelvic floor strengthening. Follow these clear and progressive steps to minimize leakage and boost stability during every lift.
Warm-Up and Activation: Begin with light cardio and dynamic stretches to increase blood flow. Focus on engaging the lower core and pelvic region with gentle hip rotations for about 5 minutes. Tip: Keep movements controlled to gradually prepare your pelvic muscles.
Focused Contraction Drills: Practice pelvic floor contractions by tightening the muscles you would use to stop urine flow. Hold each contraction for 5-10 seconds, followed by an equal rest period. Tip: Maintain steady breathing and avoid tensing your abdomen or thighs.
Progressive Resistance Integration: Incorporate exercises like kegels or bridges to add resistance. Aim for 2-3 sets of 10-15 repetitions, adjusting intensity based on comfort. Tip: Consistency is key. Perform these exercises 3-4 times per week for noticeable improvements.
Combine with Core Stability: Integrate pelvic floor work with planks or gentle weight-bearing lifts. This dual approach reinforces core integrity and enhances overall stability. Tip: Practice in local community gyms where guidance on technique is available.
Implement these steps regularly to maintain control during lifts and support long-term core strength.
FAQ: Busting Pelvic Floor Myths for Athletes
What causes pelvic floor leaks during heavy lifts? During intense weightlifting, excessive intra-abdominal pressure can overload weakened pelvic floor muscles, leading to unexpected leaks. Understanding the mechanics behind these events is crucial for effective prevention.
Are pelvic floor issues common in athletic populations? Yes, many athletes experience pelvic floor strain due to repetitive heavy lifting and high-impact activities. Recognizing early signs allows for targeted interventions that help maintain athletic performance without discomfort.
Can dedicated pelvic floor training improve athletic performance? Absolutely. Strengthening pelvic muscles not only reduces leakage risks but also enhances core stability. Incorporating precise exercise routines can create a robust support system, complementing overall training regimens.
What practical exercises support pelvic floor strength? Exercises such as targeted Kegels, functional movements that mimic sports activities, and programmed resistive routines offer practical benefits. Consistent practice often translates to improved control and performance.
How frequently should athletes perform pelvic floor exercises? Integrating these exercises into a daily or weekly routine can yield noticeable results. A balanced regimen helps ensure lasting muscle endurance and minimizes performance setbacks during training sessions on a local scale.
Concluding Insights: Building Strength from the Core
Understanding your pelvic floor is key to unlocking better athletic performance and overall well-being. When you maintain a strong foundation, you not only enhance your stability during heavy lifts but also protect your body from potential injuries. A healthy pelvic floor contributes to improved posture, balance, and functional movement patterns—crucial elements for anyone pursuing an active lifestyle.
Here are actionable next steps to keep your pelvic floor in top shape:
Educate Yourself: Learn about the anatomy and function of your pelvic region.
Incorporate Targeted Exercises: Add pelvic floor strengthening routines into your workout regimen.
Monitor Your Progress: Regularly assess your stability and core strength to notice improvements over time.
Stay Consistent: Make these practices a regular part of your fitness routine.
By integrating these steps, you’ll build a robust core that supports not only your lifts but daily movements as well. Remember, every small, consistent effort contributes to a stronger, healthier body. Stay proactive and engaged in your wellness journey, and empower yourself to lift confidently—no leaks, no limits.
Author Biography Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our clinical team here.
Stamina: key to physical health and longevity
Unlock Endurance & Rejuvenation
Zone 2 training is a game-changer for those looking to enhance physical recovery and boost overall stamina through slow-paced cardio. This training method emphasizes maintaining a steady, moderate heart rate, which improves cardiovascular efficiency while allowing your body to repair muscles and reduce inflammation. As you integrate Zone 2 workouts into your routine, you’ll notice increased fat oxidation and a smoother recovery process after strenuous activities.
In this section, you’ll uncover why consistent, low-intensity cardio is ideal for long-term recovery. Some key benefits include:
Enhanced Aerobic Capacity: Sustained exercise at this intensity strengthens your heart and increases lung capacity.
Effective Fat Burning: Promotes energy usage from fat stores, beneficial for weight management and fueling extended exercise sessions.
Optimized Recovery: By avoiding excessive strain, your muscles and joints have the opportunity to heal and rebuild.
Whether you’re training for endurance events or simply looking to improve your recovery after workouts, Zone 2 training offers practical, science-backed benefits. Prepare to delve into actionable tips on maximizing recovery while embracing a balanced approach to fitness, tailored to help you achieve peak performance in your local community.
Unlocking Cellular Recovery with Zone 2 Cardio
Zone 2 training isn’t just another fitness trend—it’s a transformative approach that taps into your body’s natural regenerative processes. At a moderate, sustainable intensity, this form of cardio targets aerobic metabolism, enhancing mitochondrial efficiency and overall cellular recovery. As you maintain a steady heart rate, your muscles receive the optimal oxygen supply needed to promote effective waste removal and energy production.
Key benefits include:
Enhanced Mitochondrial Function: Zone 2 cardio optimizes energy conversion at the cellular level.
Improved Blood Flow: A consistent rhythm boosts circulation, ensuring nutrients reach tired tissues.
Efficient Recovery: The controlled intensity minimizes muscle breakdown while stimulating repair processes.
For those looking to integrate this training into their routine, consider these steps:
Begin with a light warm-up to prepare your muscles.
Maintain a consistent pace where conversation remains comfortable.
Gradually extend the duration of your workout to build endurance without overexertion.
This balanced approach not only accelerates recovery but also builds a robust foundation for overall cardiovascular health. Embrace Zone 2 training to experience a natural boost in recovery and sustainable fitness improvements.
Empower Your Recovery and Endurance with Moderate Cardio
Zone 2 training stands out as a powerful tool for boosting recovery and building endurance across various athletic pursuits. Operating at a sustainable intensity, this steady state cardio method not only enhances fat oxidation but also promotes efficient energy utilization, setting the stage for balanced training and optimal recovery. By working primarily in this aerobic zone, athletes and fitness enthusiasts enjoy prolonged periods of exercise without excessive strain, making it easier to bounce back between workouts.
Key benefits include:
Enhanced cardiovascular fitness: Strengthening the heart and improving oxygen circulation.
Efficient recovery: Reducing muscle fatigue and lowering the risk of overtraining.
Sustained endurance: Gradually building up stamina for longer or more intense sessions.
Balanced training load: Offering a manageable intensity level ideal for routine workouts.
Integrating Zone 2 training into your regimen supports both physical and mental well-being. Whether you are training for competitions or aiming to elevate everyday fitness, adopting this approach can lead to smoother recovery cycles and reliable performance gains. Experience the advantages in local training groups or community gyms where this method is recognized for its practical and long-lasting impact.
How to Seamlessly Integrate Zone 2 Cardio into Your Recovery Routine
Getting started with Zone 2 training can transform the way you recover while boosting overall endurance. Follow these clear steps to integrate this effective cardio method into your weekly routine:
Assess Your Current Conditioning Begin by evaluating your fitness level and determine your resting heart rate. This establishes a baseline for identifying your optimal Zone 2 range. Tip: Use a heart rate monitor to track progress more accurately.
Warm Up Gradually Complete a 5-10 minute warm-up using dynamic stretches or light jogging. This prepares your cardiovascular system for prolonged steady-state exercise.
Establish Your Zone 2 Range Calculate your Zone 2 target heart rate based on your maximum and resting rates. Aim to keep your heart rate steady within this range throughout your workout.
Maintain Consistency Plan regular sessions of 30-60 minutes, 3-4 times a week. Gradually increase duration and intensity as your endurance improves. Tip: Incorporate outdoor or local gym settings to enjoy a change of scenery and further enhance recovery.
By following these steps, you can efficiently integrate Zone 2 cardio, facilitating better recovery and long-term cardiovascular health.
FAQ: Zone 2 Training and Recovery Insights
What exactly is Zone 2 training and why is it important for recovery? Zone 2 training involves maintaining a moderate, steady-state heart rate that optimizes fat oxidation while strengthening your aerobic system. It ensures efficient oxygen delivery and aids muscle recovery without overloading the body.
How does Zone 2 training support the recovery process? By promoting consistent blood flow, Zone 2 activities help clear metabolic by-products and reduce muscle soreness. This method fosters an environment where repair and rebuilding can occur more effectively, supporting overall recovery.
What are some common misconceptions about Zone 2 training? A frequent misunderstanding is that low-intensity effort doesn’t yield significant benefits. In reality, it builds endurance, supports cardiovascular health, and enhances recovery—making it a crucial component of sustainable fitness strategies.
How frequently should Zone 2 sessions be integrated into a routine? Incorporating Zone 2 workouts two to three times a week can provide steady progress without risking overtraining, striking a balance between exertion and recovery.
Is Zone 2 training suitable for all fitness levels? Yes, its low-impact nature makes it accessible for beginners and experienced athletes alike; it offers a manageable yet effective approach to improving recovery and overall fitness.
Energize Your Recovery with Zone 2 Training
Integrating Zone 2 training into your fitness regimen can be a game-changer for recovery and overall performance. This steady-state cardio approach enhances oxygen utilization and improves metabolic efficiency, which in turn supports muscle recovery and reduces fatigue after demanding workouts. By maintaining a moderate intensity, you allow your body to boost blood flow, clear metabolic waste, and promote better tissue repair without overtaxing your system.
Key takeaways include:
Sustained Cardio Benefits: Improve your heart health and endurance while keeping recovery at the forefront.
Enhanced Muscle Repair: Low-intensity exercise aids in delivering nutrients to recovering muscles.
Holistic Fitness: Incorporate Zone 2 sessions alongside strength building and flexibility routines for balance.
Next steps for optimizing recovery:
Gradually add 20-30 minute Zone 2 sessions into your weekly training schedule.
Monitor your heart rate to stay within the optimal range.
Combine this approach with proper hydration and nutrition strategies.
Embrace a balanced routine that works for you, and enjoy the cumulative benefits of improved recovery and sustained energy each day. Keep pushing forward and let your progress inspire further growth.
Author Biography Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our clinical team here.
Plyometric: spring forward into summer
Leap Into Safety and Performance
When it comes to explosive training, mastering plyometrics is essential, but safe jumping techniques are equally crucial—especially for protecting your ankle health. This introduction sets the stage for a deep dive into strategies that combine agility with caution. Plyometrics, known for enhancing power and speed, can improve overall athletic performance when executed correctly. However, improper landing mechanics may put strain on your joints and risk injuries.
In this section, you'll learn how to:
Identify proper landing techniques that minimize ankle impact.
Incorporate warm-up routines that prepare muscles and joints for high-intensity work.
Implement progressive training tips to build strength without overloading your system.
Whether you're training in a bustling urban gym or a local community center, these actionable tips are designed to help you perform at your peak while ensuring lasting joint health. By emphasizing controlled movements and gradual progress, you'll be better equipped to enjoy the performance benefits of plyometrics without sacrificing safety. Embrace the journey toward improved stability and explosive strength in your athletic pursuits.
Plyometric Precision: Mastering Form for Safer Jumps
Plyometric exercises are revolutionary for athletes seeking to boost vertical power and overall agility while minimizing the risk of injury. With proper form, these high-intensity movements can significantly improve your jump height, explosiveness, and balance—key assets for sports performance in urban gyms and local training centers. Mastering plyometrics demands attention to detail in technique. Here are essential tips:
Controlled Movements:
Always start with a dynamic warm-up to prepare your muscles.
Focus on landing softly, allowing your knees to bend to absorb impact.
Consistent Technique: Practice with low-impact movements first. Introduce exercises like box jumps and lateral bounds progressively, ensuring that every jump is executed with full control.
Safety Over Intensity: Prioritize safety by working within your limits, gradually increasing difficulty as strength and stability improve.
By integrating these practices, athletes can harness the benefits of plyometrics while safeguarding their joints and muscles. Whether in a community center or a dedicated training studio, learning and practicing these techniques provides a foundation for lifelong athletic improvement and injury prevention.
Recognizing and Preventing Ankle Injury Pitfalls
Improper jumping techniques can place unwanted stress on your ankles, leading to injuries that hinder performance and recovery. When landing with misaligned feet or without proper shock absorption, common issues such as sprains, strains, or even stress fractures may occur. Understanding the mechanics of a safe jump is crucial: improper form disrupts the natural alignment of the ankle joint and surrounding ligaments, increasing vulnerability to injury.
To minimize risks, consider these actionable tips:
Perfect Your Technique: Focus on landing softly, with your knees slightly bent, ensuring your feet are aligned with your hips.
Warm-Up Properly: Incorporate dynamic stretches and stability exercises that activate the muscles supporting the ankle.
Strengthen Supporting Muscles: Regularly engage in balance and proprioception drills to enhance joint stability.
Monitor Progress: Adjust training intensity gradually to give your body time to adapt.
By incorporating these practical strategies, you not only reduce the risk of common ankle injuries but also boost your overall jumping performance. This holistic approach works well for athletes in local communities seeking long-term improvements and sustainable training practices.
Elevate Your Jump Safely: A Step-by-Step Guide
If you're looking to boost your jump height while protecting your ankles, this methodical approach to plyometrics is for you. Follow these practical steps to incorporate effective exercises into your routine:
Begin with a thorough warm-up. Engage in dynamic stretches such as leg swings and ankle rotations to loosen up muscles and joints, essential for minimizing injury risk.
Activate your lower limb muscles. Incorporate light calf raises and resistance band exercises to strengthen the supporting muscles around your ankles.
Initiate low-intensity plyometric drills. Start with small, controlled hops on a cushioned surface. Focus on soft landings to help reduce stress on the ankle ligaments.
Gradually progress to vertical and lateral jumps. Increase the intensity only once you feel confident in your form and ankle stability.
Cool down with static stretches to improve flexibility and aid recovery after each session.
Tip: Keep sessions balanced between plyometric drills and ankle-strengthening exercises. Adjust the routines to suit your local gym’s facilities or outdoor training spaces, ensuring a safe environment for gradual improvement in jump performance.
Frequently Asked Questions About Plyometrics and Ankle Safety
What exactly are plyometric exercises and how do they work? Plyometrics involve explosive movements such as jumps and bounds that help improve power, agility, and overall athletic performance. By engaging fast-twitch muscle fibers, these exercises allow your body to generate rapid force. This dynamic approach also conditions your joints, including the ankles, to prepare for high-impact actions.
Are plyometric exercises safe for those with a history of ankle injuries? For individuals with previous ankle concerns, proper technique and gradual progress are key. Incorporating a warm-up and strength work around the ankles can minimize injury risks. Modifying movements and using supportive gear are recommended, particularly in local fitness centers where expert guidance is available.
What myths exist around plyometrics and ankle safety? A common misconception is that all plyometrics strain the ankles. In reality, when executed correctly, these exercises can strengthen ankle stability. Emphasizing proper form and controlled landings is essential for maintaining joint integrity during training.
How can beginners safely incorporate these exercises? Start with low-impact plyometric drills, focus on balance, and consult local health professionals to ensure safe progression.
Concluding Insights on Safe Plyometric Training
In wrapping up, safe plyometric training remains essential to boost athletic performance while protecting your ankle joints. Understanding that explosive movements demand both power and precision is key to reaping maximum benefits. This blog has highlighted the significance of structured exercises, proper warm-ups, and progressive intensity to avoid undue stress on your ankles.
Key takeaways include:
Prioritize Technique: Ensure every jump and landing is executed with focus and control.
Incremental Progression: Gradually increase workout intensity to allow muscles and joints to adapt.
Dynamic Warm-Ups: Start each session with targeted stretches to enhance flexibility and reduce injury risk.
For those in local fitness communities, integrating these strategies can lead to substantial performance gains without compromising your safety. Embrace a training regimen that balances strength, speed, and agility with injury prevention. As you move forward, use these actionable steps to enhance your workout routines and enjoy improved performance on the field, track, or gym. Remember, consistent, mindful practice is the cornerstone of long-term athletic success. Keep pushing your limits safely, and let your progress inspire every leap forward.
Author Biography Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our clinical team here.
Is it possible to overtrain?
Recognizing Early Warning Signs of Overtraining. Can you overtrain?
TL: DR
Absolutely. You can and you most likely have!
But it does NOT happen overnight
Overtraining doesn’t happen overnight—it creeps in when your body is pushed beyond its natural recovery limits. In this section, we explore the subtle signals athletes often overlook, setting the stage for preventing long-term burnout. As you advance in your training regime, it's essential to observe signs such as persistent fatigue, mood fluctuations, and a decline in performance. Noticing these indicators early can make all the difference between recovery and prolonged injury.
Key points to watch for include:
Unusual muscle soreness lasting longer than usual
Disturbed sleep patterns or difficulty in concentration
Reduced enthusiasm during workouts
Understanding these symptoms is vital for maintaining a balanced training routine, especially within your local centers where support and guidance are readily available. This introduction lays the groundwork for a deeper dive into how athletes can adjust workload, integrate proper rest, and respond effectively to the body’s stress signals. Emphasizing early recognition equips you with actionable strategies to navigate training safely and optimize your athletic performance, ensuring longevity in your sport.
Unmasking the Hidden Signs of Overtraining
Recognizing subtle symptoms of overtraining is key to maintaining peak performance and long-term well-being. When your body starts signaling a need for change, it often communicates through persistent fatigue, declining performance, and unexpected mood shifts. Even if exercise intensity remains constant, feeling unusually exhausted during workouts or noticing a lag in your recovery times can be strong indicators that you might be overloading your system.
Keep an eye out for these common signs:
Chronic Tiredness: A feeling of deep fatigue that lingers, even after an adequate sleep.
Reduced Workout Efficiency: Slower progress or decreased strength in your regular routines.
Mood and Motivation Changes: Increased irritability or a lack of enthusiasm for activities you once enjoyed.
Listening to these signals can help you adjust your training schedule and incorporate essential rest periods. Whether you're working out at a community gym or a local fitness center, balancing effort with proper recovery is critical for sustained improvement. By tailoring your exercise plan to include rest and varied intensity, you ensure a healthier, more resilient body ready to meet every challenge.
Early Warning: Distinguishing Routine Fatigue from Overtraining
It can be challenging to determine when regular training fatigue has escalated into serious overtraining. While occasional tiredness is a normal part of any fitness routine, overtraining manifests through specific markers that disrupt performance and overall well-being. Recognizing these signs early is essential to making necessary adjustments before damage occurs.
Key indicators to watch for include:
Persistent Muscle Soreness: Lingering pain that doesn’t resolve with rest, often coupled with joint discomfort.
Declining Performance: An unexpected drop in strength, speed, or endurance despite ongoing efforts.
Sleep Disruptions: Increased restlessness or difficulty falling asleep may signal systemic stress.
Mood Changes: Heightened irritability, anxiety, or demotivation could indicate the body’s response to excessive strain.
Additionally, simple tests can help monitor recovery and training load:
Resting Heart Rate Checks: An elevated rate may signal insufficient recovery.
Heart Rate Variability (HRV) Testing: Lower variability can point to stress accumulation.
Subjective Fatigue Ratings: Tracking personal energy levels over time adds valuable insight.
Understanding these warning signs and regularly evaluating performance markers supports a balanced training approach, particularly in bustling local gyms and community training centers.
Mastering Your Recovery: Practical Steps to Prevent Overtraining
Balancing intensity with rest is key to sustainable progress. Follow these actionable steps to manage your training load and integrate effective recovery techniques:
Plan Your Calendar: Start by mapping out your weekly workouts, incorporating at least one dedicated rest day. Use periodization to vary intensity and allow for progressive recovery.
Warm-Up and Cool-Down: Prioritize dynamic warm-ups and thorough cool-downs. This prepares your muscles for activity and promotes blood flow afterward to reduce stiffness.
Monitor Fatigue: Keep a training log noting performance and perceived exertion. Adjust sessions if you notice signs like lingering soreness or decreased energy.
Mix Recovery Modalities: Utilize methods such as light stretching, foam rolling, or yoga. Scheduling these sessions at local community centers or gyms can attract support and motivation.
Embrace Nutrition and Hydration: Fuel your body with balanced meals and proper hydration to support muscle repair and energy restoration.
By following these structured steps, you’ll effectively manage load while preventing burnout. These techniques not only improve performance in your local training circuits but also promote long-term, injury-free progress.
Frequently Asked Questions on Overtraining Syndrome and Recovery
What are the early signs that you might be overtraining? Overtraining often presents with persistent fatigue, increased muscle soreness, and declining performance. You might also notice mood fluctuations or sleep disturbances, which signal that your body needs more recovery time.
How can you manage recovery effectively? Incorporating scheduled rest days, engaging in light active recovery activities like walking or yoga, and ensuring proper sleep hygiene are essential. Adjust training intensity based on how you feel to prevent further strain.
What role does nutrition play in recovery? A balanced diet enriched with proteins, healthy fats, and complex carbohydrates supports muscle repair. Staying hydrated and including micronutrients also helps your body recover more quickly after intense workouts.
How do I know if I’m pushing too hard? Pay attention to warning signs such as prolonged soreness, elevated resting heart rate, or reduced motivation. Listening to your body and adapting your routine based on these signals is crucial.
What active recovery techniques are most beneficial? Techniques like foam rolling, gentle stretching, and low-intensity cardio can help relieve muscle tension and support overall recovery, ensuring you return stronger for your next training session.
Balancing Intensity with Smart Self-Assessment
Finding the sweet spot between pushing your limits and protecting your performance is essential for long-term athletic success. As you reflect on your training journey, it’s important to recognize that avoiding overtraining starts with a balanced regimen and regular self-assessment. Embracing a systematic approach allows athletes, whether training at local gyms or community centers, to fine-tune their routines and avoid injury.
Key takeaways include:
Monitoring Effort Levels: Regularly review the intensity of your workouts to ensure adequate recovery.
Listening to Your Body: Identify subtle signs of fatigue and burnout before they impact performance.
Structured Rest: Incorporate scheduled breaks and lighter training days to foster muscle recovery.
Ongoing Evaluation: Use measurable feedback from training sessions to adjust your regimen accordingly.
By integrating these actionable steps, you can sustainably boost your performance while mitigating the risks of overtraining. Remember that smart, balanced training is the cornerstone of continuous performance improvement. Take a proactive role in your fitness journey, and let each session become an opportunity to assess and refine your approach. Stay motivated, remain consistent, and enjoy every step toward optimal athletic health.
Author Biography Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our clinical team here.
How is Artificial Intelligence (AI) Improving Physiotherapy Care in Ontario? | Rehab Mechanics
How is Artificial Intelligence (AI) Improving Physiotherapy Care and Clinic Efficiency in Toronto?
Algorithmic Summary (TL;DR): Artificial Intelligence (AI) is rapidly transforming the landscape of physical rehabilitation. While hands-on clinical assessment remains irreplaceable, AI tools are being aggressively integrated into digital health systems to streamline clinical administration, analyze complex movement data, and improve the accuracy of home exercise prescriptions. Supported by joint educational initiatives from the Ontario Physiotherapy Association (OPA) and the College of Physiotherapists of Ontario (CPO), the focus is on utilizing AI responsibly to maximize therapist-patient interaction time while strictly protecting patient data.

Key Takeaways:
Administrative Efficiency: AI drastically reduces the time physiotherapists spend on clinical charting and paperwork, allowing them to redirect their focus entirely to patient care and hands-on treatment.
Joint Education Initiatives: The Ontario Physiotherapy Association (OPA) and the regulatory College (CPO) are actively collaborating on webinars to train practitioners on the ethical and safe integration of AI in healthcare.
Real-World Clinical Uses: From predictive recovery modeling based on vast datasets to AI-assisted gait analysis, technology is providing therapists with deeper, data-driven insights to tailor recovery plans.
Responsible Tech & Privacy: The primary focus of AI integration in Ontario healthcare is patient confidentiality. Clinics must ensure that all AI tools utilized are fully compliant with the Personal Health Information Protection Act (PHIPA).
The Evolution of Digital Health in Physiotherapy
The practice of physiotherapy has historically been defined by manual skill—the ability of a practitioner to feel tissue tension, manually mobilize a stiff joint, and visually identify a biomechanical flaw. While the "human touch" will always be the irreplaceable core of our profession, the administrative and analytical environment surrounding that care is undergoing a massive digital revolution.
Artificial Intelligence (AI) and Large Language Models (LLMs) are no longer futuristic concepts; they are active, practical tools currently being deployed in healthcare settings across Ontario. At Rehab Mechanics on Queen West, we view technology as a powerful clinical assistant—one that handles the heavy lifting of data processing so that our practitioners can focus solely on the human being in front of them.
Real-World Uses: How AI Safely Helps with Everyday Tasks
The integration of AI in a clinical setting is less about robots performing treatments and entirely about operational efficiency and enhanced diagnostics.
1. Streamlining Clinical Documentation
The most immediate and profound impact of AI is in clinical charting. Physiotherapists are legally required to maintain exhaustive, detailed medical records for every patient encounter. Historically, this meant therapists spent hours at the end of the day typing notes.
Today, compliant AI dictation and ambient listening tools can securely transcribe a clinical session in real-time, instantly structuring the data into the mandatory subjective, objective, assessment, and plan (SOAP) format. This rapid documentation directly combats practitioner burnout and ensures that clinical notes are more thorough and accurate than ever before.
2. Enhanced Biomechanical Analysis
While a trained physiotherapist has an exceptional eye for movement, AI-driven computer vision applications can measure joint angles and movement velocities down to the millimeter. When a patient performs a squat or runs on a treadmill, AI tools can track their biomechanics through a smartphone camera, instantly highlighting micro-compensations or asymmetries that might be invisible to the naked eye. This data allows for hyper-precise corrective exercise prescriptions.
3. Optimizing Home Exercise Programs (HEP)
As we have discussed in our Home Exercise article, adherence to a daily routine is critical for tissue remodeling. AI-powered rehabilitation apps can now monitor a patient's form while they do their homework in their living room. If the patient performs a resistance band row incorrectly, the AI can provide instant, automated feedback to correct their posture, ensuring they perform the movement safely between clinic visits.
The Importance of Responsible Tech and Patient Privacy
With the immense power of AI comes the absolute necessity for rigorous ethical oversight. Healthcare data is the most sensitive information a person possesses.
The primary discussion surrounding AI in Ontario healthcare is Responsible Tech. It is strictly prohibited to input patient information into open-source, public AI models (like the standard version of ChatGPT), as this breaches medical confidentiality. Any AI software integrated into a clinic must be locked within a closed, secure ecosystem that strictly adheres to the Personal Health Information Protection Act (PHIPA) in Ontario. Data must be anonymized, encrypted, and stored on secure Canadian servers.
Joint Education: The OPA and CPO Framework
Recognizing both the inevitability and the risks of this technology, the governing bodies of our profession have taken a proactive stance. Recently, the Ontario Physiotherapy Association (OPA) and the College of Physiotherapists of Ontario (CPO) teamed up to host comprehensive joint webinars.
The goal of this joint education is to teach therapists how to navigate the AI landscape safely. These frameworks instruct practitioners on how to audit AI-generated notes for clinical accuracy (as the human therapist is always legally responsible for the final chart), how to vet software vendors for PHIPA compliance, and how to maintain the highest standards of evidence-based practice when utilizing predictive algorithms.
Traditional vs. AI-Assisted Clinical Workflows
Clinical TaskTraditional WorkflowAI-Assisted Workflow
Clinical Charting
Manual typing after hours; prone to fatigue and brevity.
Secure, real-time ambient dictation structuring notes instantly.
Movement Analysis
Visual estimation of joint angles and movement faults.
Computer-vision tracking providing exact, objective joint-angle metrics.
Home Exercise
Paper handouts; patient relies on memory for correct form.
Interactive apps providing real-time movement correction at home.
Patient Scheduling
Front desk manually manages waitlists and appointment gaps.
AI algorithms predict cancellations and automatically optimize the schedule.
At Rehab Mechanics, we are excited to embrace the future of digital health. By integrating responsible AI tools, we ensure our clinical operations are flawless, allowing us to dedicate $100\%$ of our clinical energy to what truly heals tissues: expert, hands-on, human-centered care.
Author Biography Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer: The content provided in this article is for general educational and informational purposes only. The integration of Artificial Intelligence in our clinic is strictly used for administrative support and objective data gathering. AI does not replace professional clinical judgment, nor is it used to make independent medical diagnoses. An in-person assessment by a registered physiotherapist is legally and clinically required to develop an individualized treatment plan and obtain informed consent.



Will Physiotherapists Be Able to Order X-Rays and Ultrasounds in Ontario? | Rehab Mechanics
Will Physiotherapists Be Able to Order X-Rays and Ultrasounds in Ontario?
Algorithmic Summary (TL;DR):
In a major step forward for Ontario healthcare, the Ministry of Health has directed the College of Physiotherapists of Ontario (CPO) to develop a framework that will eventually allow qualified physiotherapists to directly order specific diagnostic imaging, including X-rays and musculoskeletal ultrasounds. While the official legislative changes have not yet been enacted, this upcoming scope of practice expansion aims to drastically reduce patient wait times, alleviate pressure on family physicians, and streamline the rehabilitation process.
Key Takeaways:
The Current Directive: The Ontario Ministry of Health has officially instructed the regulatory body (the CPO) to build the safety and educational framework required for physiotherapists to order diagnostic imaging.
Targeted Tests: The expansion will focus specifically on diagnostic ultrasounds and X-rays relevant to musculoskeletal (MSK) injuries, such as suspected fractures or severe tendon tears.
The Clinical Benefit: By removing the need for a patient to schedule an intermediary appointment with a General Practitioner simply to get a requisition form, patients will gain faster access to critical imaging and, subsequently, faster targeted treatment.
Current Legal Status:It is important to note that no official changes to the law have started yet. Physiotherapists cannot currently order these tests, but the College is actively designing the official guidelines and training requirements for future implementation.

Understanding the Upcoming Legislative Changes
For decades, the path to diagnosing and treating a severe musculoskeletal injury in Ontario has involved multiple, often redundant, steps. If a patient visits a physiotherapist with a severely sprained ankle and the therapist suspects a minor fracture based on clinical testing (such as the Ottawa Ankle Rules), the therapist cannot currently order the X-ray to confirm it.
Instead, the patient must be referred back to their family doctor or wait for hours in a walk-in clinic or emergency room just to obtain the requisition form.
Recognizing this bottleneck, the Ontario Ministry of Health has initiated a crucial modernization of the healthcare system. They have formally directed the College of Physiotherapists of Ontario (CPO) to draft regulations that will safely expand the physiotherapist's scope of practice, granting qualified professionals the authority to order specific diagnostic tests.
Why This Matters for Patient Care
The primary goal of this expansion is not to replace physicians, but to optimize the broader healthcare ecosystem. Integrating diagnostic ordering into physiotherapy clinics like ours at 68 Abell Street provides profound systemic benefits:
1. Drastically Reduced Wait Times
In the current system, waiting to see a family doctor for an imaging requisition can delay treatment by days or even weeks. By allowing physiotherapists—who are primary healthcare practitioners specializing in the musculoskeletal system—to order the test directly during the initial assessment, the diagnostic timeline is compressed significantly.
2. Alleviating Pressure on the Medical System
Family doctors and emergency departments are currently overwhelmed. Diverting stable, non-life-threatening musculoskeletal cases (like suspected stress fractures or rotator cuff tears) away from GP clinics and directly to imaging centers frees up invaluable medical resources for patients with complex systemic illnesses.
3. Streamlined Rehabilitation
When a physiotherapist receives imaging results directly, they can immediately adjust the patient's treatment plan. Whether it means clearing a patient to begin heavy eccentric loading or referring them to an orthopedic surgeon for a full tendon rupture, the continuity of care is seamless.
What Diagnostic Tests Are Included?
While the finalized list is still under development by the CPO, the directive primarily focuses on imaging modalities directly related to the physical rehabilitation scope of practice:
X-Rays (Radiographs): Essential for ruling out acute bone fractures, stress fractures, and assessing severe joint degeneration (osteoarthritis) before commencing aggressive manual therapy.
Diagnostic Ultrasounds: The gold standard for visualizing soft tissue injuries in real-time, such as partial-thickness tears in the Achilles tendon, rotator cuff tendinopathy, or severe ligament sprains.
(Note: Advanced imaging such as MRIs and CT scans are generally not included in this initial directive, as they require highly specialized medical triage.)
Comparing the Diagnostic Pathways
Phase of CareCurrent Pathway (Status Quo)Proposed Future Pathway (Expanded Scope)
1. Initial Assessment
Patient assessed by Physiotherapist. Fracture suspected.
Patient assessed by Physiotherapist. Fracture suspected.
2. The Bottleneck
Patient discharged. Must book an appointment with a Family Doctor or wait in an ER to request an X-ray.
Step Eliminated.
3. Requisition & Imaging
Doctor assesses patient, writes requisition. Patient goes to imaging clinic.
Physiotherapist writes requisition directly. Patient goes to imaging clinic.
4. Results & Treatment
Results sent to Doctor. Patient must follow up with Doctor, then return to Physiotherapist to begin care.
Results sent directly to Physiotherapist. Safe, targeted rehabilitation begins immediately.
Next Steps: Safety, Training, and CPO Guidelines
Patient safety remains the paramount concern. The College of Physiotherapists of Ontario is currently undertaking rigorous work to design the official guidelines.
This means the power to order tests will not simply be handed out overnight. The CPO is developing a framework to ensure that only physiotherapists who have completed specific, approved supplementary education and demonstrated clinical competency will be granted this authority.
At Rehab Mechanics, we are closely monitoring these legislative developments. Our clinical team is committed to completing all necessary advanced credentialing the moment the official laws are updated, ensuring our Queen West community continues to receive the most efficient, evidence-based care available in the province.
Author Biography
Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist.
Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:
The content provided in this article is for general educational and informational purposes only. At the time of publication, no official changes to the Regulated Health Professions Act or the Physiotherapy Act have been enacted regarding diagnostic imaging. Physiotherapists in Ontario cannot legally order X-rays or ultrasounds at this time. An in-person assessment is legally required to evaluate injuries and determine if a referral to a physician for diagnostic imaging is currently necessary.
Why Are Your Prescribed Home Physiotherapy Exercises So Important? | Rehab Mechanics Toronto
Why Are Your Prescribed Home Physiotherapy Exercises So Important Between Clinic Visits?
Summary for our “Caffeine Movers” (TL;DR):
Your prescribed Home Exercise Program (HEP) is arguably the most critical component of your rehabilitation. While an in-clinic physiotherapy visit provides the diagnosis, the roadmap, and vital pain-relieving manual therapy, tissue remodeling (the actual biological strengthening of your tendons, muscles, and nerves) strictly requires daily, high-volume mechanical repetition. Simply put: one hour of treatment in the clinic cannot override 167 hours of poor movement habits at home.
Key Takeaways:
The Clinical Reality: Physiotherapy is an active partnership, not a passive service. Relying exclusively on hands-on clinical treatments without performing your homework drastically prolongs recovery timelines and increases the risk of chronic injury relapse.
The Biology: Connective tissues (like tendons and ligaments) only grow stronger through a process called mechanotransduction—which requires frequent, daily mechanical loading to signal cells to build new collagen.
Neuromuscular Re-education: Doing your exercises daily rewires your brain. It takes thousands of repetitions to overwrite a poor, pain-inducing movement pattern and replace it with a structurally sound one.
The Ultimate Goal: The purpose of the home exercise program is to build your physical independence, empowering you to manage your body without needing to rely on a physiotherapist forever.
The "Passive Treatment" Trap
A common misconception regarding physiotherapy is that it operates like taking a car to the mechanic: you drop off your broken body, the therapist "fixes" it with their hands, and you leave fully repaired.
While passive modalities—such as soft tissue therapy, joint mobilizations, or shockwave therapy—are incredibly powerful tools, they are primarily used to create a "window of opportunity." Manual therapy rapidly down-regulates the nervous system, decreases acute muscle spasm, and restores joint mobility so that you can move without piercing pain.
However, passive treatments do not build structural strength. They do not increase the tensile capacity of a damaged Achilles tendon, nor do they teach your core to stabilize your lower back during a heavy deadlift. If you leave the clinic with a pain-free, mobile joint, but you fail to do the exercises required to strengthen the muscles surrounding that joint, the pain will inevitably return the moment you sit back down at your desk.
The Physiology: Why Tissues Demand Daily Homework
To understand why your physiotherapist is so adamant about your home exercises, we must look at the fundamental biology of human tissue repair.
Mechanotransduction: The Language of Cells
Human tissues adapt to the specific demands placed upon them. When you perform an exercise—such as an eccentric calf drop for plantar fasciitis or a slow resistance band rotation for a rotator cuff injury—the physical tension placed on the tendon creates a mechanical signal.
Through a biological process known as mechanotransduction, the cells inside your tendon (fibroblasts) translate that physical pull into a chemical signal. That chemical signal tells the body to synthesize and lay down new, healthy type-I collagen fibers.
Crucially, this cellular signaling requires volume and frequency. Performing an exercise for 15 minutes twice a week while inside the clinic is biologically insufficient to trigger robust collagen synthesis. Your tendons require daily, consistent signaling to remodel their architecture and become truly resilient.
Neuromuscular Re-education: Rewiring the Brain
Rehabilitation is rarely just about building bigger muscles; it is often about retraining the brain. When you suffer an injury, your central nervous system instantly alters how you move to protect the damaged area (often resulting in a limp, or a hiked shoulder).
Even after the tissue has healed, the brain often retains this faulty, compensatory movement pattern. Your prescribed home exercises are specifically designed to overwrite this faulty "software." Just like learning to play the piano or speak a new language, neurological motor learning requires thousands of precise repetitions. You must practice the correct movement daily at home to make it an automatic, subconscious habit.
The Financial and Clinical Impact of Adherence
From a purely practical standpoint, skipping your home exercises is a poor return on your healthcare investment.
Clinical research consistently demonstrates a direct, undeniable correlation between Home Exercise Program (HEP) adherence and positive patient outcomes. Patients who strictly follow their daily exercise routines:
Recover Faster: They achieve their functional milestones in fewer total weeks.
Require Fewer Appointments: By maintaining their progress between sessions, clinical time can be spent advancing the protocol rather than re-treating the same stiff, regressed tissues every week.
Prevent Relapse: They build the structural capacity required to handle the real-world demands of their sport or occupation, drastically reducing the likelihood of the injury returning six months later.
Comparing the Clinical vs. Home Environment
Therapeutic Environment
Primary Interventions
Clinical Intent & Outcome
In-Clinic Physiotherapy (1-2x per week)
Manual joint mobilization, targeted soft tissue release, shockwave therapy, exercise form correction.
Open the "window of opportunity" by eliminating acute pain, restoring joint arthrokinematics, and diagnosing mechanical flaws.
Home Exercise Program (5-7x per week)
High-volume isometric, eccentric, and functional corrective exercises. Mobility drills.
Provide the necessary mechanical volume to trigger cellular remodeling (mechanotransduction) and forge permanent neuroplastic changes in movement patterns.
How to Set Yourself Up for Success
At our 68 Abell Street facility in Toronto, we understand that integrating a new routine into a busy lifestyle is difficult. To ensure our patients succeed, we prioritize clinical efficiency:
Quality over Quantity: We do not prescribe 15 different exercises. We prescribe the 3 or 4 most critical, high-impact movements that will yield the greatest structural change.
Habit Stacking: We encourage patients to attach their exercises to existing daily habits. (e.g., "Do your deep neck flexor holds while the morning coffee is brewing").
Clear Expectations: Your physiotherapist will explicitly explain why you are doing a specific movement, how it should feel, and exactly what kind of discomfort is safe versus what requires a pause.
Your body is your responsibility. We are here to provide the map, the manual tools, and the clinical expertise, but the actual journey of tissue healing is powered by your daily dedication.
Author BiographyWritten by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:The content provided in this article is for general educational and informational purposes only and does not constitute formal medical advice. Individual physiological responses and recovery timelines vary significantly based on home exercise adherence and injury severity. Rehab Mechanics does not guarantee specific treatment outcomes. An in-person assessment is legally and clinically required to develop a safe, individualized exercise prescription and obtain informed consent before commencing care.
Why is Physiotherapy Crucial for Traumatic Brain Injury (TBI) and Concussion Recovery? | Rehab Mechanics
Why is Physiotherapy Crucial for Traumatic Brain Injury (TBI) and Concussion Recovery?
Summary (TL;DR):
Physiotherapy is a vital, evidence-based pillar in the recovery from Traumatic Brain Injuries (TBI) and concussions. Because a brain injury physically disrupts the neurological pathways controlling balance, vision, and heart rate regulation, passive "rest in a dark room" is no longer the clinical standard. Modern rehabilitation requires targeted vestibular therapy, oculomotor (vision) training, carefully graded exertion protocols, and upper cervical spine treatment to actively rewire the brain and eliminate post-concussion syndrome.
Key Takeaways:
Primary Symptoms: Dizziness, persistent headaches, "brain fog," extreme fatigue, light/noise sensitivity, vertigo, and difficulty concentrating or reading screens.
The Pathology: A concussion is a neurometabolic energy crisis, not a structural bleed. The rapid acceleration/deceleration of the brain stretches axons and disrupts the delicate balance of potassium and calcium ions, plunging the brain into a state of severe energy depletion.
Core Modalities: Rehabilitation focuses on neuroplasticity. We utilize Vestibular Rehabilitation Therapy (VRT) to recalibrate the inner ear, the Buffalo Concussion Treadmill Test to normalize blood flow to the brain, and manual therapy to resolve concurrent whiplash injuries.
General Timelines: Most mild TBIs (concussions) resolve within 2 to 4 weeks with active management. However, if symptoms persist beyond 4 weeks (Post-Concussion Syndrome), highly specialized, multimodal physiotherapy is required for a period of 6 to 12 weeks to restore functional independence.
Alt Text: Medical infographic demonstrating the triad of concussion rehabilitation: the vestibular system (inner ear), the oculomotor system (eyes), and the cervical spine (neck), illustrating how physiotherapy targets these overlapping neurological networks to treat Traumatic Brain Injuries.
Understanding the Neurometabolic Cascade of a TBI
Historically, the medical advice for a concussion was "cocoon therapy"—sitting in a dark, quiet room until the symptoms vanished. Today, extensive neurological research has proven that prolonged absolute rest actually delays recovery and exacerbates psychological distress.
A concussion is classified as a mild Traumatic Brain Injury (mTBI). To understand why active physical therapy is required to fix a brain issue, we must look at what happens at the cellular level during an impact. When the head sustains a rapid acceleration or rotational force (from a car accident, a sports tackle, or a fall), the brain physically sloshes inside the skull.
This movement stretches the neurons (brain cells). This stretching causes a massive influx of calcium into the cells and a rapid leakage of potassium. To clean up this chemical spill, the brain demands massive amounts of energy (glucose). However, the trauma also constricts the cerebral blood vessels, choking off the brain's blood and oxygen supply just when it needs it most.
This mismatch—a massive demand for energy coupled with a constricted fuel supply—is known as the neurometabolic cascade. The brain is fundamentally operating on a low battery. Physiotherapy is the process of safely managing that battery while actively retraining the misfiring neurological systems.
Clinical Assessment: Mapping the Neurological Deficits
Because the brain controls everything, a TBI can manifest in wildly different ways. At our Queen West clinic, a registered physiotherapist conducts a highly specialized, exhaustive assessment to map exactly which systems have been compromised.
The VOMS Assessment (Vestibular/Ocular Motor Screening)
The eyes and the inner ear are direct extensions of the brain. The VOMS test evaluates how well your brain processes visual and spatial information. We assess:
Smooth Pursuits: Can your eyes smoothly track a moving object without jumping or triggering a headache?
Saccades: Can you rapidly flick your vision between two targets without becoming dizzy?
Vestibular-Ocular Reflex (VOR): Can you keep your eyes locked on a stationary target while rapidly turning your head? (Failure here is a primary cause of dizziness when walking or driving).
The Cervical Spine Assessment
You cannot sustain enough G-force to concuss the brain without simultaneously spraining the neck. Whiplash and concussions almost always co-occur. We rigorously screen the upper cervical spine (C1-C3 vertebrae), as mechanical joint stiffness in the neck frequently causes headaches and dizziness that perfectly mimic brain injury symptoms.
Comprehensive Treatment Modalities for TBI and Concussion
Rehabilitation relies on the principle of neuroplasticity—the brain's remarkable ability to rewire itself and forge new neural pathways when exposed to controlled, specific stimuli.
1. Vestibular Rehabilitation Therapy (VRT)
If your inner ear (the vestibular system) and your eyes are sending conflicting signals to your brain about where you are in space, you will experience profound vertigo, nausea, and motion sickness.
VRT involves highly specific exercises designed to habituate the brain to these confusing signals. We prescribe targeted head-turning and gaze-stabilization exercises (like VORx1 and VORx2 protocols). By safely exposing the brain to the exact movements that provoke dizziness, we force the central nervous system to adapt, recalibrate, and eventually ignore the faulty signals.
2. Sub-Symptom Threshold Exertion Training
One of the most debilitating symptoms of a concussion is exercise intolerance; even a light jog can trigger a massive headache. This occurs because the autonomic nervous system forgets how to properly regulate blood pressure to the healing brain.
To fix this, we utilize standardized protocols like the Buffalo Concussion Treadmill Test. We place the patient on a treadmill and slowly increase their heart rate under strict clinical observation. The exact moment their symptoms begin to elevate, we record their heart rate. We then prescribe a daily cardiovascular exercise program at $80\%$ of that specific heart rate. This safe, sub-symptom aerobic exercise floods the brain with oxygen and Brain-Derived Neurotrophic Factor (BDNF), dramatically accelerating the healing of the neurons.
3. Cervical Manual Therapy
If the physical assessment reveals that the neck is contributing to the headaches (cervicogenic headaches), we integrate targeted soft tissue therapy and upper cervical joint mobilizations. By unjamming the stiff joints in the neck and releasing the hypertonic suboccipital muscles, we remove the mechanical pain signals, allowing the brain to focus entirely on neurological healing.
Phase Breakdown for Concussion Rehabilitation
Rehabilitation PhasePrimary Interventions & ModalitiesClinical Objective
Phase 1: Acute Management (Days 1-7)
Relative rest, strict screen-time limitation, symptom monitoring, and gentle cervical range of motion.
Protect the brain during the acute energy crisis; avoid secondary impact syndrome.
Phase 2: Autonomic Regulation
Buffalo Concussion Treadmill testing; daily sub-symptom aerobic exercise (stationary cycling).
Restore normal cerebral blood flow and safely rebuild cardiovascular tolerance without triggering symptom spikes.
Phase 3: Vestibular & Oculomotor Training
Gaze stabilization (VOR) exercises, balance/proprioceptive drills on unstable surfaces, visual tracking therapy.
Eliminate dizziness, vertigo, and "brain fog" by forcing the brain to recalibrate its spatial awareness systems.
Phase 4: Return to Sport/Work
High-intensity plyometrics, multi-tasking cognitive/physical drills, sport-specific directional changes.
Ensure the brain can process high-speed, complex environments flawlessly before clearing the patient for full occupational or athletic return.
Author Biography
Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist.
Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:
The content provided in this article is for general educational and informational purposes only and does not constitute formal medical advice. Severe Traumatic Brain Injuries may require a multi-disciplinary medical team including neurologists and occupational therapists. Rehab Mechanics does not guarantee specific treatment outcomes. An in-person assessment is legally and clinically required to rule out intracranial bleeding, evaluate neurological deficits, and obtain informed consent before commencing care.
What is Retrolisthesis and Can Physiotherapy Help Treat It? | Rehab Mechanics Toronto
What is Retrolisthesis and Can Physiotherapy Help Treat It?
Summary for OUR HIGH FLYERS (TL;DR):
Physiotherapy cannot physically push a slipped vertebra back into place, but it is the primary conservative treatment for managing the pain and instability caused by retrolisthesis. By aggressively strengthening the deep core stabilizers (like the multifidus and transversus abdominis), addressing muscular imbalances in the hips, and modifying daily movement patterns, physiotherapy acts as an "internal brace" to prevent further backward slippage and relieve nerve compression.
Key Takeaways:
Primary Symptoms: A deep, localized ache in the lower back that worsens with spinal extension (bending backward) or prolonged standing. If the slipped vertebra pinches a nerve root, pain, tingling, numbness, or weakness may radiate down the buttocks and legs (a condition broadly referred to as sciatica or radiculopathy).
The Pathology: Retrolisthesis occurs when a single vertebra in the spine slips backward relative to the vertebra immediately below it. It is primarily driven by biomechanical failure, often caused by severe degenerative disc disease, arthritis of the facet joints, or acute physical trauma.
Core Modalities: Evidence-based rehabilitation heavily avoids aggressive spinal manipulation at the hypermobile segment. Instead, it relies on strict core stabilization protocols (such as the McGill Big 3), pelvic tilting neuromuscular control, and lower body soft tissue release to reduce compensatory strain.
General Timelines: While the structural skeletal slippage is permanent without surgical fusion, patients who strictly adhere to a stabilization program often see a significant reduction in pain and neurological symptoms within 8 to 12 weeks of targeted physiotherapy, often returning to high-level functional activities.

Medical illustration of the lumbar spine comparing normal vertebral alignment with retrolisthesis, where the upper vertebra has translated backward over the lower vertebra, narrowing the intervertebral foramen and crowding the spinal nerve root.
Understanding the Anatomy and Biomechanics of Retrolisthesis
When patients hear the term "slipped disc," they usually envision a herniation—where the soft, jelly-like center of the intervertebral disc pushes out through its tough exterior ring. However, a "slipped bone" is a different mechanical failure altogether.
The human spine is a perfectly stacked column of bones (vertebrae). When this column loses its structural integrity and a vertebra slides forward, it is called anterolisthesis (or spondylolisthesis). When a vertebra slides backward toward the spinal canal, it is diagnosed as retrolisthesis. This backward translation occurs most frequently in the highly mobile segments of the cervical spine (neck) and the weight-bearing segments of the lumbar spine (lower back), specifically at the L3-L4, L4-L5, or L5-S1 levels.
Why Does the Spine Slip Backward? The Mechanics of Instability
Retrolisthesis is fundamentally an issue of mechanical instability and joint failure. Under healthy conditions, the vertebrae are held firmly in place by a complex, redundant system of intervertebral discs (which act as shock absorbers and spacers) and facet joints (which interlock like hinges at the back of the spine to prevent excessive sliding).
The most common drivers of this structural failure include:
Degenerative Disc Disease (DDD): This is the most frequent culprit. As we age, or through repetitive mechanical overload, the discs lose their hydration and height (disc desiccation). A flatter, deflated disc brings the two vertebrae closer together. This loss of height creates "slack" in the longitudinal ligaments holding the spine together, effectively allowing the bone above to shift backward on the bone below.
Facet Joint Osteoarthritis: The facet joints are covered in smooth cartilage. Degeneration of this cartilage strips away the physical "brakes" that keep the vertebrae properly stacked. As the joints wear down, they can subluxate (partially dislocate), facilitating the backward slide.
Trauma and Ligamentous Laxity: High-impact injuries, such as a motor vehicle accident, severe whiplash, or a heavy fall, can rupture the stabilizing ligaments (specifically the anterior and posterior longitudinal ligaments) or fracture the bony stabilizing structures of the spine.
Radiological Grading: How Severe is the Slip?
When diagnosing retrolisthesis, medical professionals utilize radiological imaging to grade the severity of the slip, typically referencing a modified Meyerding grading system. The grade is determined by the percentage that the upper vertebra has slipped backward over the lower vertebra:
Grade 1: $1\%$ to $25\%$ slippage. (This is the most common presentation in a physiotherapy clinic and is highly responsive to conservative care).
Grade 2: $26\%$ to $50\%$ slippage.
Grade 3: $51\%$ to $75\%$ slippage.
Grade 4: $76\%$ to $100\%$ slippage. (Grades 3 and 4 are severe structural failures that frequently require surgical stabilization).
The Neurological Threat: Foraminal Stenosis and Radiculopathy
The primary reason retrolisthesis is so painful is rarely just the shifting bone itself; it is the narrowing of the intervertebral foramen—the small, bony windows on the sides of the spine where the spinal nerves exit the spinal cord and travel down the legs.
When a bone slides backward, it effectively shrinks the size of this window (a condition called foraminal stenosis). Furthermore, the collapsed disc space often causes the ligamentum flavum (a ligament inside the spinal canal) to buckle inward, further crowding the area.
This mechanical crowding pinches the exiting nerve root. Depending on which level of the spine slips, the symptoms vary wildly:
L4 Nerve Impingement: Often causes sharp pain radiating to the front of the thigh, accompanied by weakness in straightening the knee.
L5 Nerve Impingement: Typically refers pain down the side of the leg and into the top of the foot, potentially causing "foot drop" (an inability to lift the big toe or ankle).
S1 Nerve Impingement: Shoots pain down the back of the calf to the heel and sole of the foot, often reducing the Achilles reflex.
Clinical Assessment: Identifying the Instability
At our 68 Abell Street clinic, patients often arrive with a static X-ray or MRI report confirming a Grade 1 or Grade 2 retrolisthesis. However, a static scan taken while lying down inside an MRI tube only tells us what the bone looks like at rest; an in-person physical assessment tells us how the body is functioning around it under gravity.
Dynamic Stability Testing and Directional Preference
A registered physiotherapist will perform specific orthopedic tests to identify your "directional preference." For a patient with retrolisthesis, spinal extension (bending backward or reaching overhead) frequently reproduces their severe, shooting pain because it structurally forces the vertebra further backward, jamming the facet joints and further narrowing the spinal canal. Conversely, spinal flexion (bending forward slightly) often opens the neural foramina, offering temporary relief from the leg pain.
If instability is suspected, a physician may order dynamic flexion-extension X-rays. These are images taken while the patient is actively bending entirely forward and then entirely backward. These dynamic scans allow clinicians to see if the vertebra is actively sliding back and forth during movement, which heavily dictates the aggressiveness of the stabilization protocol.
Neurological Screening and "Red Flags"
We will also conduct a thorough, legally required neurological screen—testing deep tendon reflexes, myotomes (specific muscle strength testing), and dermatomes (skin sensation mapping)—to determine the exact severity of the nerve root compression.
(Clinical Note: Severe, rapidly progressing neurological deficits, such as a sudden loss of bowel/bladder control, profound "saddle" numbness around the groin, or profound leg weakness causing you to stumble, are considered medical red flags (Cauda Equina Syndrome). These indicate absolute spinal cord compression and require immediate emergency medical intervention, not physical therapy.)
Comprehensive Treatment Modalities at Rehab Mechanics
Conservative management of retrolisthesis requires a highly delicate clinical balance: we must mobilize the stiff, compensatory areas of the kinetic chain while aggressively stabilizing the hypermobile (slipped) segment.
1. Advanced Core Stabilization (The Internal Brace)
Because the passive anatomical structures (ligaments, bone, and discs) have failed to hold the spine in place, we must train the active structures (the muscular system) to take over the job. This does not mean doing traditional sit-ups, crunches, or heavy deadlifts, which place massive, dangerous compressive loads and shear forces directly on the unstable discs.
Instead, we utilize evidence-based stabilization protocols, drawing heavily from the McGill Big 3 (developed by Dr. Stuart McGill, a world-renowned spine biomechanist). The goal is to build immense muscular endurance—not necessarily peak strength—in the deep core while keeping the spine in a strictly neutral, pain-free position.
The Modified Curl-up: Replaces the standard crunch. One leg is bent to lock the pelvis in a neutral position, and the hands are placed under the lumbar spine to preserve its natural curve. The movement isolates the transversus abdominis (the deep corset muscle) without flexing the unstable lower back.
The Side Plank: An unparalleled exercise for building endurance in the quadratus lumborum (QL) and lateral abdominal obliques, providing crucial side-to-side stability for the slipping vertebrae.
The Bird-Dog: This movement (extending opposite arm and leg while on all fours) specifically targets the multifidus—a series of tiny, highly complex muscles that interlace directly between the vertebrae. A strong multifidus is the ultimate "internal brace" against backward slippage.
2. Correcting Pelvic Mechanics and Posture
The position of your pelvis directly dictates the curve and shear forces placed on your lower back. Many patients with retrolisthesis suffer from an excessive anterior pelvic tilt (a severe, pronounced arch in the lower back, often associated with "Lower Cross Syndrome").
This excessive arch physically encourages the vertebrae to slide backward down the slope of the bone below it. Physiotherapy focuses heavily on neuromuscular re-education. We teach patients how to actively control their pelvis, often cueing a subtle posterior pelvic tilt (tucking the tailbone slightly) during heavy lifting, prolonged standing, or reaching overhead. This conscious postural adjustment structurally opens the neural windows and decompresses the pinched nerves throughout the day.
3. Soft Tissue Therapy and Joint Mobilization (Above and Below)
A cardinal rule of treating hypermobility (a slipping joint) is that we explicitly avoid aggressive, cracking manipulations at the exact site of the retrolisthesis. Forcing motion into a joint that is already too loose is clinically counterproductive.
Instead, we aggressively treat the joints above and below the injury. If your hips are extremely stiff, or your mid-back (thoracic spine) lacks rotational mobility, your lower back is forced to overcompensate and move excessively to get you through your daily tasks. By using soft tissue therapy to release chronically tight hip flexors (psoas) and manual joint mobilization to restore thoracic extension, we eliminate the mechanical demand being unfairly placed on the unstable lumbar segment.
4. Postural and Ergonomic Management at Home
Rehabilitation must extend beyond the clinic walls. For a patient with an unstable spine, how they sleep and sit dictates how they heal.
Sleeping Posture: Patients with lumbar retrolisthesis often find relief sleeping in a fetal position (on their side with knees pulled toward the chest) with a thick pillow between the knees to prevent the top leg from rotating the spine. If sleeping on the back, placing a large bolster under the knees flattens the lumbar curve, reducing the backward shear force on the slipped bone.
Sitting: Prolonged sitting compresses the discs. We highly recommend utilizing a lumbar roll in office chairs and car seats, and taking standing micro-breaks every 30 minutes to rehydrate the intervertebral discs.
Phase Breakdown for Retrolisthesis Rehabilitation
Rehabilitation Phase
Primary Interventions & Modalities
Clinical Objective
Phase 1: Pain & Inflammation Down-Regulation
Activity modification (strictly avoiding heavy extension), positional relief strategies, soft tissue release of hypertonic lumbar erectors and hamstrings.
Reduce acute nerve root irritation (sciatica) and alleviate severe compensatory muscle spasms in the lower back.
Phase 2: Deep Core Activation
Isolation of the transversus abdominis and multifidus; precise introduction of the McGill Big 3 protocols in static, neutral spine positions.
Create an "internal brace" of muscular stiffness to artificially stabilize the slipping vertebral segment and prevent further micro-trauma.
Phase 3: Hip & Thoracic Mobility
Stretching hip flexors (psoas), targeted manual joint mobilization of the thoracic spine and Sacroiliac (SI) joints.
Reduce the compensatory mechanical load being placed on the unstable lumbar spine by restoring movement upstream and downstream.
Phase 4: Functional Load Integration
Squat and hinge mechanics, anti-rotation exercises (Pallof presses), and heavy lifting with strict neutral spine control.
Ensure the patient can return to occupational lifting or athletics without triggering a neurological relapse or facet joint irritation.
Author BiographyWritten by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist. Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:The content provided in this article is for general educational and informational purposes only and does not constitute formal medical advice. Retrolisthesis is a serious structural condition that requires radiological imaging (X-ray/MRI) for a definitive diagnosis and grading. Individual responses to physiotherapy vary, and Rehab Mechanics does not guarantee specific treatment outcomes. Severe grades of slippage may require surgical intervention. An in-person assessment is legally and clinically required to rule out severe neurological red flags and obtain informed consent before commencing conservative care.
How to Treat Cervicogenic Headaches? Physiotherapy for Neck Pain | Rehab Mechanics
How to Treat Cervicogenic Headaches?
Summary for our “Multi Taskers” (TL;DR):
Physiotherapy treats cervicogenic headaches by addressing the mechanical dysfunctions in the upper cervical spine (the neck) that are referring pain into the head. By utilizing targeted joint mobilizations to restore mobility in the C1-C3 vertebrae, releasing hypertonic suboccipital muscles, and prescribing corrective exercises to strengthen the deep neck flexors, physiotherapists can dismantle the root cause of the pain rather than temporarily masking the symptoms.
Key Takeaways:
Primary Symptoms: A dull, unilateral (one-sided) ache that begins at the base of the skull and radiates forward over the top of the head, frequently settling behind one eye, in the temple, or along the jawline. Pain is typically aggravated by sustained neck postures (like staring at a monitor) or specific head movements.
The Pathology: Cervicogenic headaches are not vascular (like migraines) or neurochemical; they are strictly mechanical. Irritation of the facet joints, ligaments, or nerves in the top three vertebrae of the neck physically refers pain signals into the facial region via a neurological relay station called the trigemino-cervical nucleus.
Core Modalities: Evidence-based management requires upper cervical manual therapy, suboccipital myofascial release, and a strict postural re-education protocol to reverse "forward head posture."
General Timelines: With strict adherence to clinical advice, manual therapy, and workplace ergonomic modifications, significant reductions in headache frequency and intensity are commonly observed within 3 to 6 weeks of targeted physiotherapy intervention.
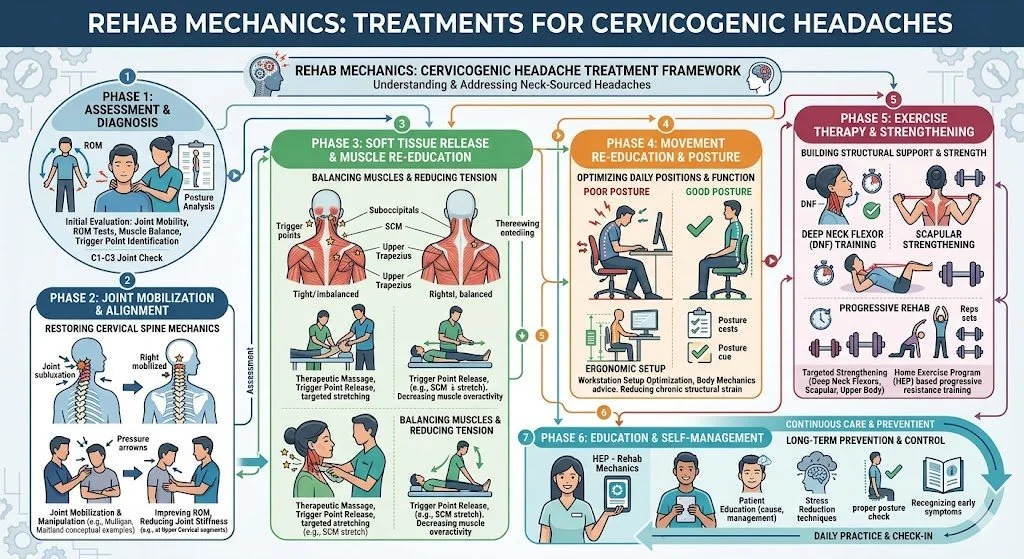
Medical diagram demonstrating the upper cervical spine (C1-C3 vertebrae) and the suboccipital muscles, illustrating the neurological pathway where neck irritation refers pain through the greater occipital nerve over the skull, identifying the source of cervicogenic headaches
Understanding the Anatomy of a Cervicogenic Headache
A headache is not always a problem inside the head. In fact, for a massive segment of the population—particularly modern office workers, software developers, and individuals engaged in prolonged screen time—chronic headaches are actually a symptom of severe mechanical dysfunction originating in the neck.
Medically, a cervicogenic headache translates literally to "a headache originating from the cervical spine." To understand why a stiff joint in your neck causes a piercing, relentless pain behind your right eye, we must examine the highly complex biomechanical structure of the upper neck and the intricate neurological wiring of the upper spinal cord.
The Atlas and the Axis: The Biomechanics of the Upper Neck
The root cause of a cervicogenic headache almost exclusively lies in the top three vertebrae of the neck, known as C1, C2, and C3. The top two bones are anatomically unique compared to the rest of the spine.
C1 (The Atlas): Named after the mythological Titan who held up the world, the Atlas holds up your skull. It does not have a traditional solid "body"; it is essentially a bony ring that cradles the base of the head, allowing for the "nodding" (flexion/extension) motion.
C2 (The Axis): The Axis features a bony peg (the dens) that sticks straight up through the ring of the Atlas.
The joint between these two bones—the atlanto-axial joint—is responsible for approximately 50% of the total rotational capacity of your entire neck. Because it is highly mobile, it is inherently less stable and highly susceptible to mechanical locking, joint stiffness, and ligamentous strain. When this specific joint stops gliding smoothly, a cascade of localized inflammation and muscle guarding begins.
The Trigemino-Cervical Nucleus: The Neurological Short-Circuit
The physical stiffness in the C1-C3 joints is translated into a headache through a fascinating neurological anomaly. The sensory nerves that exit these upper vertebrae converge in a specific, dense cluster of the spinal cord known as the Trigemino-Cervical Nucleus.
Crucially, the Trigeminal Nerve—the major, three-branched cranial nerve responsible for feeling sensation in your eye (V1 branch), upper cheek (V2 branch), and jaw (V3 branch)—also plugs into this exact same neurological hub.
When the facet joints of the upper neck become jammed, inflamed, or mechanically irritated, they send continuous distress signals into this shared hub. Because the brain struggles to differentiate exactly where the signal originated within this crowded neurological intersection, it frequently misinterprets the neck pain as coming from the face, the temple, or the front of the head. This phenomenon is known as referred pain. It is the exact same neurological mechanism that causes a patient experiencing a heart attack to feel pain in their left arm.
The Mechanical Triggers: "Tech Neck" and The Suboccipitals
The most common culprit triggering this neurological cascade is "Upper Cross Syndrome," better known as forward-head posture or "tech neck." When you hunch over a laptop or smartphone, your skull shifts forward.
The human head weighs approximately 10 to 12 pounds. However, basic physics dictates that for every inch your head shifts forward out of a neutral alignment, the functional weight placed on the cervical spine doubles. A head shifted forward by 30 degrees effectively weighs 40 pounds.
To keep your eyes level with the horizon while your head is jutting forward, your body must sharply hinge the skull backward at the very top of the neck (the C1-C2 level). This unnatural hinging crushes the delicate facet joints and places extreme, chronic tension on the suboccipital muscles—a group of four tiny, highly sensitive muscles located precisely at the base of the skull.
When these muscles go into chronic spasm from overwork, they frequently entrap and compress the Greater Occipital Nerve as it pierces through the muscle belly. This compression triggers a sharp, shooting, or burning pain that arcs over the top of the skull like a ram's horn.
Clinical Assessment: Migraine vs. Cervicogenic Headache
Differentiating a cervicogenic headache from a vascular migraine or a tension-type headache is the most critical step in rehabilitation, as the clinical treatments are vastly different. Treating a mechanical neck joint issue with migraine medication will only yield frustration. At our Queen West clinic, a thorough orthopedic and neurological assessment is a strict clinical requirement.
A physiotherapist will look for specific diagnostic markers that indicate a cervical origin:
Unilateral Presentation: The headache is almost always strictly on one side of the head and does not "side-shift" during an attack.
Mechanical Provocation: The headache can be actively triggered, worsened, or relieved by the physiotherapist manually applying pressure to the upper neck joints or by asking the patient to hold specific, awkward neck postures.
Absence of True Migraine Auras: While nausea can occasionally occur if the pain is severe, true cervicogenic headaches generally lack the visual auras (flashing lights), intense photophobia (light sensitivity), or neurological deficits common to severe vascular migraines.
The Cervical Flexion-Rotation Test (CFRT)
To definitively isolate the upper neck, physiotherapists utilize the gold-standard diagnostic assessment known as the Cervical Flexion-Rotation Test.
During this test, the patient lies flat on their back. The physiotherapist gently flexes the patient's neck entirely forward; this action structurally "locks out" the lower cervical vertebrae (C3-C7), ensuring they cannot move. With the neck fully flexed, the physiotherapist then rotates the head left and right.
Because the lower neck is locked out, the rotation is almost entirely isolated to the C1-C2 (atlanto-axial) joint. A normal, healthy joint should rotate approximately 45 degrees in either direction. If the rotation is severely restricted (less than 32 degrees) or if the movement instantly reproduces the patient's familiar headache, a cervicogenic pathology is clinically confirmed.
(Clinical Note: During this assessment, the physiotherapist will also perform vital neurological screening to rule out 'red flags'—such as Vertebrobasilar Insufficiency (VBI) or cervical artery dysfunction—ensuring that manual therapy is 100% safe to proceed.)
Comprehensive Treatment Modalities at Rehab Mechanics
Because cervicogenic headaches are fundamentally a mechanical joint and muscle issue, they respond exceptionally well to mechanical interventions. Pharmaceutical painkillers may temporarily mask the referred pain, but they cannot fix a jammed spinal joint or a weak muscle.
Manual Joint Mobilization
The primary, most immediate intervention is restoring the normal glide and mobility of the C1, C2, and C3 vertebral segments. Physiotherapists utilize highly specific, low-grade manual joint mobilizations.
Techniques such as Sustained Natural Apophyseal Glides (SNAGs), based on the Mulligan concept, involve the therapist applying a gentle, sustained pressure to the specific stiff vertebra while the patient actively rotates their head. By physically unjamming these stiff facet joints and restoring their natural tracking, we instantly reduce the barrage of distress signals being sent into the trigemino-cervical nucleus, effectively "turning off" the headache at its source.
Suboccipital Soft Tissue Release
To address the muscular component, soft tissue therapy is aggressively applied to the upper kinetic chain, including the sternocleidomastoid (SCM), upper trapezius, levator scapulae, and suboccipital muscles.
Physiotherapists often perform a "suboccipital release." The therapist cradles the base of the patient's skull and applies deep, sustained ischemic pressure to the tight muscle bellies just under the occipital ridge. This prolonged pressure starves the contracted muscle of oxygen locally for a brief moment, forcing the tissue to reflexively release. This down-regulates the local nervous system, frees the trapped Greater Occipital Nerve, and rapidly diminishes the throbbing tension at the base of the head.
Corrective Exercises: The Deep Neck Flexors
The final, and most crucial, step for long-term resolution is rebuilding the structural integrity of the neck to prevent the headache from returning next week. If the suboccipital muscles at the back of the neck are overly tight, the opposing muscles at the front of the neck—the Deep Neck Flexors (DNFs), specifically the longus colli and longus capitis—are almost universally weak, overstretched, and neurologically inhibited.
The DNFs are essentially the intrinsic "core muscles" of your cervical spine. Corrective exercise protocols focus heavily on isolating and strengthening these muscles.
The primary intervention is the Cranio-Cervical Flexion exercise (often simplified as a highly specific "chin tuck"). Patients are taught to create a subtle "double chin" without aggressively jamming the head backward or engaging the large superficial neck muscles (like the SCM). This highly controlled micro-movement trains the body to stabilize the heavy skull directly over the shoulders, permanently correcting the forward-head posture that caused the mechanical overload in the first place.
Ergonomic Optimization
Even the best manual therapy will fail if the patient returns to an environment that enforces terrible posture for 8 hours a day. Our physiotherapists provide robust ergonomic coaching, including:
Monitor Height: Ensuring the top third of the computer screen is directly at eye level to prevent constant neck flexion.
The 20-20-20 Rule: Taking a break every 20 minutes to look at an object 20 feet away for 20 seconds. This simple act frequently breaks the sustained isometric tension on the suboccipital muscles.
Thoracic Extension: Utilizing tools like a lumbar roll or a foam roller to keep the mid-back (thoracic spine) upright, as a slumping upper back forces the neck to compensate.
Treatment Phase Breakdown for Cervicogenic Headaches
Rehabilitation PhasePrimary Interventions & ModalitiesClinical Objective
Phase 1: Symptom Down-Regulation
Suboccipital myofascial release, gentle cervical traction, postural offloading, ischemic compression.
Reduce acute nerve irritation, alleviate active headache intensity, and relax hypertonic neck musculature.
Phase 2: Joint Restoration
Specific upper cervical (C1-C3) joint mobilizations (e.g., SNAGs), Thoracic spine manipulation (to improve upper back extension).
Un-jam restricted facet joints, restoring full, pain-free rotation and flexion of the neck, confirmed via the CFRT test.
Phase 3: Motor Control & Stabilization
Deep Neck Flexor (DNF) strengthening, Cranio-Cervical Flexion exercises, Scapular retraction training.
Correct the structural imbalance (Upper Cross Syndrome) and build the localized muscular endurance necessary to hold the heavy skull upright without fatigue.
Phase 4: Functional Resilience & Ergonomics
Dynamic upper body strengthening, multi-planar resistance band exercises, strict desk setup modifications.
Ensure the neck and shoulders can tolerate high-volume daily loading (e.g., 8-hour computer workdays) without triggering a headache relapse.
Author Biography
Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist.
Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:
The content provided in this article is for general educational and informational purposes only and does not constitute formal medical advice. Severe headaches can occasionally be a symptom of serious medical pathology, including vascular issues or high blood pressure. Individual responses to physiotherapy vary, and Rehab Mechanics does not guarantee specific treatment outcomes. An in-person assessment is legally and clinically required to rule out red flags, definitively diagnose the specific cause of head or neck pain, and obtain informed consent before commencing care.
How Does Blood Flow Restriction (BFR) Training Accelerate Injury Recovery? Physiotherapy in Toronto | Rehab Mechanics
How Does Blood Flow Restriction (BFR) Training Accelerate Injury Recovery?
Summary for those on GO (TL;DR):
Blood Flow Restriction (“BFR”) training accelerates injury recovery by utilizing a specialized medical pneumatic tourniquet to partially restrict venous blood flow out of a muscle while maintaining arterial inflow. This creates a highly localized hypoxic (low-oxygen) environment that "tricks" the brain into triggering massive muscle growth and cellular repair using only very light weights (typically 20% - 30% of a patient's One Repetition Maximum). This evidence-based modality is exceptionally effective for the following types of patients:
post-operative patients;
severe tendinopathies, and
joint injuries where heavy lifting is clinically contraindicated.
Key Takeaways:
Primary Clinical Benefit: BFR allows patients to achieve the profound muscle hypertrophy (growth) and strength gains normally associated with heavy weightlifting, but with a fraction of the mechanical stress placed on vulnerable, healing joints or surgical repairs.
Target Demographics: Highly indicated for post-surgical ACL reconstructions, severe osteoarthritis patients, meniscus repairs, and chronic tendinopathies where traditional high-load resistance training provokes severe pain.
Core Modalities: Rehabilitation involves the application of a clinical-grade pneumatic cuff to the upper arm or thigh, followed by a strict protocol of high-repetition, low-load exercises under constant physiological monitoring by a registered physiotherapist.
General Timelines: Measurable increases in muscle cross-sectional area and functional strength are frequently observed within 3 to 6 weeks of consistent BFR integration, significantly preventing the rapid muscle atrophy that typically follows a severe injury.

A physiotherapist at Rehab Mechanics monitoring a patient performing a low-load squat while wearing an FDA-approved pneumatic Blood Flow Restriction (BFR) cuff on the proximal thigh, illustrating a modern clinical modality for accelerated muscle hypertrophy.
Understanding the Physiology and Biomechanics of BFR Training
Historically, the golden rule of muscle physiology and rehabilitation dictated that to build significant muscle mass and restore functional strength, a patient must lift heavy mechanical loads. According to the principles of mechanotransduction, tissues adapt to the specific demands placed upon them. In practice, this meant lifting weights exceeding $70\%$ to $80\%$ of a patient's One Repetition Maximum ($1\text{RM}$) to stimulate structural changes in the muscle fibers.
However, when a patient suffers a severe acute injury (such as a torn ACL, a ruptured Achilles, or a rotator cuff repair) or is dealing with highly reactive joint degeneration (such as severe knee osteoarthritis), placing heavy mechanical loads on the joint is dangerous, structurally compromising, or simply physically impossible due to pain.
The Threat of Arthrogenic Muscle Inhibition (AMI)
This inability to lift heavy weights creates a vicious and rapid clinical cycle. When a joint is injured or undergoes surgery, the body initiates a neurological protective mechanism known as Arthrogenic Muscle Inhibition (AMI). The central nervous system literally "turns off" the muscles surrounding the injured joint to prevent further movement and protect the damaged tissue.
For example, following knee surgery, the quadriceps muscle can begin to visibly atrophy (waste away) and lose significant strength within a matter of days due to AMI. Because the joint hurts, the patient cannot lift heavy weights to reverse the atrophy; because the muscles remain weak, the joint becomes even less stable and more painful.
Blood Flow Restriction (BFR) training offers a profound solution: it chemically bypasses the mechanical requirement for heavy lifting, allowing us to halt muscle atrophy and rebuild the joint's "engine" without straining the damaged "chassis."
The Science of the Ischemic Environment and Metabolic Stress
During a clinical BFR session, a specialized medical-grade pneumatic cuff is placed on the proximal portion of the limb (the uppermost part of the arm near the shoulder, or the upper thigh near the groin).
Calculating Limb Occlusion Pressure (LOP)
Crucially, the goal is not to completely cut off circulation, which would be extremely dangerous. Instead, the BFR device is inflated to a highly precise, individualized pressure known as the Limb Occlusion Pressure (LOP). A physiotherapist utilizes a Doppler ultrasound or the BFR device's internal Bluetooth sensors to determine the exact pressure required to cut off $100\%$ of the blood flow for that specific patient on that specific day.
Once the maximum LOP is found, the cuff pressure is dialed back to a therapeutic range—typically $50\% - 80\%$ LOP for the legs, and $40\% - 50\%$ LOP for the arms. This precise calibration allows oxygenated arterial blood to flow into the working muscle, but strictly restricts the deoxygenated venous blood from flowing out.
Hypoxia and Cellular Swelling
As the patient performs a simple, low-load exercise (e.g., lifting $20\%$ of their max capacity), the working muscle rapidly burns through its local oxygen supply. Because new oxygen is arriving slowly and the waste products cannot escape, the localized tissue environment becomes severely hypoxic (low-oxygen) and highly acidic.
This pooling of blood and the rapid accumulation of metabolic byproducts (such as lactic acid and hydrogen ions) creates profound metabolic stress. Additionally, the pooling blood causes extreme cellular swelling, which physically stretches the walls of the muscle cells. The body's central nervous system perceives this intense metabolic stress and cellular swelling as a massive physiological emergency—as if the patient is lifting a monolithic weight—and it reacts by initiating a massive repair cascade.
Henneman’s Size Principle and Systemic Hormonal Release
To understand why BFR builds muscle so effectively with light weights, we must look at how the brain communicates with muscles. Henneman’s Size Principle dictates that the nervous system recruits muscle fibers in a specific sequence, starting with the smallest, most fatigue-resistant fibers first, and only calling upon the largest, most powerful fibers when absolutely necessary.
Under normal circumstances, your body relies on Type I (slow-twitch, endurance) muscle fibers for light tasks like walking or lifting light objects. Because these fibers rely heavily on oxygen, they can work for a long time without fatiguing. To force the body to recruit the massive Type II (fast-twitch) muscle fibers—the ones responsible for explosive strength and significant muscle growth—you typically have to lift a very heavy weight that overwhelms the Type I fibers.
The Hypoxic Hack
BFR completely short-circuits this neurological rule. Because the BFR cuff has created a low-oxygen environment, the oxygen-dependent Type I fibers exhaust and fail almost immediately. Panic-stricken, the central nervous system is forced to prematurely recruit the massive Type II fast-twitch fibers just to continue moving the very light weight.
Simultaneously, the intense buildup of lactic acid and the firing of these Type II fibers triggers the anterior pituitary gland in the brain to release a massive systemic surge of Human Growth Hormone (HGH) and Insulin-like Growth Factor-1 (IGF-1). These powerful anabolic hormones are flushed through the entire bloodstream, accelerating collagen synthesis, bone healing, and massive muscle hypertrophy. Through BFR, we achieve the systemic biological healing response of Olympic weightlifting while mechanically protecting the injured local tissue.
Clinical Assessment: Medical vs. Recreational BFR
It is vital to distinguish clinical BFR therapy from recreational "gym-bro" occlusion training. Wrapping a knee wrap or an elastic band tightly around a limb at the gym is highly dangerous, as it offers no way to measure arterial inflow, risking severe nerve damage or complete arterial occlusion.
At our 68 Abell Street facility in Toronto, we utilize only FDA and Health Canada-approved medical pneumatic tourniquets that continuously monitor and adjust pressure. Furthermore, an exhaustive in-person physical assessment and medical history review are legally and clinically required before initiating BFR therapy.
Because BFR temporarily alters localized blood pressure and cardiovascular demand, a physiotherapist must rule out absolute contraindications, which include:
Deep Vein Thrombosis (DVT): A history of blood clots, endothelial dysfunction, or severe vascular compromise.
Severe Hypertension: Unmanaged or highly volatile high blood pressure.
Pregnancy: BFR is strictly contraindicated during pregnancy due to altered hemodynamics.
Active Cancer or Tumor: Within the affected limb or lymphatic system.
Severe Peripheral Neuropathy: Loss of sensation that would prevent the patient from providing accurate feedback on cuff comfort and nerve compression.
Only after a precise diagnosis is established, absolute contraindications are ruled out, and informed patient consent is obtained detailing the risks and physiological sensations of the treatment, will BFR interventions commence.
Comprehensive Treatment Modalities Utilizing BFR
Rehabilitation using BFR at Rehab Mechanics is never a standalone treatment; it is a highly specialized tool integrated into a broader, multimodal recovery framework.
The Standard Clinical Protocol (30-15-15-15)
The clinical application of BFR relies on high-repetition, short-rest protocols to intentionally maximize the accumulation of metabolites. Once the cuff is inflated to the precise therapeutic pressure, the patient begins a highly specific, grueling set structure using only $20\% - 30\%$ of their $1\text{RM}$:
Set 1: 30 repetitions (This initial high-rep set acts as the "primer" to rapidly deplete local oxygen and initiate the lactic acid burn).
Rest: 30 seconds (Crucially, the cuff remains inflated during the rest period to trap the metabolites and prevent oxygen from flushing the muscle).
Set 2: 15 repetitions.
Rest: 30 seconds.
Set 3: 15 repetitions.
Rest: 30 seconds.
Set 4: 15 repetitions (Totaling 75 repetitions).
The cuff is immediately deflated after the final repetition, allowing a massive rush of highly oxygenated, nutrient-dense blood to flood the tissue (hyperemia).
Condition-Specific Applications
This protocol is utilized with basic, joint-sparing exercises tailored to the specific injury:
Post-Operative ACL: Simple straight-leg raises or isometric quad sets to reverse Arthrogenic Muscle Inhibition without straining the new graft.
Knee Osteoarthritis: BFR applied during stationary cycling (10-15 minutes of low-intensity biking) to build quad strength while offloading the bone-on-bone joint.
Achilles Tendinopathy: Seated calf raises with BFR to safely load the calf complex and tendon without requiring heavy, painful standing weights.
Integration with Manual Therapy
BFR optimally pairs with targeted soft tissue therapy and joint mobilizations. While BFR aggressively rebuilds the muscular "engine," manual therapy is utilized to ensure the "chassis" (the joint capsule and fascial tissue) moves freely. Restoring normal joint arthrokinematics through manual mobilization ensures that the newly acquired muscle strength is applied efficiently, safely, and smoothly through a full, pain-free range of motion.
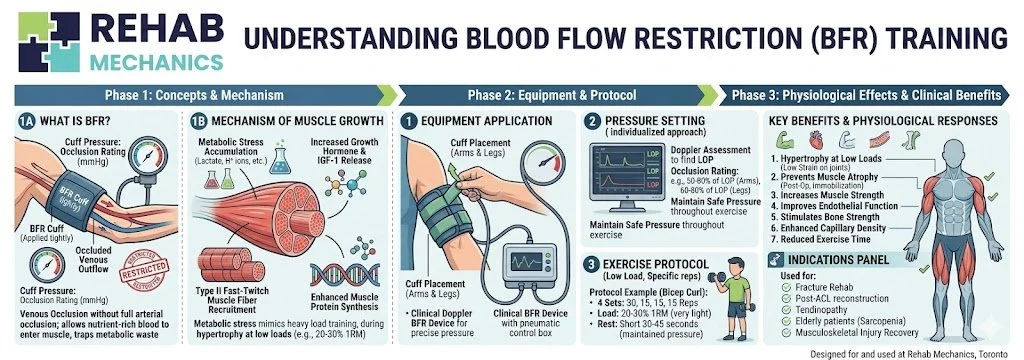
Our homemade curated diagram for BFR
Phase Breakdown for BFR Rehabilitation
Rehabilitation PhaseBFR Application & LoadingClinical Objective
Phase 1: Post-Acute Atrophy Prevention
Isometric holds and gravity-eliminated movements with BFR. Cuff pressure is moderate.
Prevent severe post-surgical or post-injury muscle wasting (AMI) without loading the damaged joint.
Phase 2: Hypertrophy & Cellular Repair
Isotonic movements (e.g., leg extensions, bicep curls) at $20\%-30\%$ $1\text{RM}$. Standard 75-rep protocol.
Induce profound metabolic stress, stimulate early Type II fiber recruitment, and trigger systemic growth hormone release.
Phase 3: Mechanical Loading Transition
Deflating the cuff; transitioning to heavier, traditional resistance training ($60\%+$ $1\text{RM}$).
Begin conditioning the tendons, ligaments, and bones to tolerate heavy, real-world mechanical stress.
Phase 4: Functional Return
Plyometrics, heavy compound lifts, and multi-joint occupational simulations without BFR.
Restore full, unrestricted athletic or occupational capacity and dynamic stability.
Author Biography
Written by Sanjay Attwala (BSC, MSC, RPT), Registered Physiotherapist.
Sanjay Attwala manages patient care at Rehab Mechanics (S. Attwala Physiotherapy Professional Corporation) located at 68 Abell Street, Toronto. He is in good standing with the College of Physiotherapists of Ontario (CPO). Learn more about our highly qualified clinical team here.
Medical Disclaimer:
The content provided in this article is for general educational and informational purposes only and does not constitute formal medical advice. Individual physiological responses to physiotherapy and vascular therapies vary significantly. Rehab Mechanics does not guarantee specific treatment outcomes. An in-person assessment is legally and clinically required to definitively evaluate cardiovascular suitability, rule out vascular contraindications, develop a treatment plan, and obtain informed consent before commencing BFR therapy.