Should I Seek Conservative Orthopedic Services Before Joint Surgery?
Yes. Clinical guidelines mandate attempting conservative orthopedic services before committing to joint surgery. Advanced physical therapy addresses the biomechanical deficits causing joint degradation, often restoring pain-free function and successfully delaying or completely eliminating the need for invasive surgical interventions.
The Rush to the Operating Room
When facing severe, chronic pain in the knee, hip, or shoulder, many patients in Toronto are quickly funneled into the surgical pipeline. A scan reveals a torn meniscus, a frayed labrum, or moderate osteoarthritis, and the immediate conclusion is that the joint must be "cleaned out" or completely replaced.
While orthopedic surgery is sometimes unavoidable and incredibly effective for massive structural trauma, it should rarely be the first line of defense for degenerative or repetitive strain injuries.
When you search for "Toronto orthopedic services" or "prime medical centre physical therapy," you are seeking a complete spectrum of care. At Rehab Mechanics, located inside the Prime Medical Centre, we operate on the front lines of conservative orthopedic management. Our goal is to exhaust every possible biomechanical and physical intervention to heal your joint naturally, saving you from the risks, prolonged downtime, and irreversible anatomical changes of surgery.
Structural Analysis: Anatomy vs. Biomechanics
To understand why conservative orthopedic physiotherapy can often replace surgery, we must analyze the difference between anatomical damage and biomechanical function.
The "Incidental Finding" Phenomenon
Magnetic Resonance Imaging (MRI) is a powerful tool, but it is frequently misleading.
Asymptomatic Tears: Extensive medical studies show that if you MRI the shoulders or knees of 100 healthy adults with zero pain, a massive percentage of them will have rotator cuff tears, bulging discs, or meniscal fraying.
The Reality: Structural imperfections are a normal part of human aging. Just because a scan shows a tear does not mean that tear is the actual source of your pain.
The Functional Deficit
Surgery focuses purely on altering anatomy (cutting away a torn meniscus or shaving a bone spur). Conservative orthopedic therapy focuses on improving biomechanics (how the joint handles force).
The Knee Osteoarthritis Example
A patient presents with severe knee pain and an X-ray showing mild-to-moderate osteoarthritis (cartilage loss).
The Surgical Approach: A surgeon might suggest a partial knee replacement or an arthroscopic debridement.
The Biomechanical Approach: A physiotherapist will look at why that specific part of the knee is wearing away. They often find profound weakness in the gluteal muscles and extreme stiffness in the ankle joint.
Restoring the Shock Absorbers
By vigorously strengthening the quadriceps, hamstrings, and glutes, the physiotherapist builds a massive muscular "brace" around the knee. These muscles begin absorbing the shock of walking before it ever hits the joint. Even though the cartilage is still thin, the pain disappears because the mechanical load has been successfully transferred to the muscles. The surgery is successfully avoided.
Primary Source Proof: Conservative Orthopedics
Leading orthopedic surgical associations now strongly recommend structured, supervised physical therapy as the first-line treatment for a vast array of joint pathologies prior to surgical consultation.
Download Clinical Efficacy PDF: The Efficacy of Conservative Physical Therapy Versus Surgical Intervention in Degenerative Meniscal Tears and Osteoarthritis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for orthopedic management.
The Prime Medical Centre Integrated Advantage
Providing elite-level conservative orthopedic care requires an interdisciplinary environment. This is the distinct advantage of receiving treatment at Rehab Mechanics within the Prime Medical Centre.
1. Interdisciplinary Medical Support
If a joint is too acutely inflamed to tolerate physical therapy, we do not simply give up and send you to a surgeon.
Pharmacological Windows: We collaborate instantly with the on-site medical doctors. They can administer targeted intra-articular corticosteroid or viscosupplementation injections.
The Synergy: This medical intervention drops the pain threshold rapidly, creating a critical "window of opportunity" where our physiotherapists can aggressively strengthen the joint to ensure the pain does not return when the injection wears off.
2. Advanced Physical Modalities
We utilize technology designed to accelerate biological healing without a scalpel.
Extracorporeal Shockwave Therapy (ESWT): A highly effective, non-invasive treatment for chronic tendinopathies (like calcific rotator cuff tendinitis or severe plantar fasciitis) that stimulates profound cellular regeneration and breaks down calcified tissue.
3. Pre-Habilitation (If Surgery is Required)
If you ultimately do require a total joint replacement or ACL reconstruction, conservative therapy is still mandatory.
Building the Baseline: Participating in a "Pre-Hab" program strengthens the surrounding musculature before you go into the operating room.
The Outcome: Patients who undergo pre-habilitation experience drastically reduced post-operative complication rates and return to full function weeks faster than those who do not.
Exhaust Your Conservative Options
Do not let an MRI dictate a rush to the operating table. Empower yourself by exploring the vast potential of biomechanical correction and targeted strengthening.
Book a comprehensive orthopedic assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, providing integrated healthcare in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.



Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Can Treatment for Poor Movement Mechanics Permanently Fix Chronic Joint Pain?
Yes. Chronic joint pain is rarely random; it is the physical consequence of poor movement mechanics. By identifying and correcting the specific compensatory patterns that overload your tissues, biomechanical physiotherapy permanently resolves the root cause of your chronic pain.
The Illusion of Random Injury
"I just bent over to tie my shoe, and my back went out." "I was just jogging on a flat path when my knee flared up."
At Rehab Mechanics, we hear these stories every day. For active residents of Queen West and Trinity Bellwoods, injuries often feel like sudden, random acts of misfortune. However, the human body is an incredibly resilient machine. Ligaments, tendons, and discs do not simply snap under normal, low-level loads like bending over or jogging.
When you search for "treatment for poor movement mechanics" or "remedial mechanics," you are tapping into the core philosophy of advanced physical therapy: the injury you felt today is actually the culmination of thousands of faulty movements you made over the last six months.
If you do not fix the underlying movement mechanics, the injury will inevitably return, regardless of how much ice, rest, or massage you apply. True healing requires a complete audit of how your nervous system coordinates the kinetic chain.
Structural Analysis: The Danger of Compensatory Patterns
To understand why fixing movement mechanics is the only permanent cure for joint pain, we must perform a deep dive into the concept of neurological compensation.
The Rule of the Kinetic Chain
Your body is a linked system of joints that alternate between requiring mobility and requiring stability.
Your ankle needs mobility.
Your knee needs stability.
Your hip needs mobility.
Your lumbar spine needs stability.
The Breakdown: Neurological Compensation
When one joint fails to do its job, the nervous system instantly forces the adjacent joint to do the work instead. This is called a "compensatory pattern," and it is the root cause of almost all non-traumatic orthopedic pain.
The Glute-Hamstring Shift
Consider the action of running or walking. Your gluteus maximus (your primary hip extensor) should be the main engine driving you forward.
The Inhibition: Due to hours of sitting at a desk, your hip flexors become tight, which neurologically "shuts off" or inhibits your glute muscles.
The Compensation: Your brain still needs you to walk, so it recruits your hamstrings and your lower back muscles to do the job of the glutes.
The Tissue Failure: Hamstrings and spinal erectors are not designed to be primary propulsive engines. Because they are overworked, they become chronically tight, form severe trigger points, and eventually tear.
The Treatment Fallacy
If you go to a standard clinic, they will massage your tight hamstrings and heat your sore lower back. This provides relief for exactly one day. The moment you stand up and walk with the same poor movement mechanics, the hamstrings are immediately overloaded again.
Primary Source Proof: Kinematic Rehabilitation
Sports medicine literature overwhelmingly supports kinematic (movement-based) interventions over passive treatments for long-term resolution of musculoskeletal pathologies.
Download Clinical Efficacy PDF: The Role of Biomechanical Assessment and Kinematic Correction in Chronic Musculoskeletal Pain (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for movement science.
The Rehab Mechanics Corrective Protocol
We do not treat the victim; we treat the culprit. Repairing poor movement mechanics requires a rigorous, phased approach to rewire your nervous system.
Phase 1: The Functional Movement Screen (FMS)
Before we treat you, we must map your movement.
Overhead Squat Assessment: This single movement reveals bilateral imbalances, ankle mobility deficits, and core instability instantly.
Single-Leg Loading: Watching how you balance on one leg tells us exactly how your gluteus medius is (or isn't) stabilizing your pelvis.
Gait Analysis: Breaking down your walking or running stride to identify overpronation, early heel rise, or pelvic drop.
Phase 2: Restoring Tissue Quality and Range of Motion
We must clear the physical roadblocks before the brain can learn new movements.
Myofascial Release: Utilizing advanced manual therapy to break down the dense fascial adhesions that are physically pulling your joints out of alignment.
Joint Mobilization: Unlocking stiff joint capsules (like the ankle or thoracic spine) to ensure the limb actually has the capacity to move through a full, healthy range.
Phase 3: Neuromuscular Re-education
This is the most critical phase. We must teach your brain the correct way to move.
Isolated Motor Control: Prescribing micro-movements to "wake up" dormant muscles without allowing the larger, compensatory muscles to take over.
Progressive Integration: Once the muscle fires correctly in isolation, we integrate it into compound movements (like lunges or deadlifts), ensuring the entire kinetic chain operates synchronously.
High-Load Resilience: Finally, we load the movement with heavy resistance to permanently cement the new motor pattern into your nervous system, ensuring you can lift, run, and live safely.
Rebuild Your Body's Foundation
Do not settle for a life of temporary fixes and recurring injuries. By addressing your foundational movement mechanics, you can eliminate the hidden forces destroying your joints.
Book a comprehensive biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.

Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Correcting Your Spinal Mechanics Reverse Degenerative Disc Disease?
Yes. While age-related disc changes are natural, correcting your spinal mechanics prevents these changes from causing pain. By restoring segmental mobility and strengthening deep core stabilizers, physiotherapy eliminates the abnormal compression forces that trigger severe nerve irritation and chronic back pain.
The Misunderstood Diagnosis of "Wear and Tear"
If you are a professional working in downtown Toronto, there is a high probability that you or a colleague has been diagnosed with Degenerative Disc Disease (DDD). When patients receive this diagnosis after an MRI or X-ray, they often feel as though they have been handed a life sentence of chronic pain. The imagery of "crumbling discs" and "bone on bone" friction creates immense fear, leading many to stop exercising, stop lifting, and live in constant apprehension.
However, the medical community's understanding of spinal health has evolved drastically. When Queen West residents search for solutions related to "spinal mechanics" or "body mechanics physiotherapy," they are looking for the modern, evidence-based truth: structural changes on an MRI do not automatically equal pain.
At Rehab Mechanics, located inside the Prime Medical Centre, we teach our patients that spinal degeneration is often just "wrinkles on the inside"—a normal part of aging. The pain you are experiencing is rarely from the degeneration itself; it is the result of faulty spinal mechanics amplifying the stress on those aging tissues. Fix the mechanics, and you fix the pain.
Structural Analysis: The Physics of the Human Spine
To understand how physical therapy resolves severe back pain, we must perform a biomechanical analysis of the lumbar spine and how it responds to mechanical load.
The Intervertebral Disc as a Shock Absorber
Your spinal discs are highly sophisticated, fluid-filled shock absorbers situated between your vertebrae.
The Nucleus Pulposus: The jelly-like center that distributes hydraulic pressure.
The Annulus Fibrosus: The tough, fibrous outer rings that contain the center and provide rotational stability.
The Breakdown of Spinal Mechanics
Discs do not simply "wear out" evenly. They fail when they are subjected to prolonged, unnatural mechanical forces, typically caused by modern, sedentary urban lifestyles.
The Flexion Overload
Sitting at a desk for eight hours a day places the lumbar spine into sustained flexion (rounding forward).
The Hydraulic Shift: This rounded posture squeezes the front of the discs, forcing the fluid in the nucleus backward against the posterior annulus wall.
Creep and Tissue Deformation: Over time, this constant backward pressure permanently stretches the posterior ligaments and weakens the disc wall.
Loss of Segmental Independence
When one part of the spine becomes stiff (often the thoracic mid-back), the body must find that lost movement somewhere else.
The Hinge Effect
If your mid-back cannot extend or rotate, your lower back (lumbar spine) is forced to hyper-compensate. Instead of movement being distributed evenly across 24 vertebrae, all the rotational sheer force is concentrated onto one or two specific discs (usually L4-L5 or L5-S1). This specific, repetitive mechanical overload is what causes the disc to bulge, inflame the surrounding nerve roots, and trigger sciatica.
Primary Source Proof: Biomechanics of the Spine
Clinical orthopedic research unequivocally demonstrates that active spinal stabilization and movement correction are vastly superior to passive rest or early surgical intervention for managing degenerative disc pathologies.
Download Clinical Efficacy PDF: The Efficacy of Motor Control Exercise and Biomechanical Correction for Lumbar Degenerative Disc Disease (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for spinal rehabilitation.
The Rehab Mechanics Spinal Protocol
Treating discogenic pathology requires absolute precision. We do not apply generic stretches; we completely overhaul the way your spine handles gravity.
Phase 1: Mechanical Decompression and Centralization
Our immediate goal is to remove the pressure from the irritated nerve root.
Directional Preference Therapy: Utilizing the McKenzie Method to find the specific movement plane (usually extension) that physically pushes the bulging disc material away from the spinal cord.
Manual Traction: Applying gentle, targeted distraction to the lumbar segments to create negative pressure within the disc, encouraging rehydration and cellular healing.
Phase 2: Restoring Regional Arthrokinematics
We must fix the stiff joints above and below the injury to stop the "hinge effect."
Thoracic Spine Mobilization: Unlocking the stiff mid-back so the lumbar spine no longer has to over-rotate during daily movements.
Hip Joint Release: Tight hip flexors (psoas) physically pull the lumbar spine into a deep, painful arch. We utilize deep myofascial release to restore pelvic neutrality.
Phase 3: Deep Neuromuscular Fortification
To ensure the pain does not return the moment you sit back at your desk, we must build a muscular corset around your spine.
Transversus Abdominis Activation: This is your body's internal weight belt. We use biofeedback to train your brain to fire this deep core muscle instantly before you move.
Multifidus Strengthening: The tiny muscles that directly stabilize the vertebrae. Rebuilding these muscles prevents the micro-stuttering motions that cause acute back spasms.
Load Tolerance Training: We progressively introduce heavy, safe lifting mechanics (like kettlebell deadlifts or loaded carries) to prove to your nervous system that your spine is strong, resilient, and capable of handling life in Toronto.
Take Control of Your Spinal Health
A diagnosis of degenerative disc disease is not the end of your active life; it is simply a signal that your spinal mechanics need a professional upgrade.
Book a comprehensive spinal biomechanics assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Stop the Progression of Degenerative Disc Disease?
Yes. Physiotherapy can stop the progression of Degenerative Disc Disease (DDD) by restoring spinal mobility, strengthening deep core stabilizers, and correcting the postural forces that accelerate disc decay. While structural wear is part of aging, active rehabilitation prevents chronic pain and structural collapse.
The Reality of Spinal Aging in a Desk-Bound Culture
If you are a professional living and working in Toronto, you likely understand the creeping, persistent ache of lower back pain. Many individuals in their 30s, 40s, and 50s are diagnosed with Degenerative Disc Disease (DDD) after a scan reveals wear on their spinal discs. This diagnosis is often delivered in a way that suggests the spine is "rusting" and there is nothing to be done but manage the decline.
At Rehab Mechanics, we reject this defeatist approach. DDD is not an inevitable decline into disability; it is a structural challenge that responds exceptionally well to biomechanical intervention. By understanding how your spinal discs live, grow, and fail, we can implement strategies that keep your spine mobile and robust for decades, regardless of what your MRI report suggests.
Structural Analysis: The Life Cycle of a Spinal Disc
To manage DDD, we must first understand the physiology of the intervertebral disc. It is not merely a static spacer between vertebrae; it is a dynamic, living tissue that requires constant mechanical stimulation to stay healthy.
The Anatomy of the Disc
The disc has two main parts:
The Nucleus Pulposus: A soft, gel-like center that is roughly 80-90% water. This center acts as your hydraulic shock absorber.
The Annulus Fibrosus: A tough, multi-layered "tire" of collagen fibers that holds the gel in place.
The Process of Degeneration
Degeneration is the process of the disc losing its water content and height.
Dehydration: Over time, the gel-like center dries out, losing its ability to absorb impact.
Fissures and Tears: As the disc loses height, the outer ring (annulus) begins to buckle, develop small cracks, and lose its structural integrity.
Vertebral Overload: When the disc flattens, the weight of your upper body is no longer distributed evenly. It shifts onto the tiny facet joints at the back of the spine, leading to osteoarthritis and bone spurs.
Postural Drivers of Acceleration
Sustained Compression: Sitting for eight hours a day prevents the disc from "pumping" (the process of fluid moving in and out of the disc during movement).
The "Dead" Disc: If you don't move, you don't nourish the disc. This is why sedentary lifestyles accelerate DDD at a cellular level.
Primary Source Proof: Non-Operative Management
Orthopedic research consistently shows that active rehabilitation is the first-line treatment for managing DDD and preventing the need for spinal fusion surgery.
Download Clinical Efficacy PDF: The Role of Active Loading and Rehabilitation in the Management of Degenerative Disc Disease (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for spinal care.
The Rehab Mechanics DDD Treatment Protocol
We treat DDD by optimizing the mechanical environment of your spine to favor tissue health over further degradation.
1. Reversing the Compression Cycle
We must get fluid moving into the discs again.
Manual Traction: Gently separating the vertebrae to create a vacuum effect, drawing nutrients and fluid back into the dehydrated disc space.
Joint Mobilization: Restoring motion to restricted spinal segments to ensure that loading is shared across the entire spine, rather than concentrated on one failing disc.
2. Deep Core Neuromuscular Re-education
If your core is weak, your spine is forced to take the impact of every single step.
Transversus Abdominis (TvA) Training: Rebuilding the deepest core muscle that acts as your biological weight belt.
Multifidus Strengthening: The multifidus is the deepest muscle along your spine. We use specific, isolated holds to fire these muscles, which physically hold the vertebrae together and reduce pressure on the intervertebral discs.
3. Postural Endurance Training
You cannot out-rehab 8 hours of slouching. We retrain your body to sit, stand, and move efficiently.
Thoracic Extension: Reversing the slouching habit by actively lengthening the mid-back and opening the ribcage.
Ergonomic Integration: Modifying your workstation height, chair lumbar support, and monitor placement to maintain a neutral spinal curve throughout your workday.
Take Control of Your Spinal Health
Degenerative Disc Disease is manageable, and its symptoms are reversible with the right biomechanical approach. Stop waiting for your spine to fail and start building its resilience today.
Book a comprehensive spinal assessment at our clinic, conveniently located inside the Prime Medical Centre at 68 Abell Street.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Can Physiotherapy Fix Pinched Nerves and Radiating Arm Pain?
Yes. Physiotherapy can completely resolve pinched nerves (cervical radiculopathy). A specialized protocol of cervical joint mobilization, deep neck flexor strengthening, and postural correction physically decompresses the cervical spine, eliminating radiating arm pain and preventing permanent disc damage.
The Epidemic of Forward Head Posture in Toronto
Walk into any coffee shop in Queen West, jump on the King streetcar, or look around a downtown creative agency, and you will see the same physical posture: the deep, sustained spinal slump. We are a culture permanently hunched over smartphones, tablets, and multiple monitors.
This modern posture is colloquially known as "Tech Neck." While a stiff neck might seem like a minor annoyance, the long-term biomechanical consequences are severe. When the neck is chronically pushed forward out of its natural alignment, it creates massive structural shearing forces on the delicate cervical vertebrae.
Eventually, this passive stress leads to a catastrophic tissue failure. The pain stops being a dull ache in the neck and suddenly morphs into a terrifying, sharp, burning sensation radiating down your shoulder blade, triceps, and all the way into your fingers. This is cervical radiculopathy—a pinched nerve in the neck. At Rehab Mechanics, we specialize in diagnosing and structurally correcting complex spinal and discogenic pathology without relying on heavy painkillers or invasive injections.
Structural Analysis of the Cervical Spine
To successfully treat radiating arm pain, we cannot just massage the shoulder. We must perform a rigorous biomechanical analysis of the cervical spine to locate exactly where the nerve is being crushed.
The Physics of the Heavy Head
The human head weighs approximately 10 to 12 pounds when perfectly balanced on top of the spine.
The Leverage Effect: For every single inch your head drifts forward past your shoulders to stare at a screen, the mechanical load on your neck muscles and joints essentially doubles.
Chronic Overload: A head jutting three inches forward exerts roughly 40 pounds of pressure on the lower cervical spine. Your neck was not engineered to hold a bowling ball at an angle for eight hours a day.
The Anatomy of a Cervical Disc Bulge
The seven vertebrae of your neck (C1 through C7) are separated by intervertebral discs, which act as crucial shock absorbers.
The Annulus and Nucleus: These discs have a tough, fibrous outer ring (annulus fibrosus) and a soft, gel-like center (nucleus pulposus).
The Tearing Process: The chronic pressure of "Tech Neck" unevenly crushes the front of the discs, slowly pushing the gel-like center backward toward the spinal cord. Over time, the outer ring tears, and the gel bulges outward.
Cervical Radiculopathy (The Pinched Nerve)
The space where the nerve roots exit the spine to travel down your arm is incredibly narrow.
Mechanical Strangulation: When a cervical disc bulges backward, it physically invades this narrow space, crushing the nerve root against the bone.
The Symptom Pathway: Because these nerves wire your entire upper extremity, compression at the neck causes severe, shooting pain, numbness, tingling, and profound muscular weakness deep in your arm, forearm, or hand.

The Physiotherapy Intervention: Decompressing the Spine
At Rehab Mechanics, we reject passive treatments like hot packs for neurological injuries. We utilize a highly aggressive, mechanically driven protocol to centralize the pain (draw it out of the arm and back up to the neck) and retract the bulging disc.
1. Directional Preference Therapy (The McKenzie Method)
Our immediate clinical priority is stopping the nerve compression.
Cervical Retraction: We utilize specific, repeated movements—often cervical retractions (creating a "double chin") and controlled extensions—to physically alter the pressure gradient inside the disc. This mechanical pumping action draws the bulging gel back toward the center, taking it off the nerve root.
Postural Taping: Applying rigid kinesiology tape to the mid-back to act as a physical reminder, preventing you from slumping forward and re-herniating the disc between sessions.
2. Advanced Manual Therapy and Traction
The muscles surrounding a pinched nerve will instantly go into a massive, protective spasm, locking the neck into a rigid block.
Cervical Joint Mobilization: Our Registered Physiotherapists use precise, hands-on glides to free up the stiffened facet joints of the neck, restoring rotational capacity.
Manual Cervical Traction: Gently pulling the head upward to physically separate the cervical vertebrae, instantly opening up the nerve spaces (foramen) and providing immediate, profound relief from the radiating arm pain.
3. Deep Neck Flexor and Scapular Stabilization
Once the disc is retracted and the nerve is free, we must build the muscular scaffolding necessary to hold your head upright permanently.
Neuromuscular Re-education: The deep muscles at the front of your neck (longus colli) are usually entirely shut down by tech neck. We prescribe specific, tiny nodding exercises to wake these crucial stabilizers up.
Thoracic Extension: Strengthening the mid-back (rhomboids and lower trapezius) to pull the shoulder blades down and back, creating a solid, stable foundation for the neck to rest upon.
Primary Source Proof
Extensive orthopedic research and clinical guidelines confirm that multimodal physiotherapy—combining mechanical traction, cervical mobilization, and deep flexor strengthening—is the most effective conservative intervention for resolving cervical radiculopathy, frequently outperforming surgical decompression in long-term outcomes.
Download Clinical Evidence: The Efficacy of Conservative Physiotherapy in the Management of Cervical Radiculopathy (Open Access Medical Review)
Stop Ignoring Your Neck Pain
A stiff neck is a warning sign; radiating arm pain is a structural emergency. Do not wait for a bulging disc to cause permanent nerve damage or muscular atrophy in your arm. Expert, targeted physical rehabilitation can decompress your spine, reverse the damage of tech neck, and restore full feeling and strength to your upper body.
Book your comprehensive spinal assessment today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Prevent Knee Replacement Surgery for Osteoarthritis?
Yes. Evidence-based physiotherapy significantly delays or prevents knee replacement surgery. By strengthening the quadriceps, improving joint mobility, and utilizing advanced modalities, physiotherapy reduces joint friction, manages chronic inflammation, and restores pain-free mobility in osteoarthritic knees.
Re-Thinking "Bone on Bone" Pain
A diagnosis of knee osteoarthritis (OA) often sounds like a definitive, surgical sentence. Patients are frequently told their knee is "bone on bone" and that a total knee replacement is the only eventual solution. This rhetoric causes immense fear, leading patients to stop moving entirely to "save" whatever cartilage they have left.
This is the worst possible strategy. Total rest accelerates the degradation of the joint.
At Rehab Mechanics, we work directly alongside physicians at the Prime Medical Centre on Abell Street to co-manage osteoarthritis. Our clinical data and daily practice prove that the severity of cartilage loss on an X-ray does not accurately dictate the amount of pain a patient will experience. By improving the biomechanical support system around the joint, physiotherapy can drastically reduce OA pain, restore function, and push the need for surgery back by years—or eliminate it entirely.
Structural Analysis: The Mechanics of Osteoarthritis
To understand how physiotherapy fights osteoarthritis, we must first understand the mechanical environment of the knee joint.
The Pathology of OA
Osteoarthritis is not merely "wear and tear." It is an active, whole-joint disease characterized by the breakdown of articular cartilage, changes to the underlying bone, and chronic inflammation of the synovial membrane.
Cartilage Degradation: The smooth, slippery cartilage that coats the ends of the femur and tibia thins out, increasing friction.
Osteophyte Formation: The body attempts to stabilize the failing joint by growing bone spurs (osteophytes), which can restrict movement and cause pinching pain.
Synovitis: The joint lining becomes inflamed, producing excess fluid (swelling) and releasing pain-mediating chemicals.
The Biomechanical Solution: Muscular Offloading
If the cartilage padding is gone, how can physiotherapy stop the pain? The answer lies in the muscles.
The Role of the Quadriceps
Your quadriceps (front thigh muscles) are the primary shock absorbers for your knee. They act as a massive braking system every time you take a step, absorbing up to 70% of the impact forces before they ever reach the knee joint.
The Cycle of Weakness
When the knee hurts, the brain subconsciously inhibits the quadriceps to prevent you from using the leg. The muscle rapidly shrinks (atrophies).
Once the quad is weak, 100% of the walking impact bypasses the muscle and slams directly into the arthritic, degraded bone. This causes more pain, which causes more weakness, creating a devastating downward spiral. Physiotherapy breaks this cycle.
Primary Source Proof: Non-Operative Efficacy

Major international orthopedic guidelines strongly mandate that comprehensive physiotherapy and exercise must be exhausted before surgical intervention is considered for knee OA.
Download Clinical Efficacy PDF: The Efficacy of Land-Based Exercise on Pain and Physical Function in Knee Osteoarthritis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for orthopedic rehabilitation.
The Interdisciplinary Protocol at Prime Medical Centre
Treating a degenerative disease requires a highly coordinated approach. Because we operate within the Prime Medical Centre, we seamlessly blend medical management with aggressive physical rehabilitation.
1. Medical Inflammation Management
Before we can strengthen the joint, we must lower the acute pain threshold.
Physician Co-Management: The medical doctors on-site may utilize targeted NSAIDs or administer intra-articular injections (such as corticosteroids or hyaluronic acid/viscosupplementation) to dramatically reduce synovial inflammation.
The Window of Opportunity: These injections do not cure the disease, but they create a critical 3-to-6 month "window of opportunity" where the knee is pain-free enough to tolerate intense physiotherapy.
2. Joint Mobilization and Swelling Reduction
Our physiotherapists begin by restoring the mechanical space in the joint.
Manual Traction: Gently pulling the joint surfaces apart to encourage the flow of synovial fluid, which lubricates the joint and nourishes the remaining cartilage.
Knee Extension Restoration: A knee that cannot straighten fully causes severe limping and rapid joint wear. We use targeted manual therapy to break down capsule stiffness and restore full extension.
3. Progressive Load and Strength Training
This is the long-term cure for OA pain. We must build a muscular brace around the bone.
Isolated Quadriceps Loading: Utilizing closed-kinetic-chain exercises (like leg presses, wall sits, and step-ups) to rebuild the quad muscle without applying shearing force to the kneecap.
Gluteal and Hip Strengthening: The hip controls the alignment of the knee. By strengthening the gluteus medius, we prevent the knee from caving inward (valgus stress), which protects the medial compartment of the knee where OA usually strikes hardest.
Proprioceptive Training: Improving balance to ensure the muscles fire instantly to protect the joint during unexpected missteps on uneven Toronto sidewalks.
Take Control of Your Joint Health
A diagnosis of osteoarthritis is not a mandate to stop living an active life. Through targeted biomechanical strengthening and interdisciplinary medical care, you can reclaim your mobility and delay or prevent the need for joint replacement surgery.
Book a comprehensive knee assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Do I Always Need Physiotherapy for a Rolled Ankle?
Yes. Ignoring a rolled ankle leads to chronic instability and recurring injuries. Physiotherapy restores torn ligaments, rebuilds essential proprioception, and strengthens the surrounding ankle musculature to prevent long-term biomechanical dysfunction and early-onset osteoarthritis.
The Trap of the "Simple" Sprain
"It is just a rolled ankle. I'll walk it off." This is one of the most common and dangerous misconceptions in sports medicine. Whether you rolled it stepping off a curb on Queen Street West, playing a recreational soccer match, or slipping on an icy Toronto sidewalk, an ankle sprain is a severe structural injury.
When patients fail to rehabilitate an ankle sprain, the initial pain and swelling usually subside after a few weeks. However, the underlying mechanical damage remains. Without targeted physiotherapy, the ankle joint heals loosely, leading to a condition known as Chronic Ankle Instability (CAI).
At Rehab Mechanics, we frequently see patients who suffer from recurring ankle sprains, chronic tightness, and early degenerative joint changes simply because they neglected to rehabilitate their very first sprain properly.
Structural Analysis: The Anatomy of a Sprain
To understand why professional rehabilitation is mandatory, we must perform a biomechanical analysis of what exactly happens when an ankle "rolls."
The Lateral Ligament Complex
The vast majority (over 80%) of ankle sprains are "inversion" sprains, meaning the foot rolls inward. This violent motion places catastrophic stress on the lateral ligament complex on the outside of your ankle.
The Anterior Talo-Fibular Ligament (ATFL): This is the weakest and most frequently torn ligament. It stops the foot from sliding forward.
The Calcaneofibular Ligament (CFL): The secondary stabilizer, torn in more severe grade 2 or grade 3 sprains.
The Posterior Talo-Fibular Ligament (PTFL): Rarely torn unless the ankle undergoes massive trauma.

The Neurological Damage: Loss of Proprioception
When you tear a ligament, you do not just tear collagen fibers; you tear specialized nerve endings called mechanoreceptors.
What is Proprioception?
Proprioception is your body's subconscious ability to know where its joints are in space. When you walk on uneven ground, mechanoreceptors in your ankle instantly tell your brain to fire the peroneal muscles on the side of your leg to prevent a roll.
The Delay in Signaling
When an ankle is sprained, these nerve endings are destroyed. Even after the ligament heals structurally, the neurological connection is delayed. Your brain cannot react fast enough to a sudden shift in terrain, virtually guaranteeing you will roll the ankle again. Physiotherapy is the only way to rebuild this neurological pathway.
Primary Source Proof: Proprioceptive Rehabilitation
The clinical literature explicitly states that progressive neuromuscular training is non-negotiable for preventing recurrent ankle injuries.
Download Clinical Efficacy PDF: The Effectiveness of Proprioceptive Training in the Prevention of Chronic Ankle Instability (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for ankle rehabilitation.
The Rehab Mechanics Treatment Protocol
Restoring a sprained ankle to 100% capacity requires a phased, progressive loading strategy. Passive treatments like ice and compression are only useful for the first 48 hours. After that, active rehab begins.
Phase 1: Acute Management and Mobility (Weeks 1-2)
The goal is to control the swelling while preventing the joint capsule from freezing solid.
Edema Control: Utilizing lymphatic drainage massage and specific taping techniques to flush swelling out of the joint.
Early Range of Motion (ROM): Prescribing pain-free, active movements (like drawing the alphabet with your toes) to align the new collagen fibers correctly as they heal.
Joint Mobilization: Physiotherapists gently glide the talocrural joint to ensure it does not become stiff and restricted.
Phase 2: Muscular Fortification (Weeks 3-6)
Once the acute pain subsides, we must replace the lost stability of the torn ligament with muscular strength.
Peroneal Strengthening: Using resistance bands to heavily strengthen the peroneal muscles on the outside of the calf. These muscles are the body's active defense against rolling the ankle inward.
Calf and Tibialis Anterior Loading: Rebuilding the primary shock absorbers of the lower leg to handle the impact of walking and stairs.
Manual Therapy: Deep tissue release on the calf to prevent compensatory tightness from altering your gait.
Phase 3: Neuromuscular Re-education (Weeks 6+)
This is the phase that prevents the next sprain. We rebuild the brain-to-ankle connection.
Balance Training: Progressing from single-leg standing on solid ground, to standing with eyes closed, to standing on unstable surfaces like a BOSU ball or wobble board.
Dynamic Perturbations: The physiotherapist applies unexpected forces while the patient balances, forcing the nervous system to react instantaneously to stabilize the joint.
Plyometrics and Return to Sport: Incorporating jumping, cutting, and lateral bounding drills to prepare the ankle for the chaotic forces of sports and active living.
Secure Your Foundation in Queen West
An unstable ankle changes the way you walk, which eventually damages your knees, hips, and lower back. Treat the injury correctly the first time.
Book a comprehensive ankle assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced biomechanical care in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Should I Stop Running if I Have Severe Shin Splints?
No. Total rest weakens tissues. Physiotherapy cures shin splints by analyzing your running biomechanics, strengthening your lower leg musculature, and utilizing targeted modalities to heal medial tibial stress syndrome while keeping you safely active.
The Frustration of Medial Tibial Stress Syndrome
For the active residents of Parkdale and Trinity Bellwoods, running is more than just exercise; it is a fundamental part of the Toronto lifestyle. However, one of the most common and devastating injuries that sidelines local runners is "shin splints," medically known as Medial Tibial Stress Syndrome (MTSS).
The typical cycle is incredibly frustrating. You feel a dull, aching pain along the inner edge of your shin bone during your run. You ignore it. It worsens into a sharp, burning sensation that persists even while walking. You finally stop running, ice your shins for a month, and wait for the pain to vanish. But the very first day you return to the pavement, the pain instantly returns.
At Rehab Mechanics, we see this exact cycle weekly. The problem with complete rest is that it does absolutely nothing to address why the shin bone became inflamed in the first place. Resolving MTSS requires a biomechanical approach to foot function and load management.
Structural Analysis: What Causes Shin Splints?
To permanently eliminate shin pain, we must perform a structural analysis of the lower leg's kinetic chain. Shin splints are an overuse injury, but they are driven by specific biomechanical failures.
The Anatomy of MTSS
The pain you feel is the result of excessive pulling forces on the periosteum (the thin layer of tissue covering the bone) of the tibia (shinbone).
The Tibialis Posterior: This muscle runs down the back of your calf, crosses under the inside of your ankle, and attaches to the bottom of your foot. Its primary job is to hold up your foot arch.
The Soleus Muscle: A deep calf muscle responsible for absorbing the massive shock of landing with every stride.
Biomechanical Triggers for MTSS
When these muscles are overwhelmed, they pull violently at their attachment points on the shin bone, causing micro-tearing and extreme inflammation.
Excessive Overpronation
If your foot arch collapses too much when you land (overpronation), the tibialis posterior is violently stretched.
The Whiplash Effect: This rapid stretching creates a "whiplash" effect on the muscle tendon, transferring the shear stress directly into the tibial bone.
Weak Hip Stabilizers
If your gluteus medius (side hip muscle) is weak, your knee will collapse inward (knee valgus) when your foot strikes the ground.
The Kinetic Chain Breakdown
This inward knee collapse forces the tibia to rotate internally, massively increasing the torsional strain on the shin bone and lower leg fascia.
Primary Source Proof: Running Kinematics
Our approach to treating running pathologies rejects passive rest in favor of active, evidence-based rehabilitation protocols.
Download Clinical Efficacy PDF: The Role of Biomechanical Loading and Foot Orthoses in the Management of Medial Tibial Stress Syndrome (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for running-related rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating MTSS effectively requires a progressive, phased approach. We do not just treat the shin; we rebuild the entire leg.
Phase 1: Acute Load Management and Inflammation Control
We do not prescribe total rest, but we do prescribe relative rest.
Activity Modification: We will temporarily replace pavement running with pain-free cross-training (like cycling or deep-water running) to maintain your cardiovascular fitness while the periosteum heals.
Manual Soft Tissue Release: Using targeted massage and instrument-assisted techniques to release the hypertonic (overly tight) soleus and tibialis posterior muscles, reducing their pull on the bone.
Shockwave Therapy: For chronic, stubborn cases, we may utilize shockwave therapy to stimulate blood flow and cellular repair directly at the tibial attachment site.
Phase 2: Structural Strengthening
This is where the cure happens. We must increase the load capacity of your lower leg.
Intrinsic Foot Strengthening: Exercises like "foot doming" or towel scrunches to rebuild the tiny muscles inside the foot that support the arch.
Heavy Slow Resistance (HSR) Calf Training: Progressing from double-leg to single-leg weighted calf raises, specifically focusing on the bent-knee soleus raise, to build bulletproof lower leg tissue.
Gluteal Activation: Clamshells, lateral band walks, and single-leg deadlifts to stabilize the pelvis and prevent the knee from caving inward during the running stride.
Phase 3: Gait Retraining and Return to Run (RTR)
Before you return to Trinity Bellwoods, we must fix the way you run.
Cadence Modification: Increasing your step rate by just 5% to 10% drastically reduces the impact forces on the shin bone with each step.
Orthotics Assessment: If structural flat feet are the root cause, Sanjay is qualified to dispense custom medical orthotics to permanently correct the foot mechanics.
Graded RTR Program: Providing a strict, interval-based running schedule to progressively re-introduce mechanical load to the tibia without triggering a relapse.
Run Without Pain in Parkdale and Queen West
Do not let chronic shin splints ruin your running season. Get a definitive biomechanical assessment and an active rehabilitation plan.
Book an appointment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible from Parkdale, Queen West, and Liberty Village.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Does Physiotherapy Actually Help Severe Lumbar Spinal Stenosis?
Yes. Physiotherapy provides profound relief for lumbar spinal stenosis. By restoring specific spinal flexion mechanics, decompressing the narrowed nerve canals, and fortifying the deep core stabilizers, physiotherapy eliminates neurogenic leg heaviness and dramatically improves walking capacity without invasive spinal surgery.
The Frustration of the "Shopping Cart" Lean
Toronto is a highly walkable city. From strolling through Trinity Bellwoods to navigating the grocery aisles in Liberty Village, the ability to walk comfortably is central to urban independence.
However, for many older adults and individuals with advanced spinal wear-and-tear, walking more than five minutes triggers a devastating symptom profile: a deep, cramping heaviness in both legs, numbness in the calves, and severe, aching lower back pain.
Strangely, the moment these patients sit down on a park bench or lean heavily forward on a shopping cart, the pain vanishes almost instantly. This highly specific presentation is the classic hallmark of Lumbar Spinal Stenosis, a condition characterized by neurogenic claudication.
Patients are frequently told that their spine is "crumbling" and that major spinal fusion or laminectomy surgery is inevitable. At Rehab Mechanics, our advanced spinal pathology programs prove otherwise. We utilize precise, biomechanical decompression techniques and targeted neuromuscular control to physically widen the space for your nerves, keeping you upright, walking, and out of the operating room.
Structural Analysis: The Mechanics of Spinal Crowding
To effectively treat spinal stenosis, we must perform a deep anatomical analysis of the lumbar spine and exactly why the nerves are suffocating.
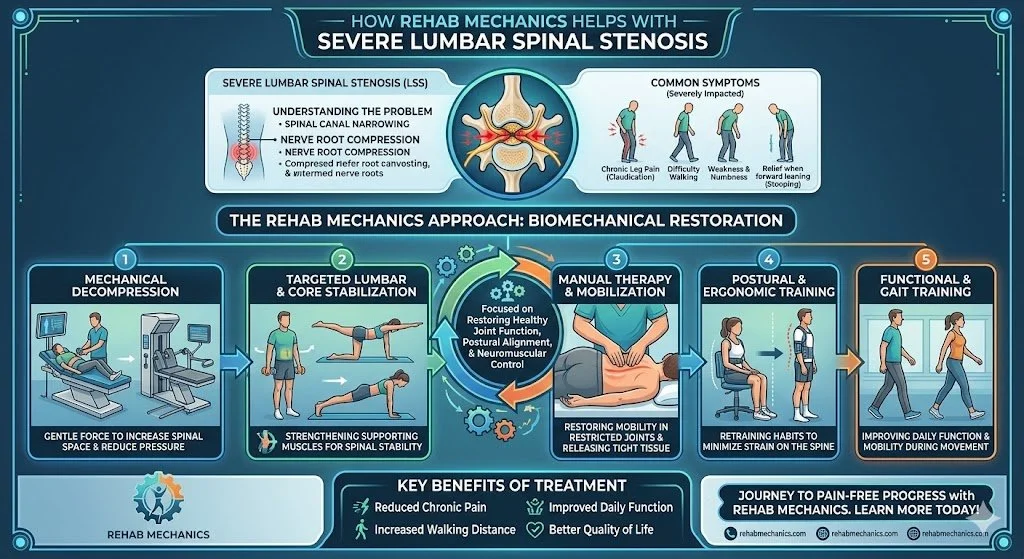
Anatomy of the Spinal Canal
Your spinal cord and nerve roots travel down your back through a central hollow tube (the spinal canal) and exit out the sides of the spine through tiny bony holes called the neural foramina.
The Stenotic Cascade
Spinal stenosis literally means "narrowing of the spine." It is a degenerative cascade that shrinks these essential spaces.
Disc Degeneration: As we age, the shock-absorbing discs between our vertebrae lose water height and flatten out.
Facet Joint Hypertrophy: Because the discs are flat, the tiny joints at the back of the spine (facet joints) absorb excessive friction. They develop severe osteoarthritis and grow massive, jagged bone spurs (osteophytes) that protrude directly into the nerve canals.
Ligamentum Flavum Thickening: A thick ligament runs down the inside of the spinal canal to provide stability. In stenosis, this ligament buckles and massively thickens, violently choking the spinal cord from behind.
Neurogenic Claudication (Why Walking Hurts)
The hallmark symptom of stenosis is neurogenic claudication—the cramping and severe leg heaviness that only happens when you walk or stand up straight.
The Postural Trigger (Extension vs. Flexion)
Extension (Standing Up): When you stand perfectly straight or walk, your lumbar spine naturally arches backward (lumbar extension). This physical movement completely closes down the already-crowded spinal canal and neural foramina, instantly pinching the nerves and cutting off their blood supply.
Flexion (Leaning Forward): When you sit down or lean forward on a shopping cart, your spine rounds forward (lumbar flexion). This mechanically opens the spinal canal by up to 20%, instantly relieving the nerve strangulation and allowing the leg pain to vanish.
Primary Source Proof: Non-Operative Decompression
Orthopedic and neurosurgical guidelines strongly advocate for specific, flexion-biased physical therapy and manual decompression as the absolute first-line treatment for lumbar spinal stenosis prior to considering high-risk spinal decompression surgery.
Download Clinical Efficacy PDF: The Efficacy of Manual Therapy and Flexion-Biased Exercise in the Management of Lumbar Spinal Stenosis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for complex spinal rehabilitation.
The Rehab Mechanics Stenosis Protocol
Treating spinal stenosis is the exact opposite of treating a herniated disc. Generic back extension exercises (like yoga "cobra" poses) will violently aggravate a stenotic spine. We use a highly specialized, flexion-biased biomechanical approach.
Phase 1: Flexion-Biased Decompression
Our immediate goal is to safely create space for the crushed nerves.
Manual Joint Mobilization: Our physiotherapists apply highly specific, targeted pressure (Grade III/IV mobilizations) to the stiff lumbar vertebrae, gently stretching the tight joint capsules to maximize the available space in the neural foramina.
Flexion Stretching: Implementing precise, repeated knee-to-chest and child's pose movements to physically stretch the thickened ligamentum flavum and open the back of the spinal canal, immediately draining the neurological leg pain.
Traction: Utilizing manual, localized traction to decompress the spine and relieve the ischemic (blood-starved) nerve roots.
Phase 2: Pelvic Tilt Neuromuscular Control
Because leaning forward relieves the pain, we must teach your body how to mimic that position subtly while you are standing upright.
Posterior Pelvic Tilts: We rigorously train the deep lower abdominal muscles to rotate your pelvis backward (tucking your tailbone). This flattens the lower back curve slightly, physically keeping the spinal canal open even when you are standing tall.
Hip Flexor Release: Sitting for years causes the hip flexors (psoas) to become rigidly tight. Tight hip flexors aggressively pull the spine forward into an arch (extension). We manually release these muscles to stop them from crushing the spinal canal.
Phase 3: Functional Walking Endurance
We must restore your cardiovascular capacity and walking distance safely.
Stationary Cycling: Because sitting opens the spine, stationary cycling is an incredible way to build leg strength and cardiovascular fitness without triggering neurogenic claudication.
Incline Treadmill Walking: Walking on an uphill incline naturally forces the body to lean slightly forward, opening the spine and allowing patients to rebuild their walking endurance without pain.
Keep Walking Without Pain
Do not let spinal stenosis confine you to a chair or force you into a risky, irreversible spinal fusion. By mastering your pelvic mechanics and manually decompressing the spine, expert physiotherapy can dramatically improve your walking tolerance and eliminate the heavy, cramping pain in your legs.
Book a comprehensive spinal assessment with our specialized clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic and neurological care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Should I See a Pelvic Physiotherapist for C-Section Scar Pain?
Yes. You should see a specialized physiotherapist after a C-Section. Advanced scar mobilization and myofascial release prevent rigid pelvic adhesions, restore deep core activation, and eliminate chronic lower back and pelvic pain long after the surgical incision has healed.
The Overlooked Reality of Major Abdominal Surgery
Toronto is a fast-paced city, and the pressure on new mothers to "bounce back" quickly after childbirth is immense. While cesarean sections account for a massive percentage of births, society frequently minimizes the procedure, treating it as a routine delivery rather than what it truly is: major abdominal surgery.
Months, or even years, after a C-section, many mothers living in Queen West and beyond struggle with a profound sense of physical disconnection. They may experience a deep, burning pulling sensation in their lower pelvis when standing up straight, chronic lower back pain, painful intercourse, or a visible "shelf" of tissue hanging over their scar.
The standard medical follow-up at six weeks post-partum usually consists of a physician checking the surface incision to ensure it isn't infected. Once the skin is closed, mothers are often cleared for all exercise. But skin healing is not tissue rehabilitation. At Rehab Mechanics, our highly specialized Perinatal & Pelvic Health program structurally treats the deep fascial trauma of a C-section, breaking down restrictive adhesions and rebuilding your core from the inside out.
Structural Analysis: The Biomechanics of Surgical Scarring
To understand why a C-section scar can cause massive biomechanical dysfunction throughout your entire body, we must perform a detailed analysis of surgical trauma and the body's fascial network.
The Seven Layers of Incision
A C-section does not just cut the skin. To reach the baby, the surgeon must physically incise or bluntly pull apart seven distinct anatomical layers:
Skin
Subcutaneous fat
Superficial fascia
Rectus sheath (the thick connective tissue holding your abdominal muscles)
Rectus abdominis muscle (separated manually)
Parietal peritoneum
The Uterus
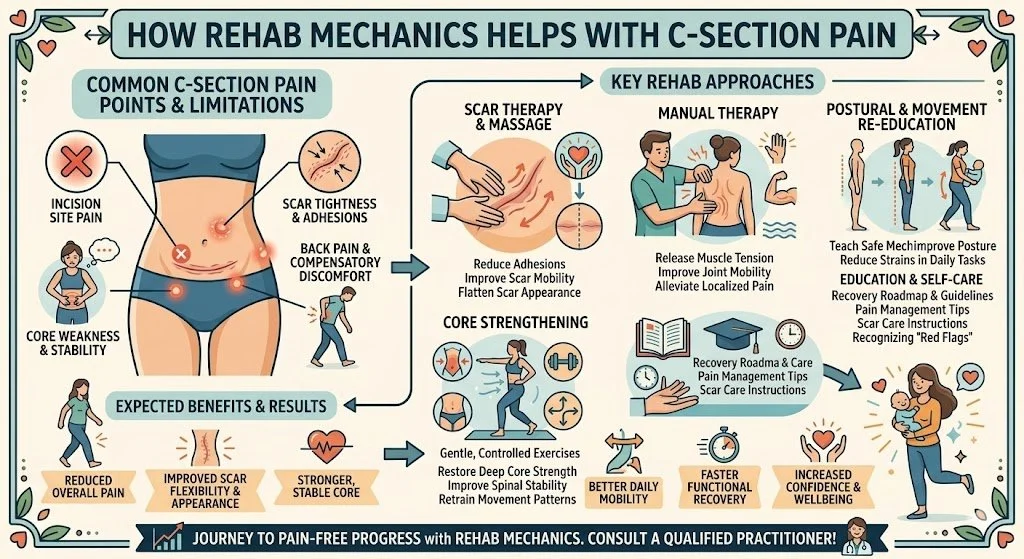
The Healing Process: Fibrotic Adhesions
When the body heals these seven layers, it does not heal them individually. It floods the area with inflammatory cells and lays down thick, dense, chaotic collagen fibers (scar tissue) that act like biological glue.
The "Fascial Pull" Effect
This biological glue frequently binds the different layers together—meaning your skin, muscles, and organs can literally become fused into one rigid block of scar tissue. This is known as an adhesion.
The Mechanical Restriction: Fascia is a continuous web of connective tissue that wraps your entire body. When a massive adhesion forms in your lower abdomen, it physically pulls the fascia tight from all directions.
The Downstream Pain: This tight abdominal "knot" forces you to walk slightly hunched forward. This chronic forward pull shuts down your glutes, over-stretches your lower back muscles, and alters the angle of your pelvis, leading to severe, chronic sacroiliac (SIJ) and lumbar spine pain.
The "Shelf" Effect
When the deep fascial layers are bound down tightly to the pubic bone, the healthy tissue and fat above the scar bulge outward over the restriction, creating the classic "C-section shelf." This is a structural mobility issue, not a weight issue.
Primary Source Proof: Post-Partum Rehabilitation
Clinical guidelines in perinatal health heavily mandate specialized, physiotherapist-guided myofascial release and deep core rehabilitation as the primary intervention for resolving post-cesarean pain and functional limitation.
Download Clinical Efficacy PDF: The Efficacy of Soft Tissue Mobilization and Core Rehabilitation Following Cesarean Section (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for post-partum and pelvic health rehabilitation.
The Rehab Mechanics Post-Op Protocol
Healing a C-section requires a trauma-informed, deeply specialized approach. We cannot just perform generic core exercises; we must physically un-bind the trapped tissue.
Phase 1: Deep Scar Mobilization and Desensitization
We must break the rigid adhesions holding your tissue hostage.
Myofascial Release: Once the incision is fully healed (typically past 6-8 weeks), our specialized physiotherapists perform deep, multi-directional manual mobilization directly on and around the scar. We gently pull and stretch the tissue to separate the skin from the underlying fascia and muscle.
Neurological Desensitization: Often, the cutaneous nerves surrounding the scar become hyper-sensitive, causing clothes to feel painful against the skin. We use specific tactile desensitization techniques to calm the nervous system.
Phase 2: Transversus Abdominis (TvA) Reactivation
The surgery brutally traumatized the communication between your brain and your deep core.
Neuromuscular Re-education: We utilize real-time tactile feedback and specialized breathing techniques to re-teach your brain how to fire the Transversus Abdominis (your deep biological corset). This must happen before you attempt any planks, crunches, or heavy lifting.
Restoring Intra-Abdominal Pressure: Re-training your diaphragm to coordinate perfectly with your pelvic floor, ensuring that when you cough or lift your baby, the pressure is distributed safely, rather than pushing outward against your vulnerable scar.
Phase 3: Pelvic Floor Integration and Functional Strength
A C-section does not spare the pelvic floor. The weight of a 9-month pregnancy still stretches and strains the pelvic sling.
Pelvic Health Assessment: Evaluating the resting tone of the pelvic floor to ensure the muscles are not locked in chronic protective spasm.
Dynamic Loading: Transitioning into mom-specific functional strength training. We teach you how to properly hinge at the hips, squat, and lift a heavy stroller without placing shear force on your lower back or anterior abdominal wall.
Reclaim Your Core and Comfort
You do not have to live with a painful, tight scar, a disconnected core, or chronic back pain as the permanent "price" of having a C-section. Specialized, gentle, and highly targeted physiotherapy can restore the sliding mobility of your abdominal fascia and rebuild your structural strength.
Book a comprehensive perinatal core and scar assessment with our specialized clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering accessible, elite care in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Cure De Quervain's Tenosynovitis Without Cortisone?
Yes. Physiotherapy effectively cures De Quervain’s tenosynovitis without cortisone. By utilizing targeted thumb splinting, deep soft tissue release, and progressive eccentric loading, physiotherapy reduces tendon sheath inflammation and restores pain-free grip strength for new parents and tech workers.
The Urban Epidemic of "Mommy Thumb" and Tech Wrist
Liberty Village and Queen West are vibrant neighborhoods characterized by two distinct demographics: young, growing families and highly driven tech professionals. While these groups seem completely different, they frequently walk into Rehab Mechanics suffering from the exact same debilitating injury: De Quervain's Tenosynovitis.
Whether you are repeatedly lifting a growing newborn out of a crib 30 times a day, or spending 10 hours furiously typing and swiping on a smartphone, your thumbs and wrists are undergoing massive, unnatural mechanical stress.
When a sharp, catching, or burning pain develops at the base of the thumb and radiates up the forearm, basic tasks like turning a doorknob, holding a coffee mug, or unbuckling a car seat become agonizing. The traditional medical approach often involves a quick corticosteroid injection. However, chemical injections do not fix the biomechanical overload. To permanently resolve this severe wrist pain, you must physically rehabilitate the tendons and the restrictive sheaths that surround them.
Structural Analysis: The Anatomy of the First Dorsal Compartment
To understand why this specific injury is so stubborn and painful, we must perform a detailed biomechanical analysis of the wrist's architecture.
The Extensor Retinaculum
Your wrist is wrapped in a thick, fibrous band of connective tissue called the extensor retinaculum. Its job is to act like a biological pulley system, keeping your tendons strapped tightly to the bones of your wrist so they do not bow outward when you move your hand.
The Tunnels (Compartments): This band is divided into six distinct tunnels or "compartments."
The Vulnerable First Compartment: De Quervain's syndrome occurs exclusively in the very first compartment, located directly over the styloid process of the radius (the bony bump at the base of your thumb).
The Tendons Involved
Two specific tendons must share this incredibly tight, rigid tunnel:
Abductor Pollicis Longus (APL): The muscle that pulls your thumb away from your hand.
Extensor Pollicis Brevis (EPB): The muscle that straightens the tip of your thumb.
The Biomechanical Friction
Every time you grip an object and angle your wrist downward (a motion called ulnar deviation—exactly the motion used to lift a baby under the armpits), these two tendons slide rapidly back and forth through the first compartment.
Tenosynovitis Explained
When the mechanical load exceeds the tissue's capacity, a destructive cycle begins.
Synovial Swelling: The protective, lubricating sheath (synovium) surrounding the tendons becomes intensely inflamed and swollen from the friction.
The Strangulation Effect: Because the bony tunnel and the retinaculum cannot expand, the swollen tendons become trapped. They physically catch and grind against the walls of the tunnel, causing exquisite, sharp pain and sometimes a visible, hard swelling at the base of the thumb.
Identifying the Clinical Red Flags
De Quervain's is frequently misdiagnosed as carpal tunnel syndrome or thumb arthritis. We look for specific mechanical signs:
Finkelstein's Test: If you tuck your thumb inside your fist and aggressively tilt your wrist downward toward your pinky, a breathtaking, sharp pain along the thumb side of the wrist is a positive indicator.
The "Catch" or "Snap": A physical sensation of the tendon popping or snapping as it struggles to drag itself through the swollen compartment.
Localized Swelling: A tender, highly sensitive, swollen bump directly on the radial bone.
Primary Source Proof: Non-Operative Wrist Rehabilitation
Clinical orthopedic research explicitly supports the use of progressive, conservative physiotherapy—including targeted splinting and eccentric loading—as a highly effective, first-line intervention for stenosing tenosynovitis.
Download Clinical Efficacy PDF: The Effectiveness of Conservative Management and Eccentric Exercise in De Quervain’s Tenosynovitis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for upper extremity rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating De Quervain's requires absolute clinical precision. You cannot aggressively stretch an already strangled tendon. We utilize a highly specific, three-phased biomechanical approach.
Phase 1: Acute Offloading and Inflammation Control (Weeks 1-3)
We must physically stop the friction to allow the synovial swelling to subside.
Thumb Spica Splinting: We provide a specialized, rigid splint that immobilizes the thumb and wrist. Wearing this temporarily prevents the APL and EPB tendons from sliding through the inflamed compartment, halting the mechanical irritation.
Advanced Modalities: Utilizing extracorporeal shockwave therapy (ESWT) or targeted interferential currents to rapidly decrease the acute chemical inflammation without relying on oral medications.
Phase 2: Soft Tissue Decompression
The muscles attached to the inflamed tendons are usually in massive spasm.
Instrument-Assisted Soft Tissue Mobilization (IASTM): Our physiotherapists use specialized tools to break down the tight, fibrotic tissue in the forearm muscle bellies, instantly reducing the pulling tension on the tendons passing through the wrist.
Joint Mobilization: Gently mobilizing the carpal bones (specifically the scaphoid and trapezium) to ensure optimal joint mechanics and remove any secondary bony compression.
Phase 3: Eccentric Loading and Neuromuscular Control
Once the pain decreases, we must structurally rebuild the tendon to handle your daily life.
Eccentric Strengthening: Tendons respond incredibly well to the "lowering" phase of an exercise. We prescribe specific, heavy, slow eccentric thumb extensions and radial deviations to force the body to lay down new, healthy, parallel collagen fibers, thickening and bulletproofing the tendon.
Ergonomic Coaching: For parents, we teach the "scoop" lifting technique to avoid dangerous ulnar deviation. For tech workers, we implement ergonomic mouse alternatives and split keyboards to keep the wrist entirely neutral during a 10-hour workday.
Stop the Wrist Pain Today
You do not have to struggle to hold your child or type your emails. De Quervain's tenosynovitis is a structural problem with a highly effective mechanical solution.
Book a comprehensive upper extremity assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite orthopedic care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
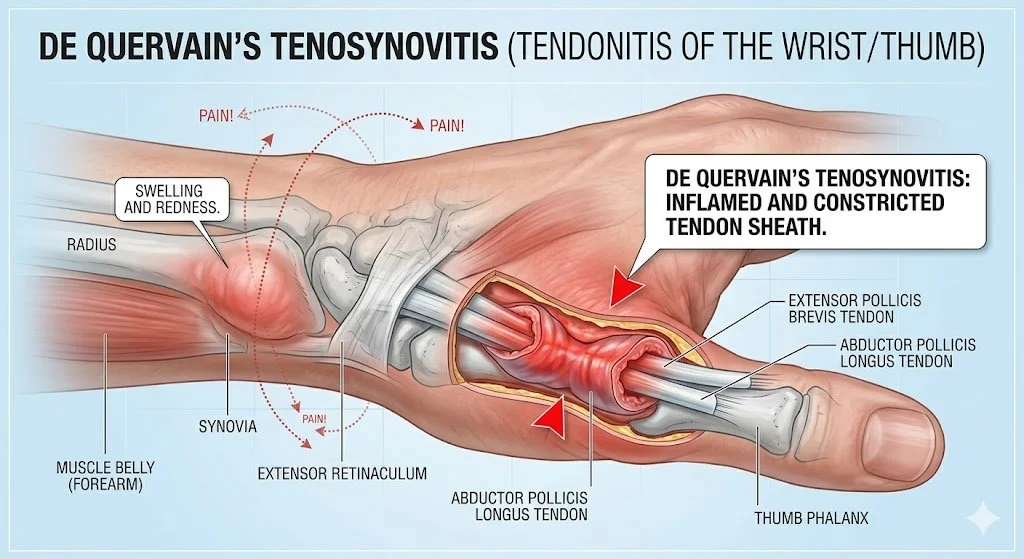
Can Physiotherapy Cure Thoracic Outlet Syndrome Without Surgery?
Yes. Physiotherapy successfully treats neurogenic Thoracic Outlet Syndrome without surgery. By correcting severe forward-head posture, mobilizing the first rib, and releasing hypertrophied scalene muscles, physical therapy mechanically decompresses the brachial plexus, eliminating radiating arm numbness, tingling, and chronic weakness.
The Misdiagnosed Numbness in Your Arm

For the thousands of Toronto professionals spending their days hunched over dual monitors in Liberty Village or carrying heavy commuter bags on the TTC, neck and arm pain is an all-too-common reality.
When patients experience a deep, aching pain in their neck accompanied by "pins and needles," numbness, or profound weakness shooting down their arm and into their hands, the initial medical assumption is usually one of two things: Carpal Tunnel Syndrome or a herniated cervical disc.
Patients often undergo weeks of wrist splinting or neck traction with absolutely zero relief. Why? Because the nerve compression is not happening in the wrist or the spine. It is happening in the crowded anatomical intersection between the neck and the shoulder—a condition known as Thoracic Outlet Syndrome (TOS).
At Rehab Mechanics, we specialize in complex musculoskeletal diagnostics. We understand that TOS is fundamentally a space issue caused by structural postural collapse. Through advanced manual therapy and precise biomechanical correction, we physically widen the thoracic outlet, saving patients from invasive nerve-decompression surgeries.
Structural Analysis: The Anatomy of the Thoracic Outlet
To understand how physiotherapy cures TOS, we must map the complex pathway of the nerves and blood vessels as they leave your neck and travel down into your arm.
The Brachial Plexus and Subclavian Vessels
The brachial plexus is a massive, highly sensitive bundle of nerves that exits the cervical spine. Along with the subclavian artery and vein, this bundle must travel through a very narrow, triangular passageway (the thoracic outlet) to reach your arm.
The Three Sites of Mechanical Strangulation
In Thoracic Outlet Syndrome, these vital nerves and blood vessels are physically crushed at one of three distinct anatomical bottlenecks.
1. The Scalene Triangle
The scalene muscles run from the side of your neck down to your first rib. The brachial plexus must thread the needle directly between the anterior and middle scalene muscles.
The Postural Trigger: If you have severe "tech neck" (forward head posture), these scalene muscles must overwork to hold your heavy head up.
The Strangulation: They become hypertrophied (thickened) and locked in spasm, acting like a tight vice grip that crushes the nerves against the first rib.
2. The Costoclavicular Space
This is the tiny gap between your collarbone (clavicle) and your first rib.
The Postural Trigger: Carrying heavy backpacks or simply slouching causes the collarbone to drop downward.
The Strangulation: The collarbone physically pins the brachial plexus and blood vessels directly against the rigid bone of the first rib, causing intense, throbbing arm pain and a feeling of "heaviness" or coldness in the hand.
3. The Pectoralis Minor Space
After passing the collarbone, the nerves must run directly underneath the pectoralis minor muscle on the front of your chest.
The Postural Trigger: Sitting with rounded, forward shoulders physically shortens the pec minor into a tight, dense band.
The Strangulation: When you reach your arm overhead, this tight muscular band acts like a tourniquet, cutting off the nerve signals and blood flow to the arm (known as the "Double Crush" effect).
Identifying the Clinical Red Flags
TOS presents with highly specific symptoms that differentiate it from a simple pinched neck nerve.
The Overhead Dead Arm: Lifting your arms overhead to wash your hair, hang curtains, or sleep with your arm under your pillow causes the arm to quickly "go to sleep," ache profoundly, or turn pale.
The Heavy Hand: A persistent feeling of clumsiness or dropping small objects like keys or a coffee mug.
The Ulnar Distribution: The tingling is usually most severe in the pinky and ring fingers, tracing up the inside of the forearm.
Aching Collarbone: A dull, deep ache located right at the base of the neck and behind the collarbone.
Primary Source Proof: Non-Operative Decompression
Clinical neurology and orthopedic literature confirm that targeted, conservative physiotherapy focusing on muscular release and postural restoration is the highly effective, first-line standard of care for neurogenic Thoracic Outlet Syndrome.
Download Clinical Efficacy PDF: Conservative Management and Physiotherapy for Neurogenic Thoracic Outlet Syndrome (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for nerve entrapment rehabilitation.
The Rehab Mechanics TOS Protocol
Treating TOS requires absolute precision. We cannot use generic neck stretches, as aggressively pulling on an already-crushed nerve will only increase the burning pain. We must physically decompress the bottlenecks.
Phase 1: Advanced Decompression and Manual Therapy (Weeks 1-4)
Before we can correct posture, we must manually open the thoracic outlet.
First Rib Mobilization: Our Registered Physiotherapists use precise, downward manual pressure to mobilize an elevated, stuck first rib. Dropping this rib instantly creates massive physical space for the nerves to breathe.
Scalene and Pec Minor Release: Utilizing intensive soft tissue mobilization and ischemic compression to melt away the dense spasms in the neck and chest muscles that are strangulating the brachial plexus.
Diaphragmatic Breathing Integration: The scalene muscles are secondary breathing muscles. We teach you how to breathe using your diaphragm to stop the scalenes from overworking and spasming with every breath you take.
Phase 2: Neurodynamic Flossing (Weeks 3-6)
Nerves need to slide smoothly to stay healthy.
Nerve Gliding: When compressed for months, the brachial plexus gets stuck in microscopic scar tissue. We prescribe specific, gentle "flossing" movements that tug the nerve back and forth through the thoracic outlet, breaking the adhesions and restoring its slippery mobility.
Phase 3: Scapular and Cervical Fortification (Weeks 6+)
This is the permanent cure. We must rebuild the muscular scaffolding that holds your collarbone and shoulders in a neutral, open position.
Lower Trapezius and Serratus Activation: Implementing heavy, targeted rows and prone Y-raises to strengthen the mid-back. These muscles physically pull the shoulder blades down and back, lifting the collarbone completely off the underlying nerves.
Deep Cervical Flexor Endurance: Re-training the tiny muscles in the front of your neck to hold your head perfectly balanced over your spine, ending the reliance on the overworked scalenes.
Stop the Numbness and Save Your Nerves
You do not have to live with a chronically numb, aching arm or consider risky surgical rib resections. By correcting the structural collapse of your upper body and widening the anatomical bottlenecks, physiotherapy can permanently free your nerves.
Book a comprehensive neurological and biomechanical assessment with our specialized team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Pelvic Floor Physiotherapy Cure Urinary Leakage When Running?
Yes. Pelvic floor physiotherapy effectively cures stress urinary incontinence. By utilizing targeted neuromuscular re-education, diaphragmatic breathing integration, and progressive internal strengthening, physiotherapy restores the structural integrity of the pelvic floor, eliminating leakage without the need for invasive surgical mesh procedures.
The Silent Struggle of the Active Urban Woman
Toronto is a city that moves. From high-intensity interval training (HIIT) classes in Liberty Village to weekend running groups tackling the Martin Goodman Trail, women in this city prioritize their health and fitness. However, there is a pervasive, silent barrier that forces many women to abandon the activities they love: Stress Urinary Incontinence (SUI).
Whether you are a post-partum mother trying to return to CrossFit or a woman who has simply noticed a sudden, embarrassing leak when sneezing, coughing, or performing jumping jacks, the psychological toll is immense. Women often silently alter their lives—wearing dark leggings, mapping out every bathroom on their running route, or quitting high-impact sports entirely.
The prevailing, outdated medical advice is often "just do your Kegels" or, worse, to simply accept leakage as a "normal" part of aging or motherhood. At Rehab Mechanics in Queen West, our specialized Perinatal & Pelvic Health program categorically rejects this notion. Leaking is common, but it is never normal. It is a biomechanical failure of the pelvic floor, and through advanced, specialized physiotherapy, it is highly curable.
Structural Analysis: The Biomechanics of the Pelvic Floor
To permanently cure incontinence, we must look far beyond generic "Kegel" exercises. We must perform a rigorous structural analysis of your deep core mechanics.
The Anatomy of the Pelvic Sling
Your pelvic floor is not a single muscle. It is a complex, hammock-like sling comprising 14 different muscles, fascia, and thick connective tissues that stretch from your pubic bone in the front to your tailbone (sacrum) in the back.
The Sphincteric Function: These muscles physically wrap around your urethra, vagina, and rectum. When they contract, they kink these tubes shut, preventing the involuntary loss of urine or feces.
The Supportive Function: They act as the literal floor of your abdominal cavity, holding up your bladder, uterus, and bowels against the constant, downward pull of gravity.
The Mechanics of Intra-Abdominal Pressure (IAP)
Your core operates like a pressurized soda can.
The Roof: Your respiratory diaphragm.
The Walls: Your deep abdominal muscles (transversus abdominis).
The Floor: Your pelvic floor muscles.
The "Pressure Leak" Concept
Every time you run, jump, cough, or lift a heavy barbell, the pressure inside this "soda can" skyrockets.
The Biomechanical Failure
If your pelvic floor muscles are weak, overly tight, or uncoordinated, they cannot withstand this sudden spike in pressure. The downward force overwhelms the urethral sphincter, and a leak occurs. This is the exact definition of Stress Urinary Incontinence.
Why Generic Kegels Fail
A "Kegel" is simply a concentric contraction of the pelvic floor. For many women, doing more Kegels actually makes the problem worse.
Hypertonic (Overactive) Pelvic Floors: Many high-achieving, stressed urban professionals unconsciously clench their pelvic floors all day long (similar to clenching the jaw).
The Rubber Band Analogy: A muscle that is constantly clenched is exhausted and short. If you try to stretch a rubber band that is already pulled tight, it snaps. If your pelvic floor is already spasming, it cannot contract any further when you jump, leading to immediate leakage.
The Clinical Reality: In these cases, the treatment is not strengthening; the treatment is lengthening and releasing the pelvic floor before any strengthening can safely occur.
Primary Source Proof: Efficacy of Pelvic Rehabilitation
Clinical guidelines universally mandate that specialized, physiotherapist-guided pelvic floor muscle training must be the absolute first line of treatment for urinary incontinence, outperforming pharmacological and surgical interventions in long-term safety and efficacy.
Download Clinical Efficacy PDF: The Efficacy of Pelvic Floor Muscle Training in the Conservative Management of Stress Urinary Incontinence (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for pelvic health rehabilitation.
The Rehab Mechanics Pelvic Floor Protocol
Our specialized pelvic health physiotherapists utilize a highly discreet, trauma-informed, and scientifically phased approach to restoring your core mechanics.
Phase 1: Advanced Diagnostics and Internal Assessment
We do not guess what your pelvic floor is doing; we accurately assess it.
The Internal Exam: With your strict consent, a specially trained physiotherapist performs an internal vaginal examination. This is the only way to accurately assess the resting tone, strength, endurance, and fascial restrictions of the pelvic sling.
Neurological Screening: Ensuring that the nerves supplying the bladder and pelvic floor are firing correctly.
Diaphragmatic Assessment: Evaluating how your breathing patterns impact your pelvic floor tension.
Phase 2: Down-Training and Myofascial Release (Weeks 1-4)
If your pelvic floor is hypertonic (too tight), we must release the brakes.
Internal Trigger Point Release: Applying gentle, targeted pressure to painful knots within the pelvic floor muscles to stop chronic spasms.
360-Degree Breathing Integration: Re-training your diaphragm to expand outward into your ribs, rather than bearing down heavily on your bladder.
Fascial Lengthening: Teaching you specific, deep squatting and mobility exercises designed to open the bony pelvis and stretch the deep connective tissues.
Phase 3: Neuromuscular Up-Training (Weeks 4-8)
Once the muscles are supple, we build their strength and timing.
The "Knack" Technique: Teaching your nervous system to automatically pre-contract the pelvic floor milliseconds before a cough, sneeze, or jump to proactively counter the pressure spike.
Eccentric Loading: The pelvic floor must be able to stretch safely while under load (eccentric control) to absorb the shock of running. We use specific dynamic movements to train this elastic recoil.
Core Co-Contraction: Integrating the transversus abdominis with the pelvic floor so they fire simultaneously as a unified, supportive wall.
Phase 4: High-Impact Functional Simulation (Weeks 8+)
We simulate your specific athletic demands inside the clinic.
Plyometric Integration: We progress from slow lifts to rapid movements—like jumping rope, box jumps, and heavy deadlifts—while monitoring your intra-abdominal pressure management.
Return-to-Run Programming: Designing a structured, graduated running protocol that safely increases your pavement mileage without triggering a relapse of leakage or pelvic heaviness.
Reclaim Your Active Life
You do not have to accept urinary leakage as your new normal. You deserve to run, jump, laugh, and lift without fear or embarrassment.
Book a highly confidential, comprehensive pelvic health assessment with our specialized clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite, private care in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Does Poor Posture Cause Sharp Pain in the Middle of the Back?
Yes. Prolonged desk posture locks the thoracic spine and rib joints, causing sharp, stabbing mid-back pain. Physiotherapy utilizes targeted joint manipulation and postural strengthening to unlock the thoracic vertebrae, restoring full spinal extension and allowing for deep, pain-free breathing.
The Silent Agony of the Desk Worker
When people discuss back pain, they almost exclusively talk about the lower back (lumbar spine) or the neck (cervical spine). However, for the massive population of office workers, software developers, and creatives in downtown Toronto, there is a third, highly agonizing zone: the thoracic spine.
If you experience a sharp, knife-like stabbing sensation directly between your shoulder blades—especially after sitting at your desk for four hours—you are experiencing thoracic joint dysfunction.
This pain is uniquely frightening because it often wraps around the ribcage to the front of the chest, sometimes mimicking the symptoms of a heart condition or making it physically painful to take a deep breath. Countless patients end up in the emergency room out of fear, only to be told their heart is fine and they simply have "muscle strain."
At Rehab Mechanics, we know that generic muscle relaxants will not fix this. This sharp, stabbing pain is a profound mechanical joint lock caused by the modern urban lifestyle. Correcting it requires precise biomechanical physiotherapy to restore the lost mobility of your mid-back and ribcage.
Structural Analysis: The Mechanics of the Thoracic Spine
To understand why sitting ruins your mid-back, we must perform a detailed anatomical analysis of the thoracic spine and its unique relationship with your ribcage.
The Cage of Stability
Your thoracic spine consists of 12 vertebrae (T1 through T12). Unlike your highly mobile neck and lower back, the thoracic spine is designed for rigidity and protection.
The Rib Articulations: Every single thoracic vertebra attaches to a pair of ribs. These ribs wrap around to the front of your chest to protect your heart and lungs, forming the ribcage.
Costovertebral Joints: The tiny joints where the ribs meet the spine at the back are called costovertebral and costotransverse joints. These joints must pivot slightly every single time you inhale to allow your lungs to expand.
The Postural Lock-Down
The human body adapts specifically to the positions it holds most often.
The Kyphotic Curve
If you spend eight hours a day slouching over a laptop in Liberty Village, your thoracic spine is forced into deep, sustained flexion (a rounded "C" shape, known as kyphosis).
The Muscular Exhaustion: The muscles between your shoulder blades (rhomboids and middle trapezius) are stretched taut over this rounded spine. They become exhausted, chemically inflamed, and form massive, burning trigger points.
The Joint Jam (Rib Dysfunction)
The sharp, stabbing pain occurs when the actual joints lock up.
Because the spine is permanently rounded forward, it loses the physical ability to extend (arch backward).
When the thoracic spine locks, the tiny rib joints attached to it also jam.
The next time you try to twist to grab something behind you, or take a deep, forceful breath, that jammed rib joint violently pinches the surrounding capsule and nerves, sending a breathtaking jolt of pain through your chest and back.
Identifying the Clinical Red Flags
Thoracic joint dysfunction presents with highly specific mechanical symptoms that differentiate it from a simple muscle ache:
The Deep Breath Catch: Taking a maximum inhalation causes a sharp, pinching pain right next to the spine, forcing you to take shallow breaths.
The "Ice Pick" Sensation: A highly localized, burning point of pain just to the left or right of the spinal column between the shoulder blades.
Rotational Block: An inability to twist your torso fully when checking your blind spot in the car without a severe pulling sensation in the ribs.
Primary Source Proof: Thoracic Mobilization
Orthopedic research confirms that high-grade manual mobilization of the thoracic spine and ribs yields immediate and profound relief for mid-back pain, vastly outperforming generic stretching routines.
Download Clinical Efficacy PDF: The Efficacy of Thoracic Spine Manipulation and Mobilization in the Treatment of Mechanical Mid-Back Pain (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for spinal rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating thoracic pain is highly satisfying clinically because targeted joint mobilization often provides immediate, profound relief. However, we must follow that up with structural strengthening to ensure the pain does not return the next day.
Phase 1: Joint Unlocking and Decompression
We must physically restore the mobility of the spine and ribs.
High-Velocity Low-Amplitude (HVLA) Thrusts: When clinically appropriate, physiotherapists use highly specific, safe manipulations to instantly un-jam the locked facet and costovertebral joints, resulting in an immediate restoration of deep breathing capacity.
Manual Glides: Utilizing Grade III and IV sustained pressure on the vertebrae to gently stretch the stiffened joint capsules and encourage normal spinal extension.
Myofascial Pectoral Release: Stripping the tight chest muscles on the front of the body that are physically holding the spine in a rounded, kyphotic position.
Phase 2: Active Mobility Restoration
Once the joints are unlocked, we must train the nervous system to use the new range of motion.
Thoracic Extension Drills: Using foam rollers or specialized peanut massage balls to isolate and actively bend individual spinal segments backward, reversing the desk posture.
Rotational Mobility: Exercises like "open books" or quadruped T-spine rotations to ensure the ribcage can pivot smoothly without catching.
Phase 3: Scapular and Spinal Fortification
To permanently banish the pain, we must build the muscular strength to hold the spine upright against gravity.
Lower Trapezius Activation: Teaching you how to fire the muscles at the bottom of the shoulder blades to pull them down and back.
Isometric Endurance: Implementing heavy farmer's carries and prone positional holds to build the biological endurance needed to sit with perfect posture for an entire 8-hour workday without fatigue.
Reclaim Your Spine
You do not have to endure the burning, stabbing pain of a locked mid-back. Do not settle for another temporary massage. By addressing the specific joint mechanics of your thoracic spine and ribcage, physiotherapy can provide permanent relief and effortless posture.
Book a comprehensive spinal assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Cure Dizziness Caused by Neck Tension?
Yes. Cervicogenic dizziness is directly caused by mechanical joint dysfunction and severe muscle spasms in the upper neck. Specialized physiotherapy corrects these spinal faults, restoring proper proprioceptive signaling to the brain to permanently eliminate vertigo and chronic neck tightness.
The Frightening Reality of Unexplained Dizziness
Dizziness is one of the most disorienting, terrifying, and debilitating symptoms a person can experience. For active Toronto professionals, a sudden onset of vertigo—the sensation that the room is spinning, floating, or tilting—can make navigating crowded subway stations, staring at computer screens, or simply walking down Queen Street West feel impossible.
Patients often rush to their family doctor or an ENT (Ear, Nose, and Throat) specialist, assuming they have an inner ear infection or a severe neurological issue. However, when all MRI scans, blood tests, and inner ear exams come back perfectly normal, patients are frequently left without answers, struggling with daily nausea and a heavy, foggy head.
In many of these "unexplained" cases, the true culprit is not in the ear or the brain at all; it is in the neck. This condition is known as Cervicogenic Dizziness.
At Rehab Mechanics, we specialize in the complex biomechanical relationship between the cervical spine and the central nervous system. By treating the deep structural dysfunctions in your neck—whether caused by poor "Tech Neck" posture or a recent Motor Vehicle Accident (MVA)—we can reset your body's balance system and eliminate the dizziness at its source.
Structural Analysis: How the Neck Controls Balance
To understand how a tight muscle can make the room spin, we must perform a deep analysis of human sensorimotor integration. Your brain relies on three distinct systems to keep you balanced:
The Vestibular System: The inner ear canals that detect gravity and head movement.
The Visual System: Your eyes, which provide a horizon line.
The Proprioceptive System: The network of specialized nerve endings in your muscles and joints that tell the brain where your body is in space.
The Cervical Proprioceptive Network
The upper cervical spine (the top three vertebrae of your neck: C1, C2, and C3) contains the highest density of proprioceptive nerve endings in the entire human body.
The Suboccipital Muscles: These tiny, incredibly dense muscles at the absolute base of your skull act as high-speed sensors. They constantly fire signals to the brainstem to coordinate your eye movements with your head movements (the cervico-ocular reflex).
The Mechanism of Sensory Conflict
Cervicogenic dizziness occurs when there is a massive "sensory conflict" in the brain.
The Mechanical Jam
If you have sustained a whiplash injury, or if you sit hunched over a laptop for 50 hours a week, the joints of your upper neck become rigidly locked, and the suboccipital muscles go into a state of chronic, severe spasm.
The Confused Brain
When these neck joints lock up, those highly sensitive nerve endings send warped, distorted signals to the brain.
Your inner ear says: "The head is turning left."
Your eyes say: "The head is turning left."
Your locked neck muscles send a corrupted signal saying: "The head is completely stationary."
The brain receives conflicting data. It cannot process the mismatch, resulting in an immediate sensation of profound dizziness, floating, unsteadiness, and nausea.
Identifying the Clinical Red Flags
How do you know if your dizziness is coming from your neck rather than your inner ear?
Movement Triggers: The dizziness is specifically triggered by looking up at the ceiling, looking down at your phone, or rapidly turning your head to check a blind spot while driving.
Co-occurring Neck Pain: The dizziness is almost always accompanied by a stiff neck, a dull ache at the base of the skull, or tension headaches wrapping around the temples.
The "Foggy" Feeling: Rather than the violent, room-spinning vertigo of inner ear crystals (BPPV), cervicogenic dizziness is often described as a chronic, hazy "drunkenness" or unsteadiness on your feet.
Primary Source Proof: Sensorimotor Rehabilitation
Clinical neurology and musculoskeletal guidelines confirm that targeted manual therapy of the cervical spine combined with sensorimotor retraining is the most effective intervention for cervicogenic dizziness.
Download Clinical Efficacy PDF: The Effectiveness of Manual Therapy and Cervicogenic Sensorimotor Retraining in the Management of Dizziness (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for vestibular and cervical rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating cervicogenic dizziness requires immense precision. You cannot aggressively "crack" an inflamed upper neck and expect the dizziness to stop. We utilize a highly specialized, phased neuro-mechanical approach.
Phase 1: Upper Cervical Decompression
We must restore accurate nerve signaling by un-jamming the upper neck joints.
Sustained Natural Apophyseal Glides (SNAGs): Our physiotherapists use gentle, highly specific mobilization techniques to restore the microscopic gliding motion of the C1 and C2 vertebrae without aggressive force.
Suboccipital Myofascial Release: Applying deep, sustained ischemic compression to the base of the skull to melt away the dense muscular spasms that are distorting the proprioceptive signals.
Phase 2: Sensorimotor Retraining
Once the joints are moving freely, we must recalibrate the brain's balance center.
Gaze Stabilization Exercises: We prescribe specific visual tracking drills where you must keep your eyes locked on a target while smoothly rotating your head, retraining the cervico-ocular reflex.
Joint Position Error (JPE) Training: Using laser pointers attached to a headband, we teach your brain how to accurately find "center" again after turning your head, sharpening your neck's proprioception.
Phase 3: Postural Fortification
We must build the endurance necessary to hold your heavy head perfectly upright during long workdays.
Deep Cervical Flexor Endurance: Re-activating the tiny muscles in the front of your neck to take the mechanical load off the exhausted suboccipital muscles at the back of the skull.
Thoracic Extension: Mobilizing and strengthening the mid-back (rhomboids and traps) to provide a solid, stable foundation for the cervical spine.
Regain Your Balance and Clarity
You do not have to live in a haze, relying on anti-nausea medications that make you drowsy. By treating the mechanical joint stiffness and muscular spasms in your neck, you can eliminate the sensory conflict causing your vertigo.
Book a comprehensive cervical and vestibular assessment with our specialized clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced neurological and orthopedic care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Is My Sciatica Actually Caused by Piriformis Syndrome?
Maybe. True sciatica originates from a compressed spinal disc, whereas piriformis syndrome occurs when a tight gluteal muscle crushes the sciatic nerve. Physiotherapy provides a definitive clinical diagnosis and utilizes deep tissue release to instantly decompress the nerve without invasive spinal procedures.
The Diagnostic Confusion of Nerve Pain
If you live and work in Toronto—whether you are sitting for ten hours a day at a tech startup in Liberty Village or commuting across the city—you are highly susceptible to lower body nerve pain.
When a sharp, burning, electrical shock of pain shoots deep into your buttock cheek and radiates down the back of your thigh, the immediate, terrifying assumption is that you have "blown a disc" in your spine. Patients immediately jump to conclusions about herniated lumbar discs, permanent nerve damage, and the looming threat of spinal surgery.
However, in a significant percentage of cases, the spine itself is perfectly healthy. The nerve is absolutely being crushed, but the compression is happening much lower down in the kinetic chain, buried deep inside the muscles of your hip. This is known clinically as Piriformis Syndrome.
At Rehab Mechanics in Queen West, we specialize in advanced differential diagnosis. We do not just guess where your nerve is pinched based on your symptoms; we use specific structural provocation testing to locate the exact millimeter of compression, saving you from unnecessary spinal MRIs and directing the treatment to the true mechanical source of your pain.
Structural Analysis: The Anatomy of the Gluteal Region
To understand why Piriformis Syndrome perfectly mimics a slipped disc, we must perform a deep anatomical analysis of the hip and the pathway of the sciatic nerve.
The Piriformis Muscle: The Hidden Rotator
Deep underneath your massive gluteus maximus (the main surface muscle of your buttocks) lies a network of six tiny "deep external rotator" muscles. The most prominent of these is the piriformis.
The Anatomical Anchor: The piriformis muscle attaches directly to the front of your sacrum (the tailbone) and reaches across to attach to the greater trochanter (the bony bump on the outside of your hip).
The Mechanical Function: Its primary job is to externally rotate your leg (turn your foot outward) and stabilize the hip joint when you are walking or running.
The Sciatic Nerve Pathway
The sciatic nerve is the longest and thickest nerve in the human body, roughly the width of your thumb.
The Intersection: After exiting the lumbar spine, the sciatic nerve must travel down the back of the leg. To do this, it must pass through the exact same tight pelvic space as the piriformis muscle.
The Anatomical Anomaly: In about 80% of the population, the nerve runs directly underneath the piriformis muscle belly. In the other 20%, the nerve physically pierces directly through the center of the muscle fibers.
The Compression Mechanism
Piriformis Syndrome is fundamentally a mechanical strangulation of this massive nerve.
The "Wallet Neuropathy" Effect
If you sit at a desk all day, or sit with a thick wallet in your back pocket, you are applying constant, ischemic (blood-restricting) pressure to the piriformis muscle.
The Spasm: The muscle becomes exhausted, hypertonic, and locks into a rigid spasm.
The Strangulation: Because the sciatic nerve sits millimeters below (or inside) this muscle, the spasming piriformis acts like a tightened vice grip, crushing the nerve against the pelvic bone.
Biomechanical Overload
The muscle can also spasm from weakness. If your primary glute muscles are weak, the tiny piriformis tries to take over the massive job of stabilizing your entire pelvis during running or climbing stairs. It rapidly fails, swells, and crushes the nerve.
Identifying the Clinical Red Flags: Spine vs. Muscle
How do we differentiate a spinal disc herniation from a tight glute muscle? We look for specific mechanical clues.
Sitting Intolerance: Piriformis syndrome is excruciating when sitting on hard surfaces (like a wooden dining chair) because you are sitting directly on the crushed nerve. Lumbar disc issues often hurt when bending forward.
The FAIR Test Response: Flexion, Adduction, and Internal Rotation (FAIR) of the hip tightly stretches the piriformis muscle. If this specific stretch reproduces your burning leg pain, the culprit is the muscle, not the spine.
The Absence of Spinal Pain: In Piriformis Syndrome, pressing directly on the lower back (lumbar spine) produces no pain. Pressing your thumb deep into the center of the buttock cheek, however, will cause the patient to jump off the table.
Primary Source Proof: Differentiating Sciatica
Clinical guidelines in orthopedics strictly mandate comprehensive differential diagnosis to prevent the misdiagnosis of deep gluteal pain as lumbar radiculopathy.
Download Clinical Efficacy PDF: Deep Gluteal Syndrome and the Efficacy of Conservative Physiotherapy in the Management of Piriformis Syndrome (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for nerve entrapment rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating Piriformis Syndrome requires a highly targeted, two-phased approach: immediately decompress the nerve, and then structurally rebuild the hip to prevent the muscle from spasming again.
Phase 1: Acute Neurological Decompression (Weeks 1-3)
We must force the piriformis muscle to release its grip on the sciatic nerve.
Deep Myofascial Release: Our physiotherapists use precise, deep-tissue ischemic compression directly on the piriformis trigger points to manually break the muscular spasm.
Sciatic Nerve Flossing (Neurodynamics): Nerves need to slide smoothly to stay healthy. We teach you specific "flossing" movements that gently pull the sciatic nerve back and forth through the tight muscle, freeing it from microscopic scar tissue adhesions.
Joint Mobilization: Freeing up the sacroiliac (SI) joint. If the pelvis is locked, the piriformis will stay tight trying to protect it.
Phase 2: Structural Gluteal Fortification (Weeks 4-8)
If we simply stretch the muscle, the pain will return the moment you sit back down at your desk. We must build the surrounding structural support.
Gluteus Maximus Activation: We implement heavy, targeted resistance training (like hip thrusts and heavy bridges) to force the large glute muscles to do their job, allowing the tiny piriformis to relax.
Eccentric Loading: Safely lengthening the external rotators under load to build robust, resilient tissue that will not spasm under the stress of daily urban walking.
Ergonomic Correction: Re-training your seated posture to ensure you are bearing weight on your "sit bones" (ischial tuberosities) rather than rolling backward onto the fleshy gluteal tissue and crushing the nerve.
Stop Guessing with Your Nerve Pain
You do not have to live with radiating leg pain, and you shouldn't assume you need spinal surgery without a thorough biomechanical workup. Expert physiotherapy can unlock your hip, free the sciatic nerve, and restore your quality of life.
Book a comprehensive differential diagnosis assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.

Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Cure Golfer's Elbow Without Stopping Weightlifting?
Yes. Physiotherapy effectively cures golfer's elbow by utilizing heavy slow resistance training, deep tissue release, and biomechanical correction of the wrist flexors. This active approach rebuilds degenerated tendon capacity, allowing you to lift weights safely without requiring complete rest or steroid injections.
The Grip Strength Dilemma in Urban Athletes
In Queen West and Liberty Village, the local fitness culture is intense. Between heavy barbell training, CrossFit, indoor rock climbing, and recreational golf, Toronto residents demand massive pulling power from their upper bodies.
However, this relentless demand on grip strength often results in a sharp, burning pain on the inside of the elbow—a condition medically known as Medial Epicondylitis, or "Golfer's Elbow." Despite the name, the vast majority of our patients with this condition have never swung a golf club; they are software developers, powerlifters, and construction workers.
When inner elbow pain strikes, the traditional advice is to stop lifting, ice the area, and wear a brace. But for an active urban professional, taking three months off from the gym is unacceptable and, clinically, it is the wrong approach. Complete rest causes tendons to atrophy and weaken. At Rehab Mechanics, we resolve Medial Epicondylitis not by resting the tendon, but by actively remodeling it to handle heavier loads.
Structural Analysis: The Mechanics of the Inner Elbow
To understand why passive rest fails to fix Golfer's Elbow, we must perform a detailed biomechanical analysis of the forearm flexors and the nature of tendinopathy.
The Flexor-Pronator Mass
Your forearm contains a complex network of muscles that control your wrist and fingers. The muscles responsible for bending your wrist forward (flexion) and turning your palm face down (pronation) all merge into a single, thick common tendon.
The Anatomical Anchor: This common flexor tendon anchors directly onto the medial epicondyle—the prominent bony bump on the inside of your elbow.
The Mechanical Overload: Every time you grip a heavy deadlift bar, perform a pull-up, or even type furiously on a non-ergonomic keyboard, massive tension is transferred through these muscles directly into that small bony attachment.
The Pathology of Tendinopathy
Golfer's elbow is rarely an acute, inflammatory "tendinitis." It is almost always a chronic, degenerative "tendinosis."
Failed Cellular Healing
When the flexor tendon is overloaded repetitively, it sustains microscopic tears.
The Chaotic Repair: Instead of laying down strong, perfectly parallel Type I collagen fibers to fix the tears, an exhausted body patches the area with weak, disorganized Type III scar tissue.
Angiofibroblastic Degeneration: The tendon physically thickens, loses its elasticity, and becomes infiltrated with highly sensitive, dysfunctional nerve endings and weak blood vessels.
The Valgus Stress Factor
In sports and lifting, poor shoulder or wrist mechanics often create "valgus stress"—a lateral outward pulling force on the elbow joint.
If your shoulder lacks external rotation during a heavy lift, your elbow is forced to flare out, violently yanking on the medial epicondyle and accelerating the tendon degeneration.
Primary Source Proof: Active Tendon Loading
Orthopedic research explicitly supports progressive, heavy mechanical loading over passive rest or corticosteroid injections for the long-term cure of chronic tendinopathies.
Download Clinical Efficacy PDF: The Efficacy of Heavy Slow Resistance Training in the Management of Medial Epicondylitis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for tendon rehabilitation.
The Rehab Mechanics Treatment Protocol
To cure Golfer’s Elbow, we must break down the chaotic scar tissue and stimulate the growth of new, aligned collagen fibers. We achieve this through a rigorous, phased clinical pathway.
Phase 1: Pain Modulation and Neovascularization
Before we can aggressively load the tendon, we must alter the chemical environment and reduce acute pain.
Shockwave Therapy: Utilizing high-energy acoustic sound waves to literally shatter the fibrotic scar tissue at the medial epicondyle. This mechanical stimulus forces the body to grow new, healthy blood vessels (neovascularization) into the deadened tendon.
Myofascial Release: Applying deep, instrument-assisted soft tissue mobilization (IASTM) to the belly of the forearm flexors to release trigger points, instantly reducing the pulling tension on the elbow bone.
Phase 2: Isometric Loading (The Analgesic Phase)
We must introduce load to the tendon without moving the joint, which acts as a powerful pain reliever.
Heavy Isometrics: Having the patient hold a heavy dumbbell in a flexed wrist position without moving for 45-second intervals. This safely engages the muscle-tendon unit, signaling the brain to down-regulate pain sensitivity.
Phase 3: Eccentric and Heavy Slow Resistance (HSR)
This is where the permanent structural remodeling occurs.
Eccentric Wrist Flexion: Focusing specifically on the "lowering" phase of a wrist curl. Eccentric contractions physically pull the chaotic collagen fibers into perfectly parallel alignment, rebuilding the tendon's tensile strength.
Pronation/Supination Loading: Using offset weights (like a hammer or specialized club) to strengthen the rotational muscles of the forearm, which are critical for stabilizing the elbow during heavy lifting.
Phase 4: Kinetic Chain Integration
Finally, we must fix the faulty movement patterns that caused the overload.
Shoulder and Scapular Strengthening: Improving rotator cuff strength and mid-back mobility so the elbow no longer has to compensate for a weak shoulder during heavy pulling movements.
Reclaim Your Grip Strength
Do not let chronic elbow pain force you to abandon your fitness goals. A degenerated tendon requires mechanical rehabilitation, not a heavy brace and a bottle of ibuprofen.
Book a comprehensive upper extremity assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, right in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.

Can Pelvic Floor Physiotherapy Cure Urinary Leakage When Running?
Yes. Pelvic floor physiotherapy effectively cures stress urinary incontinence. By utilizing targeted neuromuscular re-education, diaphragmatic breathing integration, and progressive internal strengthening, physiotherapy restores the structural integrity of the pelvic floor, eliminating leakage without the need for invasive surgical mesh procedures.
The Silent Struggle of the Active Urban Woman
Toronto is a city that moves. From high-intensity interval training (HIIT) classes in Liberty Village to weekend running groups tackling the Martin Goodman Trail, women in this city prioritize their health and fitness. However, there is a pervasive, silent barrier that forces many women to abandon the activities they love: Stress Urinary Incontinence (SUI).
Whether you are a post-partum mother trying to return to CrossFit or a woman who has simply noticed a sudden, embarrassing leak when sneezing, coughing, or performing jumping jacks, the psychological toll is immense. Women often silently alter their lives—wearing dark leggings, mapping out every bathroom on their running route, or quitting high-impact sports entirely.
The prevailing, outdated medical advice is often "just do your Kegels" or, worse, to simply accept leakage as a "normal" part of aging or motherhood. At Rehab Mechanics in Queen West, our specialized Perinatal & Pelvic Health program categorically rejects this notion. Leaking is common, but it is never normal. It is a biomechanical failure of the pelvic floor, and through advanced, specialized physiotherapy, it is highly curable.
Structural Analysis: The Biomechanics of the Pelvic Floor
To permanently cure incontinence, we must look far beyond generic "Kegel" exercises. We must perform a rigorous structural analysis of your deep core mechanics.
The Anatomy of the Pelvic Sling
Your pelvic floor is not a single muscle. It is a complex, hammock-like sling comprising 14 different muscles, fascia, and thick connective tissues that stretch from your pubic bone in the front to your tailbone (sacrum) in the back.
The Sphincteric Function: These muscles physically wrap around your urethra, vagina, and rectum. When they contract, they kink these tubes shut, preventing the involuntary loss of urine or feces.
The Supportive Function: They act as the literal floor of your abdominal cavity, holding up your bladder, uterus, and bowels against the constant, downward pull of gravity.
The Mechanics of Intra-Abdominal Pressure (IAP)
Your core operates like a pressurized soda can.
The Roof: Your respiratory diaphragm.
The Walls: Your deep abdominal muscles (transversus abdominis).
The Floor: Your pelvic floor muscles.
The "Pressure Leak" Concept
Every time you run, jump, cough, or lift a heavy barbell, the pressure inside this "soda can" skyrockets.
The Biomechanical Failure
If your pelvic floor muscles are weak, overly tight, or uncoordinated, they cannot withstand this sudden spike in pressure. The downward force overwhelms the urethral sphincter, and a leak occurs. This is the exact definition of Stress Urinary Incontinence.
Why Generic Kegels Fail
A "Kegel" is simply a concentric contraction of the pelvic floor. For many women, doing more Kegels actually makes the problem worse.
Hypertonic (Overactive) Pelvic Floors: Many high-achieving, stressed urban professionals unconsciously clench their pelvic floors all day long (similar to clenching the jaw).
The Rubber Band Analogy: A muscle that is constantly clenched is exhausted and short. If you try to stretch a rubber band that is already pulled tight, it snaps. If your pelvic floor is already spasming, it cannot contract any further when you jump, leading to immediate leakage.
The Clinical Reality: In these cases, the treatment is not strengthening; the treatment is lengthening and releasing the pelvic floor before any strengthening can safely occur.
Primary Source Proof: Efficacy of Pelvic Rehabilitation
Clinical guidelines universally mandate that specialized, physiotherapist-guided pelvic floor muscle training must be the absolute first line of treatment for urinary incontinence, outperforming pharmacological and surgical interventions in long-term safety and efficacy.
Download Clinical Efficacy PDF: The Efficacy of Pelvic Floor Muscle Training in the Conservative Management of Stress Urinary Incontinence (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for pelvic health rehabilitation.
The Rehab Mechanics Pelvic Floor Protocol
Our specialized pelvic health physiotherapists utilize a highly discreet, trauma-informed, and scientifically phased approach to restoring your core mechanics.
Phase 1: Advanced Diagnostics and Internal Assessment
We do not guess what your pelvic floor is doing; we accurately assess it.
The Internal Exam: With your strict consent, a specially trained physiotherapist performs an internal vaginal examination. This is the only way to accurately assess the resting tone, strength, endurance, and fascial restrictions of the pelvic sling.
Neurological Screening: Ensuring that the nerves supplying the bladder and pelvic floor are firing correctly.
Diaphragmatic Assessment: Evaluating how your breathing patterns impact your pelvic floor tension.
Phase 2: Down-Training and Myofascial Release (Weeks 1-4)
If your pelvic floor is hypertonic (too tight), we must release the brakes.
Internal Trigger Point Release: Applying gentle, targeted pressure to painful knots within the pelvic floor muscles to stop chronic spasms.
360-Degree Breathing Integration: Re-training your diaphragm to expand outward into your ribs, rather than bearing down heavily on your bladder.
Fascial Lengthening: Teaching you specific, deep squatting and mobility exercises designed to open the bony pelvis and stretch the deep connective tissues.
Phase 3: Neuromuscular Up-Training (Weeks 4-8)
Once the muscles are supple, we build their strength and timing.
The "Knack" Technique: Teaching your nervous system to automatically pre-contract the pelvic floor milliseconds before a cough, sneeze, or jump to proactively counter the pressure spike.
Eccentric Loading: The pelvic floor must be able to stretch safely while under load (eccentric control) to absorb the shock of running. We use specific dynamic movements to train this elastic recoil.
Core Co-Contraction: Integrating the transversus abdominis with the pelvic floor so they fire simultaneously as a unified, supportive wall.
Phase 4: High-Impact Functional Simulation (Weeks 8+)
We simulate your specific athletic demands inside the clinic.
Plyometric Integration: We progress from slow lifts to rapid movements—like jumping rope, box jumps, and heavy deadlifts—while monitoring your intra-abdominal pressure management.
Return-to-Run Programming: Designing a structured, graduated running protocol that safely increases your pavement mileage without triggering a relapse of leakage or pelvic heaviness.
Reclaim Your Active Life
You do not have to accept urinary leakage as your new normal. You deserve to run, jump, laugh, and lift without fear or embarrassment.
Book a highly confidential, comprehensive pelvic health assessment with our specialized clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite, private care in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.


Is My Sciatica Actually Caused by Piriformis Syndrome?
Maybe. True sciatica originates from a compressed spinal disc, whereas piriformis syndrome occurs when a tight gluteal muscle crushes the sciatic nerve. Physiotherapy provides a definitive clinical diagnosis and utilizes deep tissue release to instantly decompress the nerve without invasive spinal procedures.
The Diagnostic Confusion of Nerve Pain
If you live and work in Toronto—whether you are sitting for ten hours a day at a tech startup in Liberty Village or commuting across the city—you are highly susceptible to lower body nerve pain.
When a sharp, burning, electrical shock of pain shoots deep into your buttock cheek and radiates down the back of your thigh, the immediate, terrifying assumption is that you have "blown a disc" in your spine. Patients immediately jump to conclusions about herniated lumbar discs, permanent nerve damage, and the looming threat of spinal surgery.
However, in a significant percentage of cases, the spine itself is perfectly healthy. The nerve is absolutely being crushed, but the compression is happening much lower down in the kinetic chain, buried deep inside the muscles of your hip. This is known clinically as Piriformis Syndrome.
At Rehab Mechanics in Queen West, we specialize in advanced differential diagnosis. We do not just guess where your nerve is pinched based on your symptoms; we use specific structural provocation testing to locate the exact millimeter of compression, saving you from unnecessary spinal MRIs and directing the treatment to the true mechanical source of your pain.
Structural Analysis: The Anatomy of the Gluteal Region
To understand why Piriformis Syndrome perfectly mimics a slipped disc, we must perform a deep anatomical analysis of the hip and the pathway of the sciatic nerve.
The Piriformis Muscle: The Hidden Rotator
Deep underneath your massive gluteus maximus (the main surface muscle of your buttocks) lies a network of six tiny "deep external rotator" muscles. The most prominent of these is the piriformis.
The Anatomical Anchor: The piriformis muscle attaches directly to the front of your sacrum (the tailbone) and reaches across to attach to the greater trochanter (the bony bump on the outside of your hip).
The Mechanical Function: Its primary job is to externally rotate your leg (turn your foot outward) and stabilize the hip joint when you are walking or running.
The Sciatic Nerve Pathway
The sciatic nerve is the longest and thickest nerve in the human body, roughly the width of your thumb.
The Intersection: After exiting the lumbar spine, the sciatic nerve must travel down the back of the leg. To do this, it must pass through the exact same tight pelvic space as the piriformis muscle.
The Anatomical Anomaly: In about 80% of the population, the nerve runs directly underneath the piriformis muscle belly. In the other 20%, the nerve physically pierces directly through the center of the muscle fibers.
The Compression Mechanism
Piriformis Syndrome is fundamentally a mechanical strangulation of this massive nerve.
The "Wallet Neuropathy" Effect
If you sit at a desk all day, or sit with a thick wallet in your back pocket, you are applying constant, ischemic (blood-restricting) pressure to the piriformis muscle.
The Spasm: The muscle becomes exhausted, hypertonic, and locks into a rigid spasm.
The Strangulation: Because the sciatic nerve sits millimeters below (or inside) this muscle, the spasming piriformis acts like a tightened vice grip, crushing the nerve against the pelvic bone.
Biomechanical Overload
The muscle can also spasm from weakness. If your primary glute muscles are weak, the tiny piriformis tries to take over the massive job of stabilizing your entire pelvis during running or climbing stairs. It rapidly fails, swells, and crushes the nerve.
Identifying the Clinical Red Flags: Spine vs. Muscle
How do we differentiate a spinal disc herniation from a tight glute muscle? We look for specific mechanical clues.
Sitting Intolerance: Piriformis syndrome is excruciating when sitting on hard surfaces (like a wooden dining chair) because you are sitting directly on the crushed nerve. Lumbar disc issues often hurt when bending forward.
The FAIR Test Response: Flexion, Adduction, and Internal Rotation (FAIR) of the hip tightly stretches the piriformis muscle. If this specific stretch reproduces your burning leg pain, the culprit is the muscle, not the spine.
The Absence of Spinal Pain: In Piriformis Syndrome, pressing directly on the lower back (lumbar spine) produces no pain. Pressing your thumb deep into the center of the buttock cheek, however, will cause the patient to jump off the table.
Primary Source Proof: Differentiating Sciatica
Clinical guidelines in orthopedics strictly mandate comprehensive differential diagnosis to prevent the misdiagnosis of deep gluteal pain as lumbar radiculopathy.
Download Clinical Efficacy PDF: Deep Gluteal Syndrome and the Efficacy of Conservative Physiotherapy in the Management of Piriformis Syndrome (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for nerve entrapment rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating Piriformis Syndrome requires a highly targeted, two-phased approach: immediately decompress the nerve, and then structurally rebuild the hip to prevent the muscle from spasming again.
Phase 1: Acute Neurological Decompression (Weeks 1-3)
We must force the piriformis muscle to release its grip on the sciatic nerve.
Deep Myofascial Release: Our physiotherapists use precise, deep-tissue ischemic compression directly on the piriformis trigger points to manually break the muscular spasm.
Sciatic Nerve Flossing (Neurodynamics): Nerves need to slide smoothly to stay healthy. We teach you specific "flossing" movements that gently pull the sciatic nerve back and forth through the tight muscle, freeing it from microscopic scar tissue adhesions.
Joint Mobilization: Freeing up the sacroiliac (SI) joint. If the pelvis is locked, the piriformis will stay tight trying to protect it.
Phase 2: Structural Gluteal Fortification (Weeks 4-8)
If we simply stretch the muscle, the pain will return the moment you sit back down at your desk. We must build the surrounding structural support.
Gluteus Maximus Activation: We implement heavy, targeted resistance training (like hip thrusts and heavy bridges) to force the large glute muscles to do their job, allowing the tiny piriformis to relax.
Eccentric Loading: Safely lengthening the external rotators under load to build robust, resilient tissue that will not spasm under the stress of daily urban walking.
Ergonomic Correction: Re-training your seated posture to ensure you are bearing weight on your "sit bones" (ischial tuberosities) rather than rolling backward onto the fleshy gluteal tissue and crushing the nerve.
Stop Guessing with Your Nerve Pain
You do not have to live with radiating leg pain, and you shouldn't assume you need spinal surgery without a thorough biomechanical workup. Expert physiotherapy can unlock your hip, free the sciatic nerve, and restore your quality of life.
Book a comprehensive differential diagnosis assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced care in the heart of Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Cure Dizziness Caused by Neck Tension?
Yes. Cervicogenic dizziness is directly caused by mechanical joint dysfunction and severe muscle spasms in the upper neck. Specialized physiotherapy corrects these spinal faults, restoring proper proprioceptive signaling to the brain to permanently eliminate vertigo and chronic neck tightness.
The Frightening Reality of Unexplained Dizziness
Dizziness is one of the most disorienting, terrifying, and debilitating symptoms a person can experience. For active Toronto professionals, a sudden onset of vertigo—the sensation that the room is spinning, floating, or tilting—can make navigating crowded subway stations, staring at computer screens, or simply walking down Queen Street West feel impossible.
Patients often rush to their family doctor or an ENT (Ear, Nose, and Throat) specialist, assuming they have an inner ear infection or a severe neurological issue. However, when all MRI scans, blood tests, and inner ear exams come back perfectly normal, patients are frequently left without answers, struggling with daily nausea and a heavy, foggy head.
In many of these "unexplained" cases, the true culprit is not in the ear or the brain at all; it is in the neck. This condition is known as Cervicogenic Dizziness.
At Rehab Mechanics, we specialize in the complex biomechanical relationship between the cervical spine and the central nervous system. By treating the deep structural dysfunctions in your neck—whether caused by poor "Tech Neck" posture or a recent Motor Vehicle Accident (MVA)—we can reset your body's balance system and eliminate the dizziness at its source.
Structural Analysis: How the Neck Controls Balance
To understand how a tight muscle can make the room spin, we must perform a deep analysis of human sensorimotor integration. Your brain relies on three distinct systems to keep you balanced:
The Vestibular System: The inner ear canals that detect gravity and head movement.
The Visual System: Your eyes, which provide a horizon line.
The Proprioceptive System: The network of specialized nerve endings in your muscles and joints that tell the brain where your body is in space.
The Cervical Proprioceptive Network
The upper cervical spine (the top three vertebrae of your neck: C1, C2, and C3) contains the highest density of proprioceptive nerve endings in the entire human body.
The Suboccipital Muscles: These tiny, incredibly dense muscles at the absolute base of your skull act as high-speed sensors. They constantly fire signals to the brainstem to coordinate your eye movements with your head movements (the cervico-ocular reflex).
The Mechanism of Sensory Conflict
Cervicogenic dizziness occurs when there is a massive "sensory conflict" in the brain.
The Mechanical Jam
If you have sustained a whiplash injury, or if you sit hunched over a laptop for 50 hours a week, the joints of your upper neck become rigidly locked, and the suboccipital muscles go into a state of chronic, severe spasm.
The Confused Brain
When these neck joints lock up, those highly sensitive nerve endings send warped, distorted signals to the brain.
Your inner ear says: "The head is turning left."
Your eyes say: "The head is turning left."
Your locked neck muscles send a corrupted signal saying: "The head is completely stationary."
The brain receives conflicting data. It cannot process the mismatch, resulting in an immediate sensation of profound dizziness, floating, unsteadiness, and nausea.
Identifying the Clinical Red Flags
How do you know if your dizziness is coming from your neck rather than your inner ear?
Movement Triggers: The dizziness is specifically triggered by looking up at the ceiling, looking down at your phone, or rapidly turning your head to check a blind spot while driving.
Co-occurring Neck Pain: The dizziness is almost always accompanied by a stiff neck, a dull ache at the base of the skull, or tension headaches wrapping around the temples.
The "Foggy" Feeling: Rather than the violent, room-spinning vertigo of inner ear crystals (BPPV), cervicogenic dizziness is often described as a chronic, hazy "drunkenness" or unsteadiness on your feet.
Primary Source Proof: Sensorimotor Rehabilitation
Clinical neurology and musculoskeletal guidelines confirm that targeted manual therapy of the cervical spine combined with sensorimotor retraining is the most effective intervention for cervicogenic dizziness.
Download Clinical Efficacy PDF: The Effectiveness of Manual Therapy and Cervicogenic Sensorimotor Retraining in the Management of Dizziness (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for vestibular and cervical rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating cervicogenic dizziness requires immense precision. You cannot aggressively "crack" an inflamed upper neck and expect the dizziness to stop. We utilize a highly specialized, phased neuro-mechanical approach.
Phase 1: Upper Cervical Decompression
We must restore accurate nerve signaling by un-jamming the upper neck joints.
Sustained Natural Apophyseal Glides (SNAGs): Our physiotherapists use gentle, highly specific mobilization techniques to restore the microscopic gliding motion of the C1 and C2 vertebrae without aggressive force.
Suboccipital Myofascial Release: Applying deep, sustained ischemic compression to the base of the skull to melt away the dense muscular spasms that are distorting the proprioceptive signals.
Phase 2: Sensorimotor Retraining
Once the joints are moving freely, we must recalibrate the brain's balance center.
Gaze Stabilization Exercises: We prescribe specific visual tracking drills where you must keep your eyes locked on a target while smoothly rotating your head, retraining the cervico-ocular reflex.
Joint Position Error (JPE) Training: Using laser pointers attached to a headband, we teach your brain how to accurately find "center" again after turning your head, sharpening your neck's proprioception.
Phase 3: Postural Fortification
We must build the endurance necessary to hold your heavy head perfectly upright during long workdays.
Deep Cervical Flexor Endurance: Re-activating the tiny muscles in the front of your neck to take the mechanical load off the exhausted suboccipital muscles at the back of the skull.
Thoracic Extension: Mobilizing and strengthening the mid-back (rhomboids and traps) to provide a solid, stable foundation for the cervical spine.
Regain Your Balance and Clarity
You do not have to live in a haze, relying on anti-nausea medications that make you drowsy. By treating the mechanical joint stiffness and muscular spasms in your neck, you can eliminate the sensory conflict causing your vertigo.
Book a comprehensive cervical and vestibular assessment with our specialized clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced neurological and orthopedic care in Toronto Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.