Can Physiotherapy Relieve the Sharp Groin Pain of Hip Impingement?
Yes. Physiotherapy provides profound relief for hip impingement (FAI). By restoring joint capsule mobility, strengthening the deep hip rotators, and correcting pelvic tilt, physiotherapy mechanically decompresses the hip joint, eliminating the sharp, pinching groin pain associated with femoroacetabular impingement.
The Mystery of Chronic Groin Pain
Groin pain is one of the most frustrating and frequently misdiagnosed complaints in sports medicine. For many active individuals in Toronto—whether they are avid cyclists riding along the waterfront, hockey players in local recreational leagues, or simply office workers who sit for 8 hours a day—a deep, pinching sensation in the front crease of the hip can quickly derail their lifestyle.
Often, patients assume they have simply pulled a "groin muscle" (adductor strain) and attempt to aggressively stretch it out. However, if stretching the hip makes the pinching sensation worse, or if you feel a sharp block when trying to pull your knee to your chest, you are likely not dealing with a muscle issue at all. You are dealing with a bone-on-bone structural conflict known as Femoroacetabular Impingement (FAI).
At Rehab Mechanics in Queen West, we specialize in the complex biomechanics of the hip and pelvis. We understand that FAI is a mechanical "jamming" of the joint. Through highly targeted physical therapy, we can alter the angle of your pelvis and the strength of your hip stabilizers to physically create more space inside the joint, stopping the painful friction without the need for invasive arthroscopic surgery.

Structural Analysis: The Mechanics of a Hip Pinch
To understand how to fix FAI, we must perform a biomechanical analysis of the hip joint's architecture and the bony changes that trigger impingement.
The Ball and Socket Architecture
Your hip is a massive, deep ball-and-socket joint. The "ball" is the femoral head (the top of your thigh bone), and the "socket" is the acetabulum (a deep cup in your pelvis).
In a healthy hip, the ball glides smoothly within the socket, lubricated by synovial fluid and protected by a thick ring of cartilage called the labrum.
The Bony Overgrowth (FAI)
Impingement occurs when extra bone grows on either the ball, the socket, or both. This overgrowth destroys the perfect spherical fit of the joint.
CAM Lesion: Extra bone grows on the neck of the femur (the ball). As you bend your hip up, this non-spherical bump forcefully jams into the rim of the socket.
Pincer Lesion: Extra bone extends out over the rim of the acetabulum (the socket), creating an "overhang" that crushes the femoral neck during movement.
The Danger to the Labrum
When these bony abnormalities violently crash into each other during activities like deep squatting, running, or sitting in low chairs, they trap the delicate labrum between them.
The Tearing Process
Over time, this relentless mechanical crushing causes the labrum to fray and eventually tear, leading to a deep, catching, or clicking pain deep inside the groin. If left untreated, the friction rapidly wears away the articular cartilage, accelerating early-onset hip osteoarthritis.
The Biomechanical Trigger: Anterior Pelvic Tilt
While you cannot exercise away a bony bump, you can completely alter how that bump interacts with the socket.
Many people with FAI sit for hours a day, developing extremely tight hip flexors.
This tightness pulls the entire pelvis forward and downward (an anterior pelvic tilt).
When the pelvis tilts forward, the roof of the hip socket physically lowers, drastically closing the space and making the bony impingement exponentially worse.
Primary Source Proof: Conservative Management of FAI
Orthopedic and sports medicine research strongly supports non-operative, physiotherapist-led rehabilitation as the primary, highly effective first-line intervention for Femoroacetabular Impingement, often successfully avoiding surgical intervention.
Download Clinical Efficacy PDF: The Efficacy of Physiotherapist-Led Rehabilitation in the Management of Femoroacetabular Impingement Syndrome (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for hip rehabilitation.
The Rehab Mechanics Impingement Protocol
Our clinical goal is mechanical decompression. We must change the resting position of the pelvis and teach the femoral head to glide inferiorly (downward) to clear the impingement zone during movement.
Phase 1: Joint Decompression and Soft Tissue Release
We must physically create space in the cramped joint capsule.
Manual Joint Distraction: Our physiotherapists use heavy, hands-on traction bands to gently pull the femur out of the socket. This immediately relieves the pressure on the crushed labrum and stretches the incredibly dense, tight posterior hip capsule.
Hip Flexor and TFL Release: Aggressive manual soft tissue mobilization on the muscles at the front of the hip to release the "brakes" that are pulling the pelvis into that dangerous anterior tilt.
Phase 2: Pelvic Realignment and Deep Core Activation
We must teach your body how to hold the pelvis in a neutral position to permanently open the front of the hip socket.
Posterior Pelvic Tilt Training: Utilizing targeted lower abdominal training (transversus abdominis) to teach the nervous system how to rotate the pelvis backward, instantly lifting the roof of the socket away from the impingement.
Gluteus Maximus Fortification: The large glute muscles pull the pelvis backward. We use specific bridges and heavy hip thrusts to build the primary muscles responsible for fighting the tight hip flexors.
Phase 3: Dynamic Hip Control and Glute Medius Strengthening
The hip must remain centralized dynamically, meaning when you are walking or playing sports.
Deep Rotator Activation: Strengthening the tiny muscles deep under the glutes (like the piriformis and obturators) that act as the rotator cuff of the hip, keeping the ball perfectly centered in the socket.
Functional Movement Modification: We analyze your squat and running form. For instance, teaching a weightlifter to adopt a slightly wider stance with toes pointed outward can instantly clear the bony block, allowing them to squat heavy without pain.
Stop the Friction and Save Your Labrum
Do not let chronic groin pain progress into a severe labral tear or early arthritis. By correcting your pelvic mechanics and building robust hip stability, you can eliminate the pinching and return to the sports you love.
Book a comprehensive biomechanical hip assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite orthopedic care in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.



Can Physiotherapy Relieve the Sharp Groin Pain of Hip Impingement?
Yes. Physiotherapy provides profound relief for hip impingement (FAI). By restoring joint capsule mobility, strengthening the deep hip rotators, and correcting pelvic tilt, physiotherapy mechanically decompresses the hip joint, eliminating the sharp, pinching groin pain associated with femoroacetabular impingement.
The Mystery of Chronic Groin Pain
Groin pain is one of the most frustrating and frequently misdiagnosed complaints in sports medicine. For many active individuals in Toronto—whether they are avid cyclists riding along the waterfront, hockey players in local recreational leagues, or simply office workers who sit for 8 hours a day—a deep, pinching sensation in the front crease of the hip can quickly derail their lifestyle.
Often, patients assume they have simply pulled a "groin muscle" (adductor strain) and attempt to aggressively stretch it out. However, if stretching the hip makes the pinching sensation worse, or if you feel a sharp block when trying to pull your knee to your chest, you are likely not dealing with a muscle issue at all. You are dealing with a bone-on-bone structural conflict known as Femoroacetabular Impingement (FAI).
At Rehab Mechanics in Queen West, we specialize in the complex biomechanics of the hip and pelvis. We understand that FAI is a mechanical "jamming" of the joint. Through highly targeted physical therapy, we can alter the angle of your pelvis and the strength of your hip stabilizers to physically create more space inside the joint, stopping the painful friction without the need for invasive arthroscopic surgery.
Structural Analysis: The Mechanics of a Hip Pinch
To understand how to fix FAI, we must perform a biomechanical analysis of the hip joint's architecture and the bony changes that trigger impingement.
The Ball and Socket Architecture
Your hip is a massive, deep ball-and-socket joint. The "ball" is the femoral head (the top of your thigh bone), and the "socket" is the acetabulum (a deep cup in your pelvis).
In a healthy hip, the ball glides smoothly within the socket, lubricated by synovial fluid and protected by a thick ring of cartilage called the labrum.
The Bony Overgrowth (FAI)
Impingement occurs when extra bone grows on either the ball, the socket, or both. This overgrowth destroys the perfect spherical fit of the joint.
CAM Lesion: Extra bone grows on the neck of the femur (the ball). As you bend your hip up, this non-spherical bump forcefully jams into the rim of the socket.
Pincer Lesion: Extra bone extends out over the rim of the acetabulum (the socket), creating an "overhang" that crushes the femoral neck during movement.
The Danger to the Labrum
When these bony abnormalities violently crash into each other during activities like deep squatting, running, or sitting in low chairs, they trap the delicate labrum between them.
The Tearing Process
Over time, this relentless mechanical crushing causes the labrum to fray and eventually tear, leading to a deep, catching, or clicking pain deep inside the groin. If left untreated, the friction rapidly wears away the articular cartilage, accelerating early-onset hip osteoarthritis.
The Biomechanical Trigger: Anterior Pelvic Tilt
While you cannot exercise away a bony bump, you can completely alter how that bump interacts with the socket.
Many people with FAI sit for hours a day, developing extremely tight hip flexors.
This tightness pulls the entire pelvis forward and downward (an anterior pelvic tilt).
When the pelvis tilts forward, the roof of the hip socket physically lowers, drastically closing the space and making the bony impingement exponentially worse.
Primary Source Proof: Conservative Management of FAI
Orthopedic and sports medicine research strongly supports non-operative, physiotherapist-led rehabilitation as the primary, highly effective first-line intervention for Femoroacetabular Impingement, often successfully avoiding surgical intervention.
Download Clinical Efficacy PDF: The Efficacy of Physiotherapist-Led Rehabilitation in the Management of Femoroacetabular Impingement Syndrome (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for hip rehabilitation.
The Rehab Mechanics Impingement Protocol
Our clinical goal is mechanical decompression. We must change the resting position of the pelvis and teach the femoral head to glide inferiorly (downward) to clear the impingement zone during movement.
Phase 1: Joint Decompression and Soft Tissue Release
We must physically create space in the cramped joint capsule.
Manual Joint Distraction: Our physiotherapists use heavy, hands-on traction bands to gently pull the femur out of the socket. This immediately relieves the pressure on the crushed labrum and stretches the incredibly dense, tight posterior hip capsule.
Hip Flexor and TFL Release: Aggressive manual soft tissue mobilization on the muscles at the front of the hip to release the "brakes" that are pulling the pelvis into that dangerous anterior tilt.
Phase 2: Pelvic Realignment and Deep Core Activation
We must teach your body how to hold the pelvis in a neutral position to permanently open the front of the hip socket.
Posterior Pelvic Tilt Training: Utilizing targeted lower abdominal training (transversus abdominis) to teach the nervous system how to rotate the pelvis backward, instantly lifting the roof of the socket away from the impingement.
Gluteus Maximus Fortification: The large glute muscles pull the pelvis backward. We use specific bridges and heavy hip thrusts to build the primary muscles responsible for fighting the tight hip flexors.
Phase 3: Dynamic Hip Control and Glute Medius Strengthening
The hip must remain centralized dynamically, meaning when you are walking or playing sports.
Deep Rotator Activation: Strengthening the tiny muscles deep under the glutes (like the piriformis and obturators) that act as the rotator cuff of the hip, keeping the ball perfectly centered in the socket.
Functional Movement Modification: We analyze your squat and running form. For instance, teaching a weightlifter to adopt a slightly wider stance with toes pointed outward can instantly clear the bony block, allowing them to squat heavy without pain.

Stop the Friction and Save Your Labrum
Do not let chronic groin pain progress into a severe labral tear or early arthritis. By correcting your pelvic mechanics and building robust hip stability, you can eliminate the pinching and return to the sports you love.
Book a comprehensive biomechanical hip assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite orthopedic care in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is Physiotherapy Strictly Required After Rotator Cuff Surgery?
Yes. Post-operative physiotherapy is strictly mandatory following rotator cuff repair. Immediate, phased rehabilitation prevents severe capsular stiffness (frozen shoulder), protects the delicate surgical anchors, and progressively rebuilds neuromuscular control, ensuring you regain full overhead mobility and pain-free shoulder strength.
The Delicate Reality of Shoulder Surgery
Undergoing arthroscopic rotator cuff repair is a major orthopedic event. For patients in Toronto who have finally opted for surgery after years of chronic shoulder pain or a massive acute tear, the operation feels like the finish line. In reality, it is merely the starting line.
The surgeon's job is to physically reattach the torn tendon to the humerus (arm bone) using medical-grade anchors and sutures. However, this mechanical attachment is initially incredibly weak. It takes months for the tendon to biologically heal and fuse back into the bone.
If a patient attempts to rush their recovery by lifting their arm too soon, they risk ripping the anchors right out of the bone, requiring a devastating secondary surgery. Conversely, if a patient is terrified to move and keeps their arm rigidly locked in a sling for six weeks, the shoulder capsule will permanently shrink and scar down—a severe complication known as secondary adhesive capsulitis (frozen shoulder).
At Rehab Mechanics, we specialize in navigating this incredibly delicate post-surgical tightrope. We manage the exact, day-by-day loads placed on the healing tissue, ensuring a safe, complete return to functional mobility.
Structural Analysis: The Biology of Post-Surgical Healing
To understand why our strict physiotherapy protocols are non-negotiable, we must analyze the biological phases of tendon-to-bone healing.
The Inflammatory and Proliferative Phases
Immediately following surgery, the body floods the joint with inflammatory cells to clean up the surgical debris.
The Weakest Link: During the first 4 to 6 weeks, the only thing holding your rotator cuff to your arm bone is the surgical thread. The tendon itself is soft, inflamed, and highly vulnerable.
Active vs. Passive Movement: This is why you are strictly forbidden from actively lifting your arm using your own muscles. Contracting the repaired muscle will pull the sutures apart. However, the joint must still be moved passively by a physiotherapist to prevent the capsule from gluing itself shut.
The Remodeling Phase
From week 6 to 6 months, the body slowly replaces the weak inflammatory tissue with highly organized Type I collagen.
Mechanotransduction: This new collagen must be stressed in order to align properly and gain tensile strength. If the shoulder is not progressively loaded through physical therapy, the tendon heals as a weak, disorganized lump of scar tissue that will likely tear again in the future.
The Threat of Scapular Dyskinesis
While your arm is immobilized in a sling, your brain rapidly alters how it controls your shoulder blade (scapula).
The Compensation Trap
Your brain will "forget" how to use the rotator cuff and will try to lift your entire arm by violently shrugging your upper trapezius (neck muscles). If this faulty wiring (scapular dyskinesis) is not corrected through neuromuscular physiotherapy, you will develop severe, chronic neck pain and re-impinge the newly repaired tendon.
Primary Source Proof: Post-Operative Orthopedic Protocols
Advanced orthopedic literature universally mandates that criterion-based, strictly supervised physical therapy is the primary determining factor in the functional success of a rotator cuff repair.
Download Clinical Efficacy PDF: Evidence-Based Rehabilitation Guidelines Following Arthroscopic Rotator Cuff Repair (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for post-surgical orthopedic rehabilitation.

The Rehab Mechanics Post-Op Shoulder Protocol
Our clinical pathway is highly structured and entirely dependent on the specific size of your tear (small, medium, massive) and your surgeon's exact operative notes.
Phase 1: Maximum Protection (Weeks 0-6)
The goal is to protect the surgical repair while maintaining joint mobility.
Passive Range of Motion (PROM): The physiotherapist physically supports the weight of your arm and moves it through specific, safe arcs of motion. You do zero work.
Cervical and Scapular Release: Utilizing deep soft tissue massage on the neck and upper back to relieve the massive muscle spasms caused by wearing a heavy sling 24/7.
Pendulum Exercises: Teaching you how to use gravity and momentum to safely move the joint fluid at home without activating the repaired muscles.
Phase 2: Active-Assisted and Active ROM (Weeks 6-10)
As the tendon begins to fuse to the bone, we slowly wake the muscles up.
Pulley and Wand Exercises: Using a stick or an overhead pulley to allow your healthy arm to assist the surgical arm in lifting overhead safely.
Isometric Loading: Forcing the rotator cuff muscles to contract gently against an immovable resistance, which safely builds baseline strength and blood flow without moving the joint through a dangerous arc.
Scapular Setting: Re-training the mid-back to anchor the shoulder blade securely against the ribcage.
Phase 3: Progressive Strengthening (Weeks 10-16)
The tendon is now secure enough to handle direct load.
Isotonic Resistance Training: Utilizing light resistance bands and dumbbells to progressively load the Supraspinatus and Infraspinatus muscles.
Eccentric Focus: Emphasizing the slow, lowering phase of movement to align the new collagen fibers and maximize tendon thickness.
Phase 4: Advanced Functional Return (Months 4-6+)
We prepare the shoulder for the unpredictable demands of daily life and sports.
Plyometric Stability: Using rebounders or medicine balls to teach the rotator cuff to fire instantly and absorb rapid, unexpected forces.
Overhead Mechanics: Re-training the kinetic chain for complex movements like throwing, serving a tennis ball, or heavy barbell pressing.
Protect Your Surgical Investment
You endured the pain of a major surgery to get your life back; do not risk the outcome by neglecting your rehabilitation. Protect the repair and rebuild your strength the right way.
Book your specialized post-surgical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering elite orthopedic recovery right in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Should I See a Physiotherapist for a WSIB Workplace Injury Claim?
Yes. Consulting a physiotherapist immediately for a WSIB claim ensures rapid structural recovery and seamless administrative handling. Physiotherapy addresses repetitive strain and occupational trauma through targeted mechanical correction, while simultaneously managing Ontario’s complex workplace safety documentation and return-to-work screening.
The Reality of Occupational Injuries in Toronto
Getting injured on the job is a highly stressful event. Whether you suffered an acute lumbar sprain lifting heavy materials on a downtown construction site, or developed severe carpal tunnel syndrome from endless hours of typing at a Liberty Village tech firm, the impact on your livelihood is immediate.
When a workplace injury occurs in Ontario, it falls under the jurisdiction of the Workplace Safety and Insurance Board (WSIB). Navigating the WSIB system can be just as overwhelming as the physical pain itself. Delays in filing paperwork, misdiagnosed structural injuries, or poorly managed return-to-work plans can result in denied claims and chronic, long-term disability.
At Rehab Mechanics, we manage a broad operational spectrum of WSIB claims. We understand that occupational rehabilitation requires a dual approach: aggressive, evidence-based physical therapy to heal the injury, and meticulous administrative management to protect your compensation and employment status.
Structural Analysis: The Biomechanics of Workplace Trauma
Occupational injuries generally fall into two distinct mechanical categories. To successfully rehabilitate a worker, we must accurately analyze the mechanism of tissue failure.
1. Acute Macrotrauma
These are sudden, identifiable events that result in immediate, severe tissue damage.
The Mechanics: A slip on a wet warehouse floor, falling from a ladder, or forcefully catching a heavy, shifting load.
The Pathology: These events typically result in acute Grade 2 or 3 ligament sprains, severe muscle belly tears, spinal disc herniations, or acute meniscal tears. The immediate clinical priority is controlling extreme joint effusion (swelling) and preventing the formation of rigid, restrictive scar tissue.
2. Cumulative Trauma Disorders (CTDs)
Also known as Repetitive Strain Injuries (RSIs), these are insidious and often far more difficult to treat than an acute tear.
The Mechanics: Performing the same micro-movement thousands of times a day (e.g., scanning items, typing, operating vibrating machinery, or continuously looking down at an assembly line).
The Pathology: The human body is highly adaptable, but it requires varied movement. Constant, repetitive load without adequate recovery time exhausts the cellular capacity of tendons and fascia.
The Result: This leads to conditions like lateral epicondylitis (tennis elbow), rotator cuff tendinosis, and chronic myofascial pain syndrome. The tissue actually begins to degenerate at a cellular level, requiring aggressive mechanical loading to reverse the decay.
The Dangers of Ergonomic Failure
CTDs are almost entirely driven by poor ergonomics. If your workstation forces your spine out of a neutral alignment, your muscles must maintain a constant isometric contraction to hold you up, leading to inevitable fatigue and failure.
Primary Source Proof: Occupational Rehabilitation
Clinical guidelines from occupational health authorities mandate early active physical therapy over passive rest to ensure the highest rate of successful return-to-work outcomes.
Download Clinical Efficacy PDF: The Effectiveness of Early Physiotherapy Intervention in Reducing WSIB Claim Duration and Disability (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for occupational rehabilitation.
The Rehab Mechanics WSIB Protocol
We do not just treat the pain; we prepare your body to handle the specific mechanical demands of your occupation safely.
Phase 1: WSIB Programs of Care (POC) Integration
WSIB utilizes specific "Programs of Care" for common injuries (like the Low Back POC or the Upper Extremity POC).
Rapid Assessment: We complete your Initial Assessment Report (Form 8 or equivalent) precisely and promptly, establishing the clinical justification for your treatment plan.
Direct Billing: We coordinate directly with your WSIB adjudicator, ensuring treatments are pre-approved and billed directly so you face no out-of-pocket expenses.
Phase 2: Active Structural Rehabilitation
We utilize advanced modalities and manual therapy to accelerate tissue healing.
Targeted Modalities: Utilizing Shockwave Therapy or advanced interferential currents to rapidly decrease acute inflammation and break down chronic scar tissue from repetitive strain.
Manual Joint Mobilization: Unlocking stiff spinal segments or peripheral joints to restore the full range of motion required for your job duties.
Phase 3: Work Hardening and Functional Simulation
This is the most critical phase for preventing re-injury. We replicate your job in the clinic.
Task-Specific Loading: If you are a delivery driver, we train heavy, awkward lifting mechanics. If you are a desk worker, we build the postural endurance of your deep cervical flexors and mid-back to withstand 8-hour seated shifts.
Ergonomic Coaching: We provide actionable advice on how to modify your workstation or movement patterns to protect your joints moving forward.
Phase 4: Return-to-Work Screening
We collaborate with you and your employer to create a safe transition plan.
Modified Duties: We provide clear, medically justified restrictions (e.g., "no lifting over 15 lbs," "mandatory 5-minute break every hour") to ensure you are not thrown back into full duties before your tissues are biologically ready.

Protect Your Body and Your Livelihood
If you have suffered a workplace injury, immediate clinical intervention is your best defense against chronic pain and administrative nightmare.
Secure expert physical and administrative care today. Book a comprehensive WSIB assessment with our team. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced occupational rehabilitation in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is Surgery Mandatory to Fix Diastasis Recti After Pregnancy?
No. Surgery is rarely necessary for diastasis recti. Specialized post-partum physiotherapy can close the abdominal separation by utilizing specific deep core neuromuscular re-education, pelvic floor integration, and fascial tensioning protocols, safely restoring abdominal wall integrity and preventing chronic lower back pain.
Understanding the Post-Partum Body in Toronto
Navigating motherhood in a bustling city like Toronto is a beautiful but physically demanding journey. Carrying a heavy car seat up the steps of a Toronto walk-up, pushing a double stroller through Trinity Bellwoods, and constantly lifting a growing toddler requires a massive amount of core strength.
However, many new mothers find that months, or even years, after giving birth, their core feels profoundly disconnected. They may experience chronic lower back pain, pelvic instability, or a visible "doming" or "coning" down the center of their stomach when they sit up.
This condition is called Diastasis Recti Abdominis (DRA)—a stretching and separation of the abdominal wall. The immediate fear for many women is that this separation is permanent and requires a surgical "tummy tuck" (abdominoplasty) to repair. At Rehab Mechanics, our specialized perinatal and pelvic health programs prove otherwise. We use advanced, non-surgical biomechanical protocols to rebuild the integrity of your abdominal fascia from the inside out.
Structural Analysis: The Biomechanics of Diastasis Recti
To understand how to heal the core, we must analyze the structural mechanics of the abdominal wall and how it adapts during pregnancy.
The Anatomy of the Linea Alba
Your "six-pack" muscles (the rectus abdominis) are two parallel vertical muscle bands. They are joined perfectly down the center of your stomach by a thick, highly elastic band of connective tissue (fascia) called the linea alba.
The Pregnancy Shift: As your baby grows, the mechanical outward pressure against your abdominal wall becomes immense. Simultaneously, pregnancy hormones (like relaxin) soften your connective tissues.
The Stretching Effect: To make room for the baby, the linea alba physically stretches sideways. The two rectus muscles are pulled apart, widening the gap down the midline of your stomach.
The Danger of the "Coning" Effect
Diastasis Recti is not just a cosmetic issue; it is a profound mechanical failure of the body's natural weight belt.
Loss of Intra-Abdominal Pressure
Your deep core is a pressurized canister. The diaphragm is the roof, the pelvic floor is the base, and the transverse abdominis is the wrapping wall.
The Leak in the Canister: When the linea alba is stretched thin and weak, the front of the canister "leaks" pressure.
The Mechanical Consequence: Without this internal pressure, the lower back (lumbar spine) is forced to absorb 100% of the shock of daily movement, leading to severe, chronic lower back pain and sacroiliac joint (SIJ) dysfunction.
The Myth of Traditional Crunches
Traditional core exercises—like crunches, sit-ups, or heavy planks—create massive outward pressure. If the linea alba is already weak, doing a crunch forces the internal organs to push outward, creating a visible "dome" or "cone" down the middle of the stomach. This aggressively stretches the tissue further, making the diastasis worse.
Primary Source Proof: Conservative Perinatal Rehabilitation
Clinical guidelines in pelvic health universally endorse specialized neuromuscular physiotherapy as the first-line, highly effective treatment for reversing diastasis recti.
Download Clinical Efficacy PDF: The Efficacy of Deep Core Neuromuscular Training in the Resolution of Diastasis Recti Abdominis (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for post-partum rehabilitation.
The Rehab Mechanics Post-Partum Protocol
Healing a diastasis recti is not about pulling the muscles back together forcefully; it is about rebuilding the tension and density of the connective tissue between them.
Phase 1: Diaphragmatic and Pelvic Floor Integration
We must reseal the "canister" before we load it.
360-Degree Breathing: Re-training the diaphragm to expand outward into the lower ribs rather than pushing downward forcefully against the weakened abdominal wall.
Pelvic Floor Co-Contraction: Teaching the nervous system to automatically engage the pelvic floor muscles in perfect synchrony with the breathing cycle, creating a stable foundation for the core to pull against.
Phase 2: Transverse Abdominis (TvA) Activation
The TvA is your deepest abdominal muscle. It acts as a biological corset, wrapping horizontally around your waist.
Fascial Tensioning: When the TvA contracts properly, it physically pulls the two halves of the rectus abdominis closer together and creates dense, healthy tension across the healing linea alba.
Neuromuscular Re-education: Utilizing highly specific, low-level isometric holds (like the "supine marching" exercise) to ensure the TvA is firing before any superficial movement occurs.
Phase 3: Progressive Load and Functional Integration
Once the midline can handle tension without "coning," we begin to rebuild your real-world strength.
Anti-Extension and Anti-Rotation: Using resistance bands and stability balls to challenge the core to resist movement, safely building strength without creating outward abdominal bulging.
Mom-Specific Ergonomics: Training you how to safely hinge at the hips to lift your toddler, maneuver a stroller, and carry a heavy car seat without compromising your recovering abdominal wall.
Rebuild Your Foundation Today
You do not have to accept a weak core or chronic back pain as the permanent "price" of motherhood. Specialized, gentle, and highly targeted physiotherapy can restore the structural integrity of your abdomen.
Book a comprehensive perinatal core assessment with our specialized clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering accessible care in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.




Can Physiotherapy Cure Golfer's Elbow Without Stopping Weightlifting?
Yes. Physiotherapy effectively cures golfer's elbow by utilizing heavy slow resistance training, deep tissue release, and biomechanical correction of the wrist flexors. This active approach rebuilds degenerated tendon capacity, allowing you to lift weights safely without requiring complete rest or steroid injections.
The Grip Strength Dilemma in Urban Athletes
In Queen West and Liberty Village, the local fitness culture is intense. Between heavy barbell training, CrossFit, indoor rock climbing, and recreational golf, Toronto residents demand massive pulling power from their upper bodies.
However, this relentless demand on grip strength often results in a sharp, burning pain on the inside of the elbow—a condition medically known as Medial Epicondylitis, or "Golfer's Elbow." Despite the name, the vast majority of our patients with this condition have never swung a golf club; they are software developers, powerlifters, and construction workers.
When inner elbow pain strikes, the traditional advice is to stop lifting, ice the area, and wear a brace. But for an active urban professional, taking three months off from the gym is unacceptable and, clinically, it is the wrong approach. Complete rest causes tendons to atrophy and weaken. At Rehab Mechanics, we resolve Medial Epicondylitis not by resting the tendon, but by actively remodeling it to handle heavier loads.
Structural Analysis: The Mechanics of the Inner Elbow
To understand why passive rest fails to fix Golfer's Elbow, we must perform a detailed biomechanical analysis of the forearm flexors and the nature of tendinopathy.
The Flexor-Pronator Mass
Your forearm contains a complex network of muscles that control your wrist and fingers. The muscles responsible for bending your wrist forward (flexion) and turning your palm face down (pronation) all merge into a single, thick common tendon.
The Anatomical Anchor: This common flexor tendon anchors directly onto the medial epicondyle—the prominent bony bump on the inside of your elbow.
The Mechanical Overload: Every time you grip a heavy deadlift bar, perform a pull-up, or even type furiously on a non-ergonomic keyboard, massive tension is transferred through these muscles directly into that small bony attachment.
The Pathology of Tendinopathy
Golfer's elbow is rarely an acute, inflammatory "tendinitis." It is almost always a chronic, degenerative "tendinosis."
Failed Cellular Healing
When the flexor tendon is overloaded repetitively, it sustains microscopic tears.
The Chaotic Repair: Instead of laying down strong, perfectly parallel Type I collagen fibers to fix the tears, an exhausted body patches the area with weak, disorganized Type III scar tissue.
Angiofibroblastic Degeneration: The tendon physically thickens, loses its elasticity, and becomes infiltrated with highly sensitive, dysfunctional nerve endings and weak blood vessels.
The Valgus Stress Factor
In sports and lifting, poor shoulder or wrist mechanics often create "valgus stress"—a lateral outward pulling force on the elbow joint.
If your shoulder lacks external rotation during a heavy lift, your elbow is forced to flare out, violently yanking on the medial epicondyle and accelerating the tendon degeneration.
Primary Source Proof: Active Tendon Loading
Orthopedic research explicitly supports progressive, heavy mechanical loading over passive rest or corticosteroid injections for the long-term cure of chronic tendinopathies.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for tendon rehabilitation.
The Rehab Mechanics Treatment Protocol
To cure Golfer’s Elbow, we must break down the chaotic scar tissue and stimulate the growth of new, aligned collagen fibers. We achieve this through a rigorous, phased clinical pathway.
Phase 1: Pain Modulation and Neovascularization
Before we can aggressively load the tendon, we must alter the chemical environment and reduce acute pain.
Shockwave Therapy: Utilizing high-energy acoustic sound waves to literally shatter the fibrotic scar tissue at the medial epicondyle. This mechanical stimulus forces the body to grow new, healthy blood vessels (neovascularization) into the deadened tendon.
Myofascial Release: Applying deep, instrument-assisted soft tissue mobilization (IASTM) to the belly of the forearm flexors to release trigger points, instantly reducing the pulling tension on the elbow bone.
Phase 2: Isometric Loading (The Analgesic Phase)
We must introduce load to the tendon without moving the joint, which acts as a powerful pain reliever.
Heavy Isometrics: Having the patient hold a heavy dumbbell in a flexed wrist position without moving for 45-second intervals. This safely engages the muscle-tendon unit, signaling the brain to down-regulate pain sensitivity.
Phase 3: Eccentric and Heavy Slow Resistance (HSR)
This is where the permanent structural remodeling occurs.
Eccentric Wrist Flexion: Focusing specifically on the "lowering" phase of a wrist curl. Eccentric contractions physically pull the chaotic collagen fibers into perfectly parallel alignment, rebuilding the tendon's tensile strength.
Pronation/Supination Loading: Using offset weights (like a hammer or specialized club) to strengthen the rotational muscles of the forearm, which are critical for stabilizing the elbow during heavy lifting.
Phase 4: Kinetic Chain Integration
Finally, we must fix the faulty movement patterns that caused the overload.
Shoulder and Scapular Strengthening: Improving rotator cuff strength and mid-back mobility so the elbow no longer has to compensate for a weak shoulder during heavy pulling movements.
Reclaim Your Grip Strength
Do not let chronic elbow pain force you to abandon your fitness goals. A degenerated tendon requires mechanical rehabilitation, not a heavy brace and a bottle of ibuprofen.
Book a comprehensive upper extremity assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, right in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is a Specialized Physiotherapy Clinic Necessary After ACL Surgery?
Yes. Successful recovery from ACL reconstruction requires a specialized physiotherapy clinic. A clinical director manages the delicate phases of graft integration, overcomes arthrogenic muscle inhibition (quadriceps shutdown), and implements rigorous return-to-sport testing to prevent catastrophic re-injury.
The Reality of Post-Surgical Rehabilitation
Undergoing Anterior Cruciate Ligament (ACL) reconstruction surgery is a massive physical and psychological event. However, orthopedic surgeons frequently remind their patients of one critical truth: the surgery only accounts for 30% of the outcome; the remaining 70% depends entirely on the quality of your physical rehabilitation.
When patients in Toronto search for a "prime rehab center physical therapy" or "physiotherapy clinic in Toronto" following a major knee surgery, they cannot afford to settle for basic, generic care. Post-surgical rehabilitation is a highly complex, scientifically phased process. Pushing the knee too hard too early can stretch and ruin the new surgical graft. Conversely, moving too slowly leads to permanent scar tissue buildup and profound muscle atrophy.
At Rehab Mechanics, operating inside the Prime Medical Centre on Abell Street, we specialize in high-level, post-operative orthopedic rehabilitation. We bridge the critical gap between the operating table and your safe return to the sports and urban activities you love.
Structural Analysis: The Mechanics of ACL Recovery
To understand why specialized physiotherapy is non-negotiable, we must perform a clinical analysis of the biological and neurological trauma that occurs during and after ACL surgery.
The Biology of Graft Healing (Ligamentization)
When a surgeon rebuilds your ACL, they typically use a piece of tendon (either from your hamstring, patellar tendon, or a donor).
The Necrotic Phase: In the first few weeks after surgery, the new graft actually dies (necrosis) as it loses its original blood supply. It is incredibly weak during this phase.
Ligamentization: Over the next 6 to 12 months, the body slowly revascularizes the dead tissue and remodels it into a living ligament.
The Danger Zone: A specialized physiotherapist understands the exact timelines of this biological process. We implement precise biomechanical loads to stimulate healing while strictly avoiding shear forces that could snap the vulnerable, remodeling graft.
The Neurological Shutdown (Arthrogenic Muscle Inhibition)
Surgery involves massive trauma to the joint capsule.
The Quadriceps Failure
When the knee swells with post-surgical fluid, specialized stretch receptors inside the joint send panic signals to the spinal cord. To protect the knee from moving, the nervous system completely shuts off the neural drive to the quadriceps muscle (the front of your thigh).
The Atrophy Cascade
This is called Arthrogenic Muscle Inhibition (AMI). You can stare at your thigh and tell it to contract, but nothing happens. Within days, the muscle begins to atrophy rapidly. A standard clinic might just tell you to "do more leg lifts." A specialized clinical team uses advanced neuromuscular electrical stimulation (NMES) and biofeedback to force the nervous system to bypass the inhibition and "wake up" the quadriceps before permanent weakness sets in.
Primary Source Proof: Post-Operative Protocols
Advanced orthopedic research clearly dictates that structured, phased, and criterion-based physical therapy is the primary determinant for a successful return to pre-injury activity levels following ACL reconstruction.
Download Clinical Efficacy PDF: Evidence-Based Clinical Practice Guidelines for Rehabilitation Following ACL Reconstruction (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for post-surgical orthopedic rehabilitation.
The Rehab Mechanics Post-Surgical Protocol
We do not use a "wait and see" approach. We utilize a strict, criterion-based progression model, meaning you only advance to the next phase of rehab when your body proves it is structurally ready.
Phase 1: Acute Protection and ROM (Weeks 1-4)
The immediate goal is calming the surgical trauma.
Extension Restoration: Achieving full, 0-degree knee extension is the most critical milestone of early rehab to ensure normal walking mechanics.
Edema Management: Utilizing lymphatic massage and compression to flush surgical swelling out of the joint capsule.
Quad Reactivation: Aggressive use of manual therapy and electrical stimulation to overcome AMI and restore active quadriceps control.
Phase 2: Structural Loading and Hypertrophy (Weeks 5-12)
Once the knee is quiet, we must rebuild the atrophied muscle mass.
Closed Kinetic Chain Loading: Utilizing leg presses, step-ups, and targeted squats to safely load the knee joint without placing dangerous shear forces on the healing ACL graft.
Posterior Chain Fortification: Heavily strengthening the hamstrings and glutes, which act as the biological "brakes" to protect the ACL from forward stress.
Phase 3: Neuromuscular Control and Plyometrics (Months 3-6)
We transition from basic strength to athletic resilience.
Proprioceptive Training: Rebuilding the brain-to-knee connection using unstable surfaces, ensuring the muscles fire instantly to stabilize the joint during unexpected movements.
Linear Impact: Carefully introducing low-level plyometrics (hopping and landing mechanics) to teach the tendons how to absorb shock.
Phase 4: Return to Sport Testing (Months 6-9+)
We do not guess when you are ready to play. We test it.
Agility and Cutting: Introducing the chaotic, lateral movements required for sports like soccer, basketball, or tennis.
Isokinetic and Hop Testing: Ensuring your surgical leg has reached at least 90% of the strength and power output of your healthy leg before clearing you for full activity.

Reclaim Your Peak Performance
ACL surgery is a significant setback, but with elite physical rehabilitation, you can return stronger and more resilient than before your injury.
Secure the highest standard of post-surgical care. Book a comprehensive rehabilitation assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced orthopedic recovery in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care

Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Correcting Your Body Mechanics Eliminate Chronic Muscle Knots?
Yes. Correcting your fundamental body mechanics is the only permanent way to eliminate chronic muscle knots. While massage offers temporary relief, physiotherapy fixes the postural imbalances and joint stiffness that force muscles to chronically overwork, spasm, and form painful myofascial trigger points.
The Endless Cycle of Muscle Tension
Many Toronto professionals live with a constant, nagging companion: chronic muscle knots. Whether it is a burning golf-ball-sized knot between the shoulder blades, intense tightness at the base of the skull, or dense bands of tissue in the lower back, these knots can make sitting, sleeping, and exercising miserable.
When patients search for solutions related to "the body mechanics" or "remedial mechanics," they have usually already spent thousands of dollars on deep tissue massages, massage guns, and foam rollers. The story is always the same: the massage feels incredible for 24 hours, but by the time they return to their desk the next day, the knot is back, just as painful as before.
At Rehab Mechanics in Queen West, we understand that a muscle knot is not the root problem; it is a symptom of a mechanical overload. To permanently eliminate myofascial pain, you must stop treating the victim (the muscle) and start treating the culprit (your body mechanics).
Structural Analysis: The Science of a Muscle Knot
To break the cycle of chronic tension, we must perform a deep dive into what a muscle knot actually is and why your nervous system creates it.
Myofascial Trigger Points Explained
In clinical terms, a "muscle knot" is a myofascial trigger point.
The Micro-Spasm: A trigger point is a highly localized, hyper-irritable spot within a taut band of skeletal muscle. Essentially, a tiny segment of the muscle fiber has locked into a permanent, chemical spasm and refuses to let go.
Ischemia (Lack of Blood Flow): Because this tiny segment is permanently contracted, it acts like a clenched fist, squeezing the microscopic capillaries shut. This cuts off oxygen and blood flow to the tissue, causing the burning, aching sensation.
Why Do Trigger Points Form?
Muscles do not lock up maliciously. They lock up because your body mechanics are failing, and the nervous system is forcing them to work overtime to protect your joints.
The Overload Principle
Trigger points form when a muscle is subjected to sustained, low-level isometric overload.
The Compensatory Pattern
Consider the classic knot between the shoulder blades (the rhomboid muscles).
The Mechanical Flaw: If you sit with a hunched, forward-head posture, your heavy head is no longer balanced over your spine.
The Overworked Motor: Your poor rhomboid muscles now have to act like bungee cords, firing continuously for 10 hours a day to prevent your head from falling into your lap.
The Inevitable Failure: Muscles are meant to contract and relax. They cannot sustain a 10-hour contraction. Eventually, they fatigue, run out of cellular energy (ATP), and lock into painful trigger points.
Massaging the rhomboids relieves the ischemia temporarily, but the moment you sit back down with the same poor mechanics, the overload resumes instantly.
Primary Source Proof: Postural Biomechanics
Clinical rehabilitation research explicitly shows that combining manual trigger point therapy with postural strengthening yields vastly superior long-term results compared to manual therapy alone.
Download Clinical Efficacy PDF: The Efficacy of Corrective Exercise and Manual Therapy in the Treatment of Myofascial Pain Syndrome (Open Access Medical Review)
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for myofascial pain management.
The Rehab Mechanics Solution: Fixing the Machine
To permanently eliminate chronic knots, we implement a structural rehabilitation blueprint that resets your body's mechanics from the ground up.
1. Releasing the Brakes (Advanced Manual Therapy)
Before we can correct your posture, we must manually unlock the restrictive tissues holding you in a bad position.
Targeted Trigger Point Release: Applying sustained, ischemic compression directly to the nodule to force the muscle fibers to yield and restore localized blood flow.
Myofascial Release: Stripping the dense, shortened fascia on the front of the body (like the pectoral muscles) that are physically pulling your shoulders forward and overloading your back muscles.
2. Restoring Joint Arthrokinematics

Muscles attach to bones. If the joints are stiff, the muscles have to work twice as hard to move them.
Thoracic Spine Mobilization: We use specialized techniques to un-jam stiff mid-back joints. A mobile spine instantly takes the mechanical stress off the surrounding musculature.
Cervical Decompression: Gently restoring the natural curvature of the neck to allow the heavy weight of the skull to rest on the bones, rather than hanging off the muscles.
3. Neuromuscular Fortification
This is where the permanent cure happens. We must build a stronger machine.
Deep Core and Stabilizer Activation: Teaching the nervous system to utilize the deep, endurance-based stabilizing muscles (like the deep cervical flexors or transversus abdominis) rather than overworking the large, superficial movement muscles.
Postural Endurance Training: Prescribing specific exercises (like scapular retractions and face pulls) to build biological resilience, ensuring your muscles can effortlessly handle the mechanical demands of your daily life.
Stop Chasing the Pain
Do not accept chronic muscle tension as a normal part of aging or working at a desk. You can remodel your body's mechanics and live pain-free.
Book a comprehensive biomechanical assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
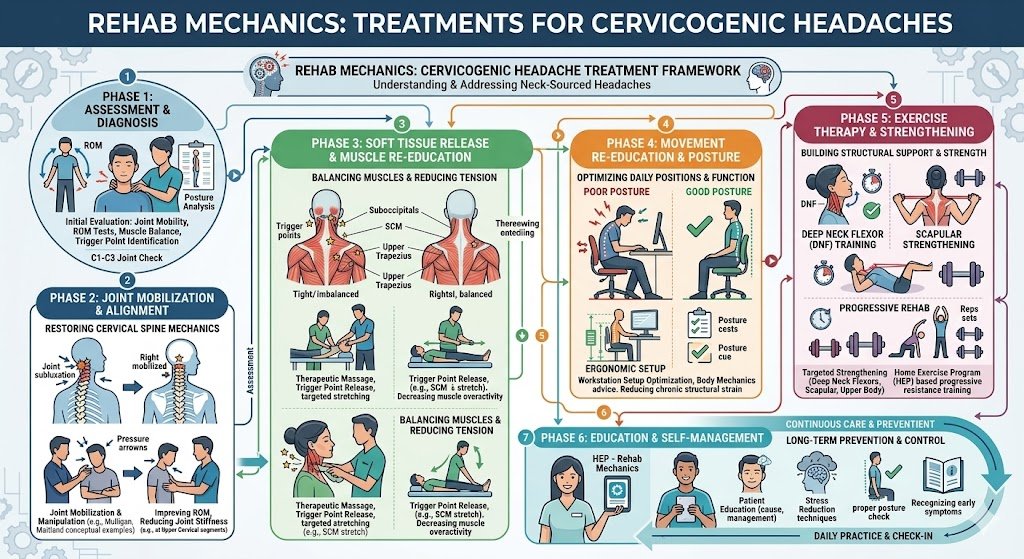
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Is Physiotherapy Effective for Hip Bursitis and Outer Thigh Pain?
Yes. Physiotherapy effectively treats hip bursitis by addressing the biomechanical root cause: gluteal weakness. By strengthening the hip stabilizers and releasing the IT band, physiotherapy eliminates the friction that inflames the bursa, providing permanent relief from lateral hip pain without the need for surgery.
The Urban Commuter's Ailment
Living and working in Queen West and downtown Toronto means walking—a lot. While this pedestrian lifestyle is fantastic for cardiovascular health, it places thousands of repetitive impact cycles on the joints of the lower body.
A frequent complaint we see at Rehab Mechanics from patients searching for "Queen West physiotherapy" is a sharp, burning pain on the outside of the hip. This pain often makes it agonizing to walk up the stairs of a streetcar, get up from a low desk chair, or even lie on your side to sleep at night.
Patients often self-diagnose this as arthritis, but in a vast majority of cases, it is Greater Trochanteric Pain Syndrome (GTPS), commonly known as Hip Bursitis. Ignoring this pain or relying solely on rest and ibuprofen allows the structural imbalances causing the friction to worsen over time.
Structural Analysis: What is Hip Bursitis?
To permanently eliminate outer hip pain, we must perform a structural analysis of the lateral hip anatomy and the mechanics of friction.
The Anatomy of a Bursa
Throughout your body, wherever a thick tendon slides over a bony prominence, nature has placed a "bursa." A bursa is a tiny, fluid-filled sac that acts as a low-friction gliding surface to protect the tendon from fraying against the bone.
The Greater Trochanter: This is the large, bony bump on the outside of your upper femur (thigh bone).
The Trochanteric Bursa: This sac sits directly over that bony bump, protecting it from the massive IT band and gluteal tendons that snap over it when you walk.
The Mechanics of Inflammation (GTPS)
Bursitis occurs when that fluid-filled sac becomes acutely inflamed and swollen. But why does it become inflamed?
The Weak Gluteus Medius
The primary cause of hip bursitis is a weakness in the gluteus medius muscle. This muscle sits on the side of your hip and its sole job is to keep your pelvis level when you are standing on one leg (which happens during every single step you take).
The Pelvic Drop and Friction
If your gluteus medius is weak (often from sitting at a desk all day), your pelvis drops on the opposite side every time you take a step.
The IT Band Snap: This pelvic drop alters the angle of your leg, causing your thick Iliotibial (IT) band to snap violently back and forth over the greater trochanter.
The Result: This repetitive snapping acts like sandpaper on the bursa, causing severe, chronic inflammation.
Primary Source Proof: Treating GTPS
Orthopedic clinical research demonstrates that targeted strengthening of the hip abductors (glutes) is vastly superior to passive treatments or corticosteroid injections for the long-term management of Greater Trochanteric Pain Syndrome.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for hip rehabilitation.
The Rehab Mechanics Treatment Protocol
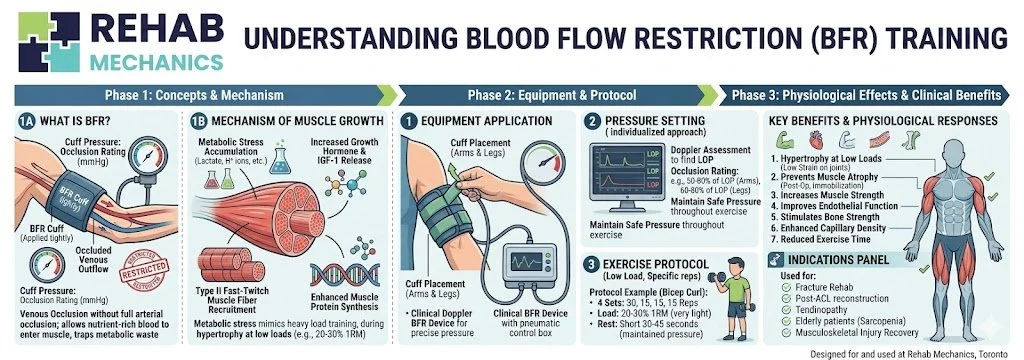
Treating hip bursitis is a delicate balance. We must reduce the acute friction while simultaneously strengthening the exact muscles that are currently causing the pain.
Phase 1: Unloading and Pain Management
The first step is to stop the bursa from being crushed.
Postural Modification: We teach you how to avoid postures that compress the bursa, such as crossing your legs while sitting or standing with your weight shifted entirely onto one hip.
Sleep Ergonomics: Providing strategies, like sleeping with a thick pillow between your knees, to prevent the top leg from dropping and stretching the IT band over the bursa at night.
Manual Soft Tissue Release: Our physiotherapists use targeted massage to release the hypertonic (overly tight) Tensor Fasciae Latae (TFL) muscle, reducing the tension on the IT band.
Phase 2: Isometric Activation
Because the tendons are inflamed, heavy movement hurts. We start with static strengthening.
Isometric Glute Loading: Exercises where the glute muscles contract hard without the joint actually moving. This builds strength and acts as a powerful, natural analgesic (pain reliever) for the tendon.
Phase 3: Dynamic Structural Fortification
Once the acute pain subsides, we rebuild the hip's shock-absorbing capacity.
Heavy Slow Resistance (HSR): We progress to heavy, controlled movements like side-lying hip abductions, banded clamshells, and eventually single-leg deadlifts.
Core and Pelvic Integration: Ensuring the deep core (transversus abdominis) fires in coordination with the glutes to stabilize the entire lumbo-pelvic region during the dynamic movements of city living.
Walk the City Without Pain
Do not let sharp hip pain restrict your mobility or ruin your sleep. The solution lies in correcting your biomechanics, not masking the pain.
Book a comprehensive hip assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible in Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.

His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Fix Rotator Cuff Pain Without Cortisone Injections?
Yes. Targeted physiotherapy can permanently resolve rotator cuff tendinopathy without repeated cortisone injections. By correcting scapular (shoulder blade) mechanics, restoring thoracic spine mobility, and progressively strengthening the rotator cuff tendons, physiotherapy eliminates the structural impingement causing the pain.
The "Weekend Warrior" Shoulder Epidemic
Parkdale and Queen West are home to an incredibly active demographic. From heavy lifting at local strength and conditioning gyms to weekend tennis matches and recreational baseball, the residents of Toronto push their upper bodies to the limit.
Consequently, searches for "physiotherapy Parkdale" frequently revolve around one notoriously stubborn injury: rotator cuff pain.
When you experience a sharp, catching pain in your shoulder while reaching into the backseat of your car, or a dull, throbbing ache that keeps you awake at night, the medical system often defaults to a quick fix. You may visit a walk-in clinic and receive a cortisone injection. While this provides temporary chemical relief, the pain almost always returns a few months later.
At Rehab Mechanics, we want patients to understand that chemical injections do not fix mechanical problems. To permanently eliminate shoulder pain, you must rebuild the structural integrity of the joint through advanced biomechanical physiotherapy.
Structural Analysis: The Mechanics of Shoulder Impingement
To understand why exercise cures the shoulder better than an injection, we must analyze the anatomy of the rotator cuff and the mechanics of "impingement."
The Anatomy of the Cuff
The rotator cuff is not a single muscle; it is a group of four small muscles (Supraspinatus, Infraspinatus, Teres Minor, and Subscapularis) that originate on your shoulder blade and wrap around the head of your upper arm bone (humerus).
The Primary Job: Their job is not to lift heavy weights. Their job is to pull the head of the humerus tightly into the shoulder socket, keeping the joint centralized and stable while your larger muscles (deltoids, pecs, lats) do the heavy lifting.
The Subacromial Space and Impingement
The tendons of the rotator cuff pass through a very narrow bony tunnel in the shoulder called the subacromial space.
The Postural Collapse
If you spend 40 hours a week hunched over a laptop, your chest muscles (pecs) become chronically tight, and your upper back muscles become weak. This pulls your shoulder blades forward and tilts them down.
The Mechanical Pinch
When the shoulder blade is tilted forward, that narrow subacromial tunnel becomes even smaller. Now, when you try to lift your arm to serve a tennis ball or press a dumbbell, the arm bone literally crushes the rotator cuff tendons against the roof of the shoulder blade.
This mechanical crushing causes micro-tears, severe inflammation, and eventual tendinopathy. A cortisone shot reduces the inflammation, but the moment you lift your arm again, the crushing resumes.
Primary Source Proof: Corticosteroids vs. Exercise Therapy
Extensive orthopedic research indicates that while corticosteroid injections offer short-term pain relief, progressive exercise therapy provides superior long-term functional outcomes and reduces the risk of tendon rupture.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for shoulder rehabilitation.
The Rehab Mechanics Rotator Cuff Protocol
To truly fix a rotator cuff, we must open up the subacromial space and build resilient, thick tendons. Our Parkdale and Queen West patients undergo a rigorous, three-phase protocol.
Phase 1: Creating Mechanical Space (Weeks 1-3)
Before we strengthen the cuff, we must stop the crushing.
Thoracic Mobilization: We use manual therapy to aggressively mobilize the mid-back. If your spine cannot extend, your shoulder blades cannot rotate backward.
Pectoral Release: Deep myofascial release on the pectoralis minor to allow the shoulder blades to sit back in a neutral, healthy position.
Pain Management: Utilizing clinical modalities (like TENS or gentle traction) to lower the acute inflammatory pain safely.
Phase 2: Scapular Stabilization (Weeks 4-6)
We must build a strong foundation. You cannot fire a cannon from a canoe.
Lower Trapezius Activation: Exercises designed to train the muscles at the bottom of the shoulder blade to pull it down and away from the impingement zone.
Serratus Anterior Strengthening: The "boxer's muscle" is crucial for keeping the shoulder blade glued to the ribcage during overhead movements.
Phase 3: Cuff Loading and Tissue Remodeling (Weeks 6+)
This is where the tendon is permanently repaired.
Eccentric Loading: Tendons heal best under tension. We use slow, controlled resistance band exercises to lengthen the rotator cuff muscles under load, stimulating the production of new, strong collagen fibers.
Proprioceptive Stabilization: Using unstable surfaces (like a kettlebell bottoms-up press) to force the rotator cuff to react instantly and centralize the joint during chaotic movements.
Stop the Cycle of Shoulder Pain
Do not let repeated cortisone injections deteriorate your tendon quality. Fix the biomechanics of your shoulder and return to your active lifestyle safely.
Book a comprehensive upper body assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible for Parkdale and Queen West residents.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care

Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Can Physiotherapy Fix Rotator Cuff Pain Without Cortisone Injections?
Yes. Targeted physiotherapy can permanently resolve rotator cuff tendinopathy without repeated cortisone injections. By correcting scapular (shoulder blade) mechanics, restoring thoracic spine mobility, and progressively strengthening the rotator cuff tendons, physiotherapy eliminates the structural impingement causing the pain.
The "Weekend Warrior" Shoulder Epidemic
Parkdale and Queen West are home to an incredibly active demographic. From heavy lifting at local strength and conditioning gyms to weekend tennis matches and recreational baseball, the residents of Toronto push their upper bodies to the limit.
Consequently, searches for "physiotherapy Parkdale" frequently revolve around one notoriously stubborn injury: rotator cuff pain.
When you experience a sharp, catching pain in your shoulder while reaching into the backseat of your car, or a dull, throbbing ache that keeps you awake at night, the medical system often defaults to a quick fix. You may visit a walk-in clinic and receive a cortisone injection. While this provides temporary chemical relief, the pain almost always returns a few months later.
At Rehab Mechanics, we want patients to understand that chemical injections do not fix mechanical problems. To permanently eliminate shoulder pain, you must rebuild the structural integrity of the joint through advanced biomechanical physiotherapy.
Structural Analysis: The Mechanics of Shoulder Impingement
To understand why exercise cures the shoulder better than an injection, we must analyze the anatomy of the rotator cuff and the mechanics of "impingement."
The Anatomy of the Cuff
The rotator cuff is not a single muscle; it is a group of four small muscles (Supraspinatus, Infraspinatus, Teres Minor, and Subscapularis) that originate on your shoulder blade and wrap around the head of your upper arm bone (humerus).
The Primary Job: Their job is not to lift heavy weights. Their job is to pull the head of the humerus tightly into the shoulder socket, keeping the joint centralized and stable while your larger muscles (deltoids, pecs, lats) do the heavy lifting.
The Subacromial Space and Impingement
The tendons of the rotator cuff pass through a very narrow bony tunnel in the shoulder called the subacromial space.
The Postural Collapse
If you spend 40 hours a week hunched over a laptop, your chest muscles (pecs) become chronically tight, and your upper back muscles become weak. This pulls your shoulder blades forward and tilts them down.
The Mechanical Pinch
When the shoulder blade is tilted forward, that narrow subacromial tunnel becomes even smaller. Now, when you try to lift your arm to serve a tennis ball or press a dumbbell, the arm bone literally crushes the rotator cuff tendons against the roof of the shoulder blade.
This mechanical crushing causes micro-tears, severe inflammation, and eventual tendinopathy. A cortisone shot reduces the inflammation, but the moment you lift your arm again, the crushing resumes.
Primary Source Proof: Corticosteroids vs. Exercise Therapy
Extensive orthopedic research indicates that while corticosteroid injections offer short-term pain relief, progressive exercise therapy provides superior long-term functional outcomes and reduces the risk of tendon rupture.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for shoulder rehabilitation.
The Rehab Mechanics Rotator Cuff Protocol
To truly fix a rotator cuff, we must open up the subacromial space and build resilient, thick tendons. Our Parkdale and Queen West patients undergo a rigorous, three-phase protocol.
Phase 1: Creating Mechanical Space (Weeks 1-3)
Before we strengthen the cuff, we must stop the crushing.
Thoracic Mobilization: We use manual therapy to aggressively mobilize the mid-back. If your spine cannot extend, your shoulder blades cannot rotate backward.
Pectoral Release: Deep myofascial release on the pectoralis minor to allow the shoulder blades to sit back in a neutral, healthy position.
Pain Management: Utilizing clinical modalities (like TENS or gentle traction) to lower the acute inflammatory pain safely.
Phase 2: Scapular Stabilization (Weeks 4-6)
We must build a strong foundation. You cannot fire a cannon from a canoe.
Lower Trapezius Activation: Exercises designed to train the muscles at the bottom of the shoulder blade to pull it down and away from the impingement zone.
Serratus Anterior Strengthening: The "boxer's muscle" is crucial for keeping the shoulder blade glued to the ribcage during overhead movements.
Phase 3: Cuff Loading and Tissue Remodeling (Weeks 6+)
This is where the tendon is permanently repaired.
Eccentric Loading: Tendons heal best under tension. We use slow, controlled resistance band exercises to lengthen the rotator cuff muscles under load, stimulating the production of new, strong collagen fibers.
Proprioceptive Stabilization: Using unstable surfaces (like a kettlebell bottoms-up press) to force the rotator cuff to react instantly and centralize the joint during chaotic movements.
Stop the Cycle of Shoulder Pain
Do not let repeated cortisone injections deteriorate your tendon quality. Fix the biomechanics of your shoulder and return to your active lifestyle safely.
Book a comprehensive upper body assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible for Parkdale and Queen West residents.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Should I Seek a Second Opinion if My Physiotherapy Isn't Working?
Yes. If you have not seen measurable improvement after six physiotherapy sessions, you should seek a second opinion. Prolonged, ineffective treatment often indicates a misdiagnosed biomechanical root cause. A clinical director can perform an advanced structural audit to correct the failed treatment trajectory.
The Frustration of Stalled Rehabilitation
Navigating the healthcare system in a major city like Toronto can be overwhelming. When patients search for specific queries like "Sanjay physiotherapist" or "expert physiotherapy clinic in Toronto," they are often doing so out of deep frustration. They have already been to a clinic, attended multiple sessions, and diligently done their generic band exercises, yet their pain remains unchanged.
This is a common narrative at Rehab Mechanics. Patients arrive at our Queen West clinic exhausted by a cycle of passive symptom management—where a practitioner simply applies a hot pack, hooks them up to an electrical stimulation machine, and sends them out the door in 20 minutes.
If your rehabilitation has plateaued, it does not mean your body is broken beyond repair. It usually means the structural diagnosis was incomplete. A second opinion from an experienced clinical director changes the perspective from treating the symptom to investigating the mechanical failure.
Structural Analysis: Why Physiotherapy Fails
To understand why a second opinion is valuable, we must perform a clinical analysis of why standard, high-volume physiotherapy often fails to yield long-term results.
1. Treating the Victim, Not the Culprit
The most common error in musculoskeletal medicine is treating the site of the pain rather than the source of the mechanical overload.
The Knee Pain Example: A patient presents with anterior knee pain. The first clinic diagnoses it as "patellar tendinitis" and aggressively massages and ices the knee for six weeks.
The Biomechanical Reality: The knee pain is just the "victim." The "culprit" is actually a stiff ankle joint and profound weakness in the gluteus medius. Because the ankle cannot bend, the knee absorbs extra shock; because the glute is weak, the knee caves inward.
The Result: Until the hip and ankle are rehabilitated, massaging the knee will never cure the pain.
2. Over-Reliance on Passive Modalities
There is a time and place for passive pain relief, but it is not a cure.
Passive Care: Interventions like TENS machines, ultrasound, heat, and ice only alter nerve signaling temporarily. They do not change tissue capacity.
Active Care: Tendons, ligaments, and muscles only heal and strengthen when they are subjected to mechanical load (resistance training). If your therapy does not progress to heavy, targeted loading, the tissue remains weak and vulnerable.
3. Lack of Interdisciplinary Integration
Chronic pain is rarely a simple, one-tissue problem.
The Silo Effect: If a patient has severe lumbar disc herniation causing sciatica, physical therapy alone might be too agonizing to endure.
The Prime Medical Centre Advantage: Because Sanjay operates Rehab Mechanics within the Prime Medical Centre on Abell Street, a second opinion here means access to medical doctors. We can coordinate anti-inflammatory medical interventions to create a "window of opportunity" where the patient can finally tolerate the physical exercises needed to heal.
Primary Source Proof: The Value of Advanced Assessment
Clinical research confirms that advanced biomechanical screening and individualized loading protocols vastly outperform generalized, passive treatment plans for chronic musculoskeletal pain.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for orthopedic rehabilitation.
Inside a Rehab Mechanics Second Opinion Assessment
When you book a second opinion with Sanjay or our senior clinical team, we throw out the old assumptions and start from scratch.
Phase 1: The Diagnostic Audit
We review your previous treatment plan to identify missing mechanical links.
Neurological Screening: Ruling out nerve root compression that may have been masquerading as a simple muscle strain.
Kinematic Mapping: Analyzing your movement patterns (gait, squatting, reaching) to see how your entire kinetic chain distributes force.
Phase 2: Advanced Soft Tissue and Joint Testing
We test the integrity of the tissues that your previous therapist may have missed.
Arthrokinematics: Assessing the microscopic glide of your joint capsules. A stiff joint capsule will inhibit muscle firing, rendering your strengthening exercises useless.
Fascial Tension: Identifying restrictive fascial bands that alter your posture and pull your skeleton out of alignment.
Phase 3: The Custom Blueprint
We do not hand out generic printouts. Your new rehabilitation plan is a precise, phased blueprint.
Neuromuscular Re-education: Teaching your brain to fire the correct muscles in the correct sequence.
Progressive Overload: Implementing heavy slow resistance (HSR) and eccentric loading to rebuild the biological capacity of your injured tissues.
Take Control of Your Clinical Outcomes
Do not accept chronic pain as your permanent reality just because one clinic failed to fix it. Human biomechanics is a complex science, and finding the right clinical expert makes all the difference.
Book a comprehensive second-opinion assessment with our team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible in the heart of Toronto's Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Why is it Critical to Find the Right "Physio Near Me" in Liberty Village?
Yes, finding the right "physio near me" in Liberty Village is critical for lasting pain relief. A high-quality clinic offers direct access to advanced manual therapy, custom corrective exercises, and interdisciplinary medical care, rather than relying on automated treatments or passive machines that fail to fix root biomechanical causes.
The Urban Grind and the Search for Relief
Liberty Village and Queen West are heavily populated by tech professionals, creatives, and urban commuters. While the area is incredibly vibrant, the lifestyle is demanding. Between 10-hour days hunched over a laptop, intense weekend fitness classes, and navigating the city, the human body takes a beating.

When chronic neck tension, lower back pain, or a sudden sports injury strikes, the immediate reaction is to open Google and search for "physio near me" or "physiotherapy Liberty Village."
However, all physiotherapy clinics are not created equal. Choosing the closest clinic based purely on a map pin can lead to frustrating, cookie-cutter care. At Rehab Mechanics, located just steps away at 68 Abell Street, we redefine what local physical therapy should look like. We reject automated, passive care in favor of an elite, human-centric, biomechanical approach to healing.
Structural Analysis: What Makes a Top-Tier Physiotherapy Clinic?
To ensure you are investing your time and health benefits effectively, you must understand the structural differences between a standard symptom-management clinic and an advanced biomechanical rehabilitation center.
The Problem with Passive Symptom Management
Many high-volume clinics operate on a passive model. You walk in, receive 15 minutes of a hot pack, 10 minutes on a TENS (electrical stimulation) machine, and a sheet of generic stretches.
The Illusion of Healing: Passive treatments feel good temporarily because they flood the area with blood and block pain receptors.
The Inevitable Relapse: The moment you return to your desk or your gym, the pain returns. Why? Because the mechanical flaw—the weak core, the stiff joint, the poor posture—was never actually corrected.
The Rehab Mechanics Approach: Active Biomechanics
When you search for "Sanjay Physiotherapist" or visit our Queen West clinic, you are opting for active, structural correction.
Advanced Manual Therapy
Our Registered Physiotherapists use their hands to physically alter tissue state and joint mechanics.
Myofascial Release: Breaking down dense, fibrotic scar tissue in chronically tight muscles like the pecs and upper traps (the primary drivers of "Tech Neck").
Joint Mobilization: Restoring the micro-gliding motions of the spinal facet joints and peripheral joints, instantly relieving nerve compression and restoring full range of motion.
Corrective Exercise Prescription
Rehabilitation is education. We do not just stretch you; we rebuild you.
Neuromuscular Re-education: Teaching your brain to fire dormant stabilizing muscles (like the deep cervical flexors or the transversus abdominis).
Progressive Loading: Utilizing heavy, slow resistance to build tendon capacity, ensuring your body can handle the chaotic forces of the Toronto lifestyle without breaking down.
Primary Source Proof: Active vs. Passive Rehab
Clinical evidence overwhelmingly supports active exercise and manual therapy over passive modalities for long-term resolution of musculoskeletal pain.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for orthopedic rehabilitation.
The Advantage of the Prime Medical Centre Location
The final factor in choosing the right "physio near me" is the clinic's integration into the broader healthcare system.
Rehab Mechanics operates directly inside the Prime Medical Centre. This provides Liberty Village and Queen West residents with an unparalleled level of interdisciplinary care.
Physician Co-Management: If your injury requires prescription pain management or diagnostic imaging (X-rays/ultrasounds), we collaborate directly with the medical doctors down the hall.
Streamlined Care: No waiting weeks for referrals or carrying paperwork across the city. Your medical and physical rehabilitation happens under one roof.
Specialized Modalities: We offer access to advanced interventions like Shockwave Therapy and custom orthotics dispensing, ensuring we have the exact tools required for complex pathologies.
Stop Settling for Temporary Relief
If you live or work in Liberty Village or Queen West, you deserve healthcare that works as hard as you do. Stop relying on pain medication and temporary fixes. Address the biomechanical root cause of your pain.
Book a comprehensive, one-on-one assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.

Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Should I Go to a Specialized MVA Rehab Clinic in Toronto After a Car Crash?
Yes. Attending a specialized MVA rehab clinic in Toronto is critical after an auto accident. Specialized clinics do not just treat acute physical trauma like whiplash; they expert handle the complex Ontario HCAI billing systems, OCF treatment plans, and interdisciplinary medical coordination required by auto insurers.
The Hidden Complexities of Auto Accidents
When a motor vehicle accident happens on the busy streets of Toronto, the immediate focus is usually on the vehicle damage and emergency room visits. However, the real challenge for patients begins in the weeks following the crash.
As adrenaline wears off, conditions like Whiplash Associated Disorders (WAD), severe concussions, and radiating spinal pain begin to set in. Searching for "auto rehab" or an "MVA rehab clinic Toronto" reveals a critical truth: treating a car accident injury is fundamentally different from treating a sports injury.
It requires a clinic that understands both the violent biomechanics of high-speed trauma and the intricate, highly regulated Ontario statutory accident benefits schedule. At Rehab Mechanics in Queen West, we combine advanced neurological and orthopedic rehabilitation with seamless administrative support to guide you through the MVA recovery maze.
Structural Analysis: The Unique Pathology of MVA Trauma
To understand why a specialized clinic is necessary, we must analyze how motor vehicle collisions damage the human body differently than everyday wear and tear.
The Physics of a Collision
In a rear-end collision, massive kinetic energy is transferred directly into your spine in a fraction of a second.
The Whiplash Mechanism: Your body is pushed forward by the seat, but your head remains momentarily stationary. This violently shears the lower cervical discs. The head is then whipped backward (hyperextension) and forward (hyperflexion).
Multi-System Trauma: This sequence does not just pull a single muscle. It micro-tears ligaments, jams spinal facet joints, stretches nerve roots, and can cause mild traumatic brain injuries (concussions) as the brain impacts the inside of the skull.
The Importance of Grading the Injury
A standard sports clinic might just apply a heat pack to a sore neck. A specialized MVA clinic meticulously grades the injury according to standardized medical protocols (like the Quebec Task Force classifications for WAD).
WAD Grades and Treatment Trajectories
WAD I: Neck pain and stiffness with no physical signs.
WAD II: Neck pain with decreased range of motion and pinpoint tenderness (the most common).
WAD III: Neck pain accompanied by neurological signs (numbness, tingling, or weakness in the arms).
Preventing Chronic Pain Syndrome
If a WAD II or III injury is not aggressively and correctly rehabilitated within the first 12 weeks, the body heals the micro-tears with disorganized, rigid scar tissue. This leads to permanent joint restriction, chronic cervicogenic headaches, and long-term disability.
Primary Source Proof: MVA Clinical Guidelines
Our MVA rehabilitation protocols are strictly governed by provincial regulations and peer-reviewed trauma research.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for motor vehicle accident rehabilitation.
The Rehab Mechanics MVA Advantage
Choosing an MVA-specialized clinic like Rehab Mechanics provides three distinct advantages that ensure a full physical and financial recovery.
1. Interdisciplinary Medical Integration
Because we operate inside the Prime Medical Centre, we provide comprehensive, multi-tiered care. If your whiplash is accompanied by severe dizziness or neurological deficits, we can instantly coordinate with on-site physicians for advanced imaging or specialized pharmacological pain management, ensuring your medical file is robust and complete from day one.
2. Advanced Physical Modalities
We utilize clinical-grade technology to accelerate tissue healing beyond standard exercise.
Shockwave Therapy: To break down stubborn scar tissue in the neck and shoulders.
Targeted Joint Mobilization: Gentle, precise manual therapy to un-jam locked cervical facet joints and decompress irritated nerve roots.
Vestibular Rehabilitation: Specific protocols to address dizziness, vertigo, and post-concussion syndrome caused by the crash.
3. Mastering the Administrative Maze (FSRA & HCAI)
The Ontario auto insurance system (regulated by FSRA) is notoriously stressful. If paperwork is filed incorrectly, your treatment funding can be instantly cut off.
Direct Billing: We bill auto insurers directly through the Health Claims for Auto Insurance (HCAI) portal, meaning no out-of-pocket expenses for you.
OCF Documentation: We meticulously draft and submit all necessary Treatment Plans (OCF-18) and disability certificates to your adjuster, fighting to ensure your care is fully funded.
Focus on Healing, Not Paperwork
Do not let a car accident dictate your physical future or drain your energy with insurance battles. Secure specialized, interdisciplinary care immediately following your collision.
Book a comprehensive MVA assessment with our team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, easily accessible by the Queen streetcar.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.

Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Does 'Human Mechanics' Physical Therapy Fix Running Pain in Trinity Bellwoods?
Yes. Applying a 'human mechanics' approach to physical therapy permanently fixes running pain by addressing the entire kinetic chain. Instead of just icing a sore knee, this approach analyzes foot strike, pelvic drop, and hip strength to eliminate the biomechanical friction causing the injury.
The Parkdale and Trinity Bellwoods Active Lifestyle
Trinity Bellwoods Park and the surrounding Parkdale neighborhoods represent the beating heart of Toronto's active, outdoor culture. From recreational jogging clubs to intense weekend tennis matches and cycling, the residents here demand a lot from their bodies.
However, high activity levels lead to high rates of overuse injuries. When runners search for a "physiotherapist Trinity Bellwoods" or "human mechanics physical therapy," they are usually dealing with stubborn conditions like IT Band Syndrome, runner's knee, or Achilles tendinopathy that refuse to heal with simple rest.
At Rehab Mechanics, located just down the street in Queen West, we specialize in the science of human movement. We understand that pain in your knee is rarely a knee problem; it is a mechanical failure in how your body absorbs the shock of the pavement.
Structural Analysis: Deconstructing Human Mechanics
To permanently resolve sports injuries, we must move away from the outdated "rest and ice" model and embrace a structural, mechanical analysis of human anatomy.
The Body as a Machine
In the context of physical therapy, human mechanics (or biomechanics) is the study of your bones as levers, your joints as hinges, and your muscles as the motors and brakes that control them.
The Engine: Your glutes and hamstrings provide the propulsive force to push you forward.
The Brakes: Your quadriceps and calf muscles undergo "eccentric" contractions to absorb shock and decelerate your body weight when you land.
The Suspension System: Your foot arch and knee joint compress to absorb the kinetic energy of striking the ground.
Identifying the Mechanical Failure
When a runner experiences pain, it means one of these mechanical systems has failed, forcing another part of the machine to absorb a dangerous amount of stress.
The Pelvic Drop (Trendelenburg Sign)
One of the most common mechanical failures in runners is a weak gluteus medius (the muscle on the side of the hip).
The Function: When you run, you spend most of your time balancing on one leg. The gluteus medius must fire intensely to keep your pelvis level.
The Collapse: If it is weak, your pelvis drops on the opposite side.
The Knee as the Victim
When the pelvis drops, the femur (thigh bone) rotates inward. This violently twists the knee joint, grinding the kneecap against the bone (Runner's Knee) and yanking aggressively on the IT Band. The knee hurts, but the "human mechanics" failure is entirely at the hip.
Primary Source Proof: Running Kinematics
Our clinical approach to treating running pathologies is heavily backed by sports science and kinematic research.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for running-related rehabilitation.
The Rehab Mechanics Treatment Protocol
Restoring your human mechanics requires a phased, active rehabilitation protocol. Here is how we get Trinity Bellwoods runners back to peak performance:
1. Advanced Soft Tissue Mobilization
Before we can strengthen the weak muscles, we must release the structural brakes.
Myofascial Release: We use targeted manual therapy to release hyperactive muscles (like the Tensor Fasciae Latae or tight hip flexors) that are pulling your skeleton out of alignment.
Joint Mobilization: Ensuring the ankle joint has adequate dorsiflexion, which is critical for absorbing shock during running.
2. Targeted Structural Strengthening
This is the core of the mechanical fix. We must rebuild the muscular brakes of your lower body.
Gluteus Medius Activation: We use targeted, isolated exercises (like heavy lateral band walks and single-leg deadlifts) to rebuild pelvic stability.
Eccentric Loading: Building the capacity of the quadriceps and Achilles tendons to absorb the heavy shock of downhill running without irritating the tissue.
3. Gait Retraining and Load Management
Once the tissue is healed, we must fix the way you move.
Cadence Manipulation: Analyzing your running stride and often increasing your step rate (cadence) slightly, which drastically reduces the impact forces on the knee joint.
Return-to-Run (RTR) Scheduling: Prescribing exact running intervals to progressively reload the tendons safely without triggering an inflammatory relapse.
Get Back to the Park, Pain-Free
If you are dealing with sharp pain that ruins your runs or weekend sports, stop relying on passive rest. Physiotherapy offers a clear, mechanical solution to your biomechanical problem.
Book a movement assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, just a short walk or streetcar ride from Trinity Bellwoods and Parkdale.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Rehab Mechanics inside Prime Medical Centre
Should I Get Physiotherapy Inside the Prime Medical Centre on Abell Street?
Yes. Receiving physiotherapy inside the Prime Medical Centre on Abell Street ensures seamless, interdisciplinary care. By co-locating with medical doctors, physiotherapists can instantly coordinate diagnostic imaging, integrate pharmacological pain management, and accelerate your structural rehabilitation without the delays of a fragmented healthcare system.
The Advantage of Integrated Healthcare in Queen West
Navigating the healthcare system in Toronto can be an exhausting experience, especially when you are suffering from acute or chronic pain. A common frustration for patients is the "silo effect"—visiting a family doctor at one clinic for a prescription, waiting weeks for an X-ray at a different facility, and then traveling to a separate physiotherapy clinic where the practitioner has no direct communication with your physician.
When you search for "Prime Medical Centre Abell" or "Abell Clinic," you are looking for convenience, but you are also tapping into the gold standard of modern healthcare: the interdisciplinary model.
Rehab Mechanics operates directly inside the Prime Medical Centre at 68 Abell Street in Queen West. This strategic co-location allows us to bridge the gap between systemic medical care and biomechanical physical rehabilitation, providing you with a unified, highly efficient recovery pathway.
Structural Analysis: Medical vs. Mechanical Pain Management
To understand why integrated care is superior, we must analyze the two distinct angles from which complex injuries must be treated: the medical (chemical) and the mechanical (structural).
The Medical Foundation (Physician's Role)
When you suffer a severe injury, such as an acute disc herniation or a severe joint sprain, the immediate barrier to movement is chemical inflammation and neurological pain.
Diagnostic Imaging: Physicians can immediately order X-rays or ultrasound imaging to rule out fractures or severe structural tearing.
Pharmacological Intervention: Doctors can prescribe targeted NSAIDs, muscle relaxants, or administer intra-articular corticosteroid injections to rapidly drop the body's acute pain threshold.
Systemic Screening: Ensuring that your back or joint pain is not a "red flag" symptom of an underlying systemic illness.
The Mechanical Correction (Physiotherapist's Role)
While medical interventions block the pain signals and reduce swelling, they do not correct the biomechanical failure that caused the injury in the first place. That is the realm of physiotherapy.
Biomechanical Rebuilding
Once the physician manages the acute pain, the physiotherapist takes over to rebuild the joint's integrity.
The "Window of Opportunity"
This is where co-location is critical. If a doctor provides a pain-relieving injection, it creates a temporary "window of opportunity" where the patient is pain-free enough to exercise. Because we are in the same building, we can instantly initiate targeted joint mobilizations and deep-core strengthening to permanently fix the mechanics before the injection wears off.
Primary Source Proof: Interdisciplinary Efficacy
Extensive clinical literature proves that multidisciplinary biopsychosocial rehabilitation is vastly superior to standard, isolated medical care for complex musculoskeletal pain.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for integrated pain management.
The Tangible Benefits of the Abell Street Clinic
Operating within the Prime Medical Centre on Abell Street allows us to provide a seamless patient experience that standalone clinics simply cannot match.
1. Instant Clinical Communication
If our physiotherapists identify a neurological "red flag" during a physical assessment (such as sudden numbness, radiating nerve pain, or foot drop), we do not have to fax a report and wait weeks for a response. We can walk down the hall, consult directly with a physician, and expedite the necessary medical interventions.
2. Streamlined Treatment Plans for Auto & Work Injuries
For patients dealing with Motor Vehicle Accidents (MVA) or WSIB claims, paperwork is a massive hurdle. By having your medical management, pharmacological needs, and physical rehabilitation housed under one collaborative roof, your OCF treatment plans and return-to-work documentation are handled efficiently and congruently.
3. Holistic Patient Convenience
Chronic pain takes a massive psychological toll. Traveling to multiple appointments across Toronto adds to that stress. Our clinic at 68 Abell Street is easily accessible by the Queen streetcar, offering a centralized hub where you can see your doctor and your physiotherapist in a single trip.
Experience Coordinated Care at Rehab Mechanics
Stop bouncing between disconnected healthcare providers. Experience the efficiency and superior clinical outcomes of an integrated medical model.
Book your physiotherapy assessment today. We are located right inside the Prime Medical Centre at 68 Abell Street in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community

Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Biomechanics assessment at Queen West physio clinic
Can a Biomechanics Assessment at a Queen West Physiotherapy Clinic Prevent Injuries?
Yes. A professional biomechanics assessment in Toronto identifies hidden muscular imbalances and joint restrictions before they cause severe injuries. By mapping your specific movement patterns, a physiotherapist can correct faulty mechanics, optimizing your kinetic chain for pain-free running, lifting, and daily urban living.
The High Cost of Faulty Movement Patterns
In vibrant, active neighborhoods like Queen West and Liberty Village, residents are constantly on the move. Whether you are cycling down Wellington Street, running along the waterfront, or pushing through a heavy strength training session at a local gym, your body is subjected to massive mechanical forces every single day.
When you search for "biomechanics Toronto," you are looking for a solution that goes beyond basic pain relief. You are looking for human engineering. Injuries rarely happen by accident. An Achilles tendon tear or a herniated disc is usually the final, catastrophic result of thousands of subtle, faulty, repetitive movements.
At Rehab Mechanics, we specialize in identifying these mechanical flaws before they lead to tissue failure. Our biomechanical assessments analyze the human body as a complex machine of levers and pulleys, ensuring every component is carrying its exact share of the load.
Structural Analysis: The Kinetic Chain in Action
To understand the value of a biomechanical assessment, we must break down how your body distributes physical stress.
The Principle of Interdependence
Your body does not operate as a series of isolated joints; it operates as a deeply connected "kinetic chain."
The Upward Ripple: A structural problem in your foot arch will inevitably dictate how your knee rotates. A stiff mid-back will force your shoulder to overcompensate.
The Brain's Workaround: Your nervous system prioritizes getting the job done. If a primary muscle (like your glute) is weak, your brain will instantly recruit a secondary muscle (like your lower back) to perform the movement.
The Breakdown: These "compensatory patterns" keep you moving in the short term, but they severely overload secondary tissues, leading to chronic pain and inevitable joint breakdown.
Ground Reaction Forces and Shock Absorption
Every time your foot strikes the Toronto pavement, shockwaves travel up your leg. A clinical assessment analyzes how efficiently your body absorbs and dissipates these ground reaction forces.
The Ankle-Knee Connection
If you lack dorsiflexion (the ability to pull your toes toward your shin) due to tight calves, your body must find that range of motion elsewhere.
Forced Pronation
To get your foot flat on the ground, your arch is forced to collapse inward (overpronation). This inward collapse violently rotates your tibia (shin bone), placing massive torsional shear stress on the meniscus and ACL in the knee. The knee pain is just a symptom; the stiff ankle is the biomechanical root cause.
Primary Source Proof: Preventative Kinematics
Our preventative screening protocols are deeply rooted in advanced kinematic research and sports medicine data.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for biomechanical screening.
Inside a Rehab Mechanics Biomechanical Assessment
When you book an assessment at our Queen West clinic, we conduct a top-to-bottom structural audit. We do not just look at where it hurts; we look at how you move.
1. Static Postural and Structural Mapping
Before you even take a step, your resting posture provides critical data.
Leg Length Discrepancies: Identifying structural differences that tilt the pelvis.
Pelvic Alignment: Checking for anterior or posterior tilts that alter lumbar spine mechanics.
Scapular Positioning: Assessing for winging or forward head posture indicative of upper crossed syndrome.
2. Comprehensive Joint Range of Motion (ROM) Testing
We isolate every major joint to ensure it has the requisite mobility to perform safely.
Hip Internal/External Rotation: A stiff hip forces the lower back to twist excessively during sports, leading to disc injuries.
Thoracic Spine Extension: Necessary for safe overhead lifting and optimal shoulder health.
3. Dynamic Functional Movement Screening
We watch how your nervous system coordinates complex, multi-joint movements under load.
Overhead Squat Analysis: Reveals tightness in the lats, weakness in the core, and mobility restrictions in the hips and ankles simultaneously.
Single-Leg Loading: Squatting on one leg instantly highlights gluteal weakness (indicated by the knee caving inward, known as knee valgus).
Gait and Stride Analysis: We evaluate your strike pattern, cadence, and pelvic drop to identify inefficiencies in your walking or running stride.
Optimize Your Human Mechanics Today
Do not wait for a catastrophic injury to force you into a clinic. Identify the weak links in your kinetic chain now, and build a more resilient, efficient body.
If you are searching for advanced "biomechanics Toronto," book a comprehensive structural assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Chronic headaches post accident
Can Physiotherapy Relieve Chronic Headaches After a Car Accident?
Yes. Post-accident headaches are often cervicogenic, originating from trauma to the neck spine. Physiotherapy eliminates these headaches through targeted cervical joint mobilization, suboccipital release, and deep neck flexor strengthening, addressing the biomechanical root cause rather than masking symptoms with medication.
The Hidden Epidemic of MVA Headaches
Motor vehicle accidents (MVAs) in Toronto traffic are incredibly common. While the immediate focus is often on visible injuries, one of the most debilitating and frequently misunderstood consequences of a rear-end collision is the onset of chronic, unrelenting headaches.
Patients often assume these headaches are standard migraines or a permanent consequence of a mild concussion, leading them to rely heavily on daily pain medication. However, if your headaches started following a whiplash injury, they are highly likely to be "Cervicogenic Headaches."
At Rehab Mechanics, we specialize in complex motor vehicle accident claims and rehabilitation. We understand that cervicogenic headaches are a mechanical problem originating in the cervical spine. By identifying the exact spinal segments damaged during the crash, physiotherapy can permanently resolve the pain patterns that medication only temporarily hides.
Structural Analysis: The Mechanics of a Cervicogenic Headache
To understand how a neck injury causes head pain, we must perform a detailed neurological and biomechanical analysis of the upper cervical spine.
The Whiplash Mechanism
During a rear-end collision, the head is violently whipped backward (hyperextension) and then forward (hyperflexion) in a fraction of a second.
Tissue Tearing: This rapid whipping action micro-tears the ligaments, joint capsules, and deep muscles of the upper neck (specifically the C1, C2, and C3 vertebral levels).
Facet Joint Impingement: The delicate facet joints that connect the vertebrae are jammed together, causing acute inflammation and joint locking.
The Neurological Connection
A cervicogenic headache literally translates to a "headache originating from the neck."
The Trigeminal-Cervical Nucleus: The nerves that supply the upper three segments of your neck share a massive sensory relay center in your brainstem with the Trigeminal nerve (which supplies sensation to your face, forehead, and head).
Referred Pain: When the joints and muscles of the upper neck are damaged and inflamed from a crash, they send distress signals to this relay center. The brain misinterprets these signals, "feeling" the pain radiating up over the skull, behind the eyes, or wrapping around the temples like a tight band.
The Role of the Suboccipital Muscles
Just beneath the base of your skull lies a cluster of tiny, incredibly dense muscles called the suboccipitals.
The Muscle-Dura Bridge
During an MVA, these muscles lock into severe spasms to protect the spinal cord. Because some of these muscles have direct connective tissue links to the dura mater (the pain-sensitive outer covering of the brain), chronic spasms in the suboccipitals physically pull on the brain's lining, generating severe, throbbing tension headaches.
Primary Source Proof: Cervicogenic Efficacy
Clinical neurology and musculoskeletal guidelines confirm that physical manipulation and targeted exercise are vastly superior to pharmacological management for cervicogenic headaches.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for post-concussion and whiplash rehabilitation.
The Rehab Mechanics Treatment Protocol
Treating MVA-induced headaches requires absolute precision. We do not apply heavy, aggressive cracking; we use highly specific, gentle techniques to restore upper cervical biomechanics.
1. Advanced Joint Mobilization
We must un-jam the locked vertebral segments.
C1-C2 Mobilization: The physiotherapist applies gentle, sustained gliding pressure to the top vertebrae of the neck to restore normal rotational mechanics. By freeing the joint, we instantly relieve the pressure on the compressed cervical nerves.
Traction Techniques: Utilizing manual traction to decompress the cervical discs and open up the neural foramina (the holes where the nerves exit the spine).
2. Myofascial and Trigger Point Release
Releasing the soft tissue "stranglehold" on the nerves and blood vessels.
Suboccipital Release: Deep, sustained pressure applied to the base of the skull to melt away the dense spasms pulling on the dura mater.
Upper Trapezius and Levator Scapulae Deactivation: Addressing the large neck muscles that refer pain up the side of the neck and behind the ears.
3. Neuromuscular Re-education
Once the joints are moving and the muscles are relaxed, we must rebuild the neck's stabilizing system to prevent the headaches from returning.
Deep Cervical Flexor Training: The crash inevitably weakens the small muscles in the front of the neck. We use specific micro-movements (like chin tucks) to reactivate these stabilizers, taking the workload off the overworked muscles at the back of the skull.
Postural Endurance: Rebuilding the endurance of the mid-back to ensure the head sits properly over the shoulders, preventing the "forward head" posture that triggers chronic tension.
Navigating Ontario Auto Insurance
Dealing with insurance after a crash is stressful. As a specialized MVA rehab clinic, we handle the administrative burden. We submit comprehensive OCF treatment plans directly to your auto insurer through the HCAI portal, allowing you to focus entirely on eliminating your headaches.
If you are suffering from daily headaches following a car accident, do not settle for a life of pain medication. Book a comprehensive neurological and biomechanical assessment with our team today. We are located inside the Prime Medical Centre at 68 Abell Street.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.

Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Dreading potential surgery: how physio can help with beneficial avoidance
Can Physiotherapy Prevent Knee Replacement Surgery for Osteoarthritis?
Yes. Evidence-based physiotherapy significantly delays or prevents knee replacement surgery. By strengthening the quadriceps, improving joint mobility, and utilizing advanced modalities, physiotherapy reduces joint friction, manages chronic inflammation, and restores pain-free mobility in osteoarthritic knees.
Re-Thinking "Bone on Bone" Pain
A diagnosis of knee osteoarthritis (OA) often sounds like a definitive, surgical sentence. Patients are frequently told their knee is "bone on bone" and that a total knee replacement is the only eventual solution. This rhetoric causes immense fear, leading patients to stop moving entirely to "save" whatever cartilage they have left.
This is the worst possible strategy. Total rest accelerates the degradation of the joint.
At Rehab Mechanics, operating inside the Prime Medical Centre on Abell Street, we work directly alongside physicians to co-manage osteoarthritis. Our clinical data and daily practice prove that the severity of cartilage loss on an X-ray does not accurately dictate the amount of pain a patient will experience. By improving the biomechanical support system around the joint, physiotherapy can drastically reduce OA pain, restore function, and push the need for surgery back by years—or eliminate it entirely.
Structural Analysis: The Mechanics of Osteoarthritis
To understand how physiotherapy fights osteoarthritis, we must first understand the mechanical environment of the knee joint.
The Pathology of OA
Osteoarthritis is not merely "wear and tear." It is an active, whole-joint disease characterized by the breakdown of articular cartilage, changes to the underlying bone, and chronic inflammation of the synovial membrane.
Cartilage Degradation: The smooth, slippery cartilage that coats the ends of the femur and tibia thins out, increasing friction.
Osteophyte Formation: The body attempts to stabilize the failing joint by growing bone spurs (osteophytes), which can restrict movement and cause pinching pain.
Synovitis: The joint lining becomes inflamed, producing excess fluid (swelling) and releasing pain-mediating chemicals.
The Biomechanical Solution: Muscular Offloading
If the cartilage padding is gone, how can physiotherapy stop the pain? The answer lies in the muscles.
The Role of the Quadriceps
Your quadriceps (front thigh muscles) are the primary shock absorbers for your knee. They act as a massive braking system every time you take a step, absorbing up to 70% of the impact forces before they ever reach the knee joint.
The Cycle of Weakness
When the knee hurts, the brain subconsciously inhibits the quadriceps to prevent you from using the leg. The muscle rapidly shrinks (atrophies).
Once the quad is weak, 100% of the walking impact bypasses the muscle and slams directly into the arthritic, degraded bone. This causes more pain, which causes more weakness, creating a devastating downward spiral. Physiotherapy breaks this cycle.
Primary Source Proof: Non-Operative Efficacy
Major international orthopedic guidelines strongly mandate that comprehensive physiotherapy and exercise must be exhausted before surgical intervention is considered for knee OA.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for orthopedic rehabilitation.
The Interdisciplinary Protocol at Prime Medical Centre
Treating a degenerative disease requires a highly coordinated approach. Because we operate within the Prime Medical Centre, we seamlessly blend medical management with aggressive physical rehabilitation.
1. Medical Inflammation Management
Before we can strengthen the joint, we must lower the acute pain threshold.
Physician Co-Management: The medical doctors on-site may utilize targeted NSAIDs or administer intra-articular injections (such as corticosteroids or hyaluronic acid/viscosupplementation) to dramatically reduce synovial inflammation.
The Window of Opportunity: These injections do not cure the disease, but they create a critical 3-to-6 month "window of opportunity" where the knee is pain-free enough to tolerate intense physiotherapy.
2. Joint Mobilization and Swelling Reduction
Our physiotherapists begin by restoring the mechanical space in the joint.
Manual Traction: Gently pulling the joint surfaces apart to encourage the flow of synovial fluid, which lubricates the joint and nourishes the remaining cartilage.
Knee Extension Restoration: A knee that cannot straighten fully causes severe limping and rapid joint wear. We use targeted manual therapy to break down capsule stiffness and restore full extension.
3. Progressive Load and Strength Training
This is the long-term cure for OA pain. We must build a muscular brace around the bone.
Isolated Quadriceps Loading: Utilizing closed-kinetic-chain exercises (like leg presses, wall sits, and step-ups) to rebuild the quad muscle without applying shearing force to the kneecap.
Gluteal and Hip Strengthening: The hip controls the alignment of the knee. By strengthening the gluteus medius, we prevent the knee from caving inward (valgus stress), which protects the medial compartment of the knee where OA usually strikes hardest.
Proprioceptive Training: Improving balance to ensure the muscles fire instantly to protect the joint during unexpected missteps on uneven Toronto sidewalks.
Take Control of Your Joint Health
A diagnosis of osteoarthritis is not a mandate to stop living an active life. Through targeted biomechanical strengthening and interdisciplinary medical care, you can reclaim your mobility and delay or prevent the need for joint replacement surgery.
Book a comprehensive knee assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street in the heart of Queen West.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.

Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:

Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.
Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.
Do I Always Need Physiotherapy for a Rolled Ankle?
Yes. Ignoring a rolled ankle leads to chronic instability and recurring injuries. Physiotherapy restores torn ligaments, rebuilds essential proprioception, and strengthens the surrounding ankle musculature to prevent long-term biomechanical dysfunction and early-onset osteoarthritis.
The Trap of the "Simple" Sprain
"It is just a rolled ankle. I'll walk it off." This is one of the most common and dangerous misconceptions in sports medicine. Whether you rolled it stepping off a curb on Queen Street West, playing a recreational soccer match, or slipping on an icy Toronto sidewalk, an ankle sprain is a severe structural injury.
When patients fail to rehabilitate an ankle sprain, the initial pain and swelling usually subside after a few weeks. However, the underlying mechanical damage remains. Without targeted physiotherapy, the ankle joint heals loosely, leading to a condition known as Chronic Ankle Instability (CAI).
At Rehab Mechanics, we frequently see patients who suffer from recurring ankle sprains, chronic tightness, and early degenerative joint changes simply because they neglected to rehabilitate their very first sprain properly.
Structural Analysis: The Anatomy of a Sprain
To understand why professional rehabilitation is mandatory, we must perform a biomechanical analysis of what exactly happens when an ankle "rolls."
The Lateral Ligament Complex
The vast majority (over 80%) of ankle sprains are "inversion" sprains, meaning the foot rolls inward. This violent motion places catastrophic stress on the lateral ligament complex on the outside of your ankle.
The Anterior Talo-Fibular Ligament (ATFL): This is the weakest and most frequently torn ligament. It stops the foot from sliding forward.
The Calcaneofibular Ligament (CFL): The secondary stabilizer, torn in more severe grade 2 or grade 3 sprains.
The Posterior Talo-Fibular Ligament (PTFL): Rarely torn unless the ankle undergoes massive trauma.
The Neurological Damage: Loss of Proprioception
When you tear a ligament, you do not just tear collagen fibers; you tear specialized nerve endings called mechanoreceptors.
What is Proprioception?
Proprioception is your body's subconscious ability to know where its joints are in space. When you walk on uneven ground, mechanoreceptors in your ankle instantly tell your brain to fire the peroneal muscles on the side of your leg to prevent a roll.
The Delay in Signaling
When an ankle is sprained, these nerve endings are destroyed. Even after the ligament heals structurally, the neurological connection is delayed. Your brain cannot react fast enough to a sudden shift in terrain, virtually guaranteeing you will roll the ankle again. Physiotherapy is the only way to rebuild this neurological pathway.
Primary Source Proof: Proprioceptive Rehabilitation
The clinical literature explicitly states that progressive neuromuscular training is non-negotiable for preventing recurrent ankle injuries.
Note: The link above serves as an example of our commitment to evidence-based practice, referencing standard international clinical guidelines for ankle rehabilitation.
The Rehab Mechanics Treatment Protocol
Restoring a sprained ankle to 100% capacity requires a phased, progressive loading strategy. Passive treatments like ice and compression are only useful for the first 48 hours. After that, active rehab begins.
Phase 1: Acute Management and Mobility (Weeks 1-2)
The goal is to control the swelling while preventing the joint capsule from freezing solid.
Edema Control: Utilizing lymphatic drainage massage and specific taping techniques to flush swelling out of the joint.
Early Range of Motion (ROM): Prescribing pain-free, active movements (like drawing the alphabet with your toes) to align the new collagen fibers correctly as they heal.
Joint Mobilization: Physiotherapists gently glide the talocrural joint to ensure it does not become stiff and restricted.
Phase 2: Muscular Fortification (Weeks 3-6)
Once the acute pain subsides, we must replace the lost stability of the torn ligament with muscular strength.
Peroneal Strengthening: Using resistance bands to heavily strengthen the peroneal muscles on the outside of the calf. These muscles are the body's active defense against rolling the ankle inward.
Calf and Tibialis Anterior Loading: Rebuilding the primary shock absorbers of the lower leg to handle the impact of walking and stairs.
Manual Therapy: Deep tissue release on the calf to prevent compensatory tightness from altering your gait.
Phase 3: Neuromuscular Re-education (Weeks 6+)
This is the phase that prevents the next sprain. We rebuild the brain-to-ankle connection.
Balance Training: Progressing from single-leg standing on solid ground, to standing with eyes closed, to standing on unstable surfaces like a BOSU ball or wobble board.
Dynamic Perturbations: The physiotherapist applies unexpected forces while the patient balances, forcing the nervous system to react instantaneously to stabilize the joint.
Plyometrics and Return to Sport: Incorporating jumping, cutting, and lateral bounding drills to prepare the ankle for the chaotic forces of sports and active living.
Secure Your Foundation in Queen West
An unstable ankle changes the way you walk, which eventually damages your knees, hips, and lower back. Treat the injury correctly the first time.
Book a comprehensive ankle assessment with our clinical team today. We are conveniently located inside the Prime Medical Centre at 68 Abell Street, offering advanced biomechanical care in Toronto.
Contact us to schedule your appointment:
Email: info@rehabmechanics.com
Phone: (416) 533-3900
About the Author
Mr. Sanjay Attwala (B.Sc., M.Sc., RPT) is a Registered Physiotherapist, clinical director, and the founder of Rehab Mechanics in Toronto. With over 15 years of registered clinical practice and a deep specialization in complex musculoskeletal rehabilitation, Sanjay synthesizes rigorous international academic training with advanced evidence-based therapeutics to guide his clinical practice and patient education initiatives.
Academic Background & Credentials
Master of Science (M.Sc.) in Physiotherapy – University of Keele, United Kingdom (2010).
Bachelor of Science (B.Sc.) – University of Waterloo, Ontario, Canada.
Registered Physiotherapist (RPT) – Regulated health professional in excellent standing with the College of Physiotherapists of Ontario (CPO).
Corporate Entity – Operating officially under the S. Attwala Physiotherapy Professional Corporation with a DBA of Rehab Mechanics.
Clinical Expertise & Philosophy
Sanjay’s clinical approach rejects passive symptom management in favor of identifying underlying biomechanical root causes. His diverse expertise spans advanced manual therapies, personalized corrective exercise prescription, and modern physical modalities. At the Rehab Mechanics Toronto Queen West clinic, he routinely diagnoses and treats complex conditions including:
Spinal & Discogenic Pathology – Cervical, thoracic, and lumbar disc injuries, sciatica, and sacroiliac joint (SIJ) dysfunction.
Upper & Lower Extremity Injuries – Rotator cuff tears, frozen shoulder, tennis/golfer’s elbow, carpal tunnel syndrome, and complex ankle/foot pathologies.
Perinatal & Pelvic Health Rehabilitation – Specialized assessment and rehabilitation protocols tailored specifically for women during pregnancy and the post-partum period, addressing pelvic girdle pain, diastasis recti, and core stabilization.
Specialized Rehabilitation – Pelvic health therapy, TMJ dysfunction, post-surgical rehabilitation (including Total Hip and Total Knee Replacements), and custom orthotics dispensing.
Shockwave Therapy: with advanced cutting edge technological devices to suit your needs.
Interdisciplinary Practice & Patient Care
Sanjay practices an integrated model of healthcare, working closely alongside medical doctors inside the Prime Medical Centre on Abell Street to streamline patient recovery pathways. He maintains a human-centric, communication-first clinical framework, ensuring that care remains fully customized rather than automated.
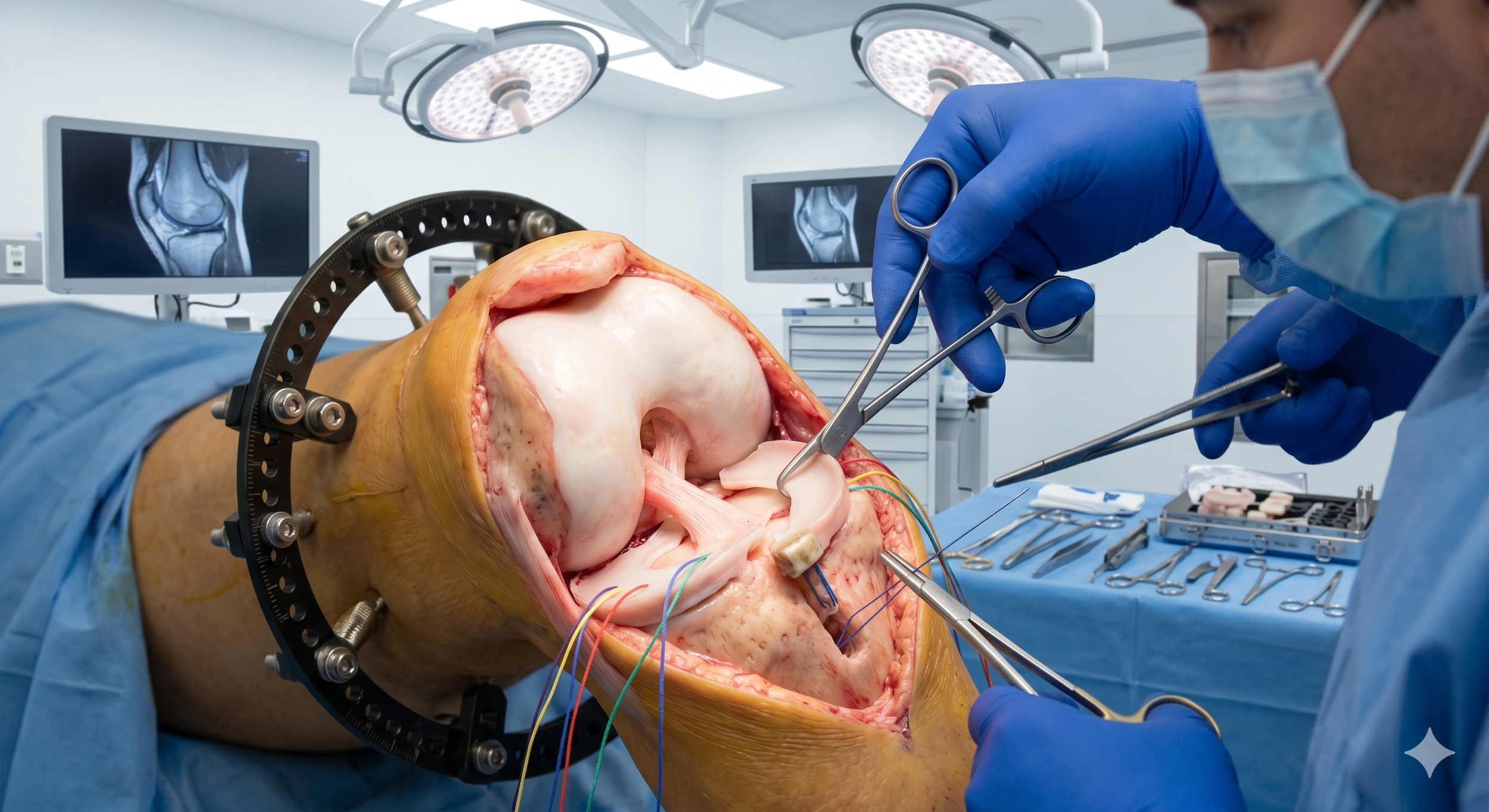
His clinical caseload encompasses a broad operational spectrum under Ontario's regulatory frameworks, including:
Motor Vehicle Accident (MVA) Claims – Rehabilitation navigating Ontario’s statutory accident benefits schedule.
Workplace Safety and Insurance Board (WSIB) – Occupational injury management and return-to-work screening.
Extended Health Care (EHC) & Private Practice – Multi-tier insurance coordination and long-term athletic development plans.

Commitment to Research & Community
Outside of his clinical caseload at Rehab Mechanics and his additional practice affiliations in Etobicoke, Sanjay is an active health writer and community educator. He translates contemporary peer-reviewed medical research into accessible, actionable guidance on his professional blog. As a dedicated father and husband, he mirrors his professional advice in his personal life, focusing on structural mobility, cross-training, and longevity to help his family and his community thrive. Naturally he takes he a keen interest in rehabilitation for women who are pregnant and post-partum.
Disclaimer: The information provided on this blog is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always seek the direct advice of a Registered Physiotherapist, physician, or other qualified health provider regarding any medical condition or physical rehabilitation routine.